
Abstract
Background
Antibodies targeting programmed cell death-1(PD1) and its ligand (PDL1) have revolutionized cancer therapy. However, little is known about the preexisted anti-PD1/PDL1 autoantibodies (AAbs) distribution in multiple cancer types, nor is their potential biomarker role for anti-PD1 therapy.
Method
Plasma anti-PD1/PDL1 AAb IgG and subclasses (IgG1-4) were detected by enzyme-linked immune sorbent assay (ELISA) in 190 cancer patients, covering 10 cancer types (lung, breast, esophageal, colorectal, liver, prostatic, cervical, ovarian, gastric cancers and lymphoma), the comprehensive correlation of AAbs with multiple clinical parameters was analyzed. We further tested these AAbs in 76 non-small cell lung cancer (NSCLC) samples receiving anti-PD1 therapy, the association of AAbs level with survival was analyzed and validated in an independent cohort (n = 32).
Results
Anti-PD1/PDL1 AAb IgG were globally detected in 10 types of cancer patients. IgG1 and IgG2 were the major subtypes for anti-PD1/PDL1 AAbs. Correlation analysis revealed a distinct landscape between various cancer types. The random forest model indicated that IgG4 subtype was mostly associated with cancer. In discovery cohort of 76 NSCLC patients, high anti-PD1 IgG4 was associated with a reduced overall survival (OS, p = 0.019), not progression-free survival (PFS, p = 0.088). The negative association of anti-PD1 IgG4 with OS was validated in 32 NSCLC patients (p = 0.032).
Conclusion
This study reports for the first time the distribution of preexisted anti-PD1/PDL1 AAb IgG and subclasses across 10 cancer types. Moreover, the anti-PD1 AAb IgG4 subclass was identified to associate with OS, which may serve as a potential biomarker for anti-PD1 therapeutic survival benefit in NSCLC patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Programmed cell death-1 (PD1, also known as CD279) is an important immune checkpoint expressed on multiple immune cells and engaged in the regulation of immune homeostasis [1]. Upon binding to its ligands, PD1 ligand-1 (PDL1, also known as B7-H1 or CD274) or PD1 ligand-2 (PDL2, also known as B7-DC or CD273), PD1 induces exhausted T cell immunity against antigens or cancer cells [2]. PDL1 is expressed in a wide range of cell types, including T cells, B cells, dendritic cells, macrophages, mesenchymal stem cells and a broad range of tumor cells. In the tumor microenvironment, lymphocytes frequently express heightened levels of PD1, thus enables blocking the PD1/PDL1 pathway to activate anti-tumor immune responses [3]. Nowadays, disrupting the PD1/PDL1 interaction has made a breakthrough in cancer therapy with remarkable clinical response durability. Six immune checkpoint inhibitors, including three anti-PD1 antibodies Pembrolizumab, Nivolumab, Cemiplimab and three anti-PDL1 antibodies Avelumab, Durvalumab and Atezolizumab [4], have been approved by U.S. Food and Drug Administration (FDA) for the treatment of melanoma [5], non-small cell lung cancer(NSCLC) [6], renal cell carcinoma [7] and many other cancer types. The FDA of China (CFDA) has approved four native anti-PD1 antibodies in recent 3 years (Table 1). Notably, all approved anti-PD1 drugs are IgG4 antibodies, while three anti-PDL1 antibodies are IgG1 form [8].
Autoantibodies (AAbs), kind of antibodies targeting self-antigens, have been robustly detected in cancer patients [9]. The reasons for AAb production are complicated, mainly including altered antigen expression, exposure or presentation (cancer cells express abnormal proteins or overexpress proteins induced by genetic alterations), post-translational modifications (changes in glycosylation, ubiquitination, lipidation, methylation), and abnormal antigen location or structure, as well as the loss of immune tolerance and inflammation [10]. AAb production was found of significance in cancer early detection [11], disease prognosis [12], and therapy response or adverse effect prediction [13], especially for their stability in serum, high specificity and easy to be detected. The human AAbs mainly comprise of IgG, IgM and IgA, among which IgG targets antigen with high avidity and contributes to pathogenic processes induced by cell clearance and signal transduction [10]. There are four AAb IgG subclasses identified: IgG1, IgG2, IgG3 and IgG4 in order of their serum concentrations.
Compared with exogenous anti-PD1/PDL1 antibodies, the distribution and the role of preexisted AAbs against PD1 or PDL1 in cancer patients are unknown. A study has detected AAb against B7-H1(PDL1) in rheumatoid arthritis(RA) patients and indicated anti-PDL1 IgG was able to costimulate the proliferation of T cells in vitro [14]. Another study indicated that AAbs against PD1 existed in sera of type 1 autoimmune hepatitis (AIH) patients may be used as a diagnostic marker for discriminating AIH from other liver disorders and healthy people [15]. In systemic lupus erythematosus (SLE) patients, the results revealed that anti-PD1 IgG is associated with disease activity [16]. Our previous work has assessed anti-PD1 AAb and anti-PDL1 AAb in sarcoma, lung cancer and lymphoma patients, the results indicated that the IgG1, IgG2 are the major types for anti-PD1 AAb and anti-PDL1 AAb in lymphoma patients [17]. Although the production of serum anti-PD1 IgG or anti-PDL1 IgG has been reported individually in autoimmune diseases or cancer patients, no study has systematically investigated their IgG and subclass distribution in a broad spectrum of cancer types. Moreover, little is known about the association of self-active anti-PD1 AAb and anti-PDL1 AAb with clinical parameters and their role in immunotherapy.
In this study, we set out to identify circulating anti-PD1 AAb, anti-PDL1 AAb and their subclass distribution in 10 types of cancers (lung, breast, esophageal, colorectal, liver, prostatic, cervical, ovarian, gastric cancers and lymphoma). Moreover, the relationship between preexisted AAbs and the survival of NSCLC patients treated with anti-PD1 therapy was investigated.
Materials and methods
Study design and patient characteristics
Plasma samples from a total of 298 cancer patients were retrospectively collected between August 2015 and July 2021 in National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, including 190 patients without anti-PD1 therapy which consists of 28 lung cancer, 18 breast cancer 18 esophageal cancer, 18 colorectal cancer, 18 liver cancer, 18 prostatic cancer, 18 cervical carcinoma, 18 ovarian cancer, 18 gastric cancer and 18 lymphoma. For 108 NSCLC patients receiving anti-PD1 therapy, 76 patients were distributed as discovery cohort, 32 patients were included in the validation cohort. All plasma samples were centrifuged for 10 min at 16,000 g and 4 °C, the supernatant was stored in 1.5 ml cryovials at − 80 °C and thawed once at the time of the testing. Clinical information and the demographic characteristics of patients are shown in Supple Table S1 and Supple Table S2. A total of 83 clinical parameters were obtained from the electronic medical system, including complete blood count, the comprehensive metabolic panel, coagulation function test and virus infection test (Supple Table S3).
This study was approved by the Ethics Committee of the National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Peking Union Medical College and the Chinese Academy of Medical Sciences (Permission No. 19–019/1804). All experiments were executed according to the Declaration of Helsinki.
Detection of anti-PD1/PDL1 AAb IgG and subclasses using ELISA
The ELISA assay was performed in duplicate to detect anti-PD1/PDL1 AAb IgG and subclasses. First, PD1/PDL1 protein (Sino Biological, Beijing, China) at 1 ng/uL in 0.2 mol/L sodium bicarbonate buffer (pH 9.4) was added to individual wells of 96-well ELISA plates (Corning Inc, NY). After coating overnight at 4 °C, remove the coating solution and block the plate with 5% milk in PBST at room temperature for 1 h, in parallel, the plasma samples were thawed on ice and diluted 1:300 for IgG detection and 1:25 for subclass detection with 5% milk in PBST and then incubated the coated plate with diluted plasma for 1 h at room temperature. After washing the plate three times with PBST solution, add HRP-conjugated anti-human IgG antibody (Jackson ImmunoResearch Laboratories, PA, USA) for 1 h for anti-PD1/PDL1 AAb IgG detection, HRP-conjugated anti-human IgG1-4 antibodies were used to detect the distribution of IgG subclasses in plasma. Tetramethyl benzidine (TMB) substrate (ComWin Biotech, Beijing, China) was then added for 15 min. Sulfuric acid was used to stop the reaction. The signal was assessed using an Infinite F50 plate reader (TECAN, Männedorf, Switzerland) at 450 nm.
The ELISA signal of AAb IgG was normalized using the OD450 of the samples minus the median OD450 of negative controls, IgG subclasses were normalized by OD450 of the samples divided by median OD450 of negative controls.
Statistical analysis
The Mann–Whitney U test was used to identify differently produced AAbs between ten cancer types; for multiple comparisons, p value was adjusted by the Bonferroni method, and p value < 0.05 was statistically significant for all the tests. The correlation between anti-PD1/PDL1 AAb IgG and the clinical parameters was analyzed with Spearman correlation (plotted with R). The random forest model and survival analysis were performed in R version 3.6.3.
Results
Global detection of anti-PD1 and anti-PDL1 AAb IgG in 10 types of cancer patients
We used ELISA to assess anti-PD1 AAb IgG and anti-PDL1 AAb IgG in a total of 190 patients involving 10 types of cancers (Supple table S1). There was a significant correlation of AAb testing signals in intro experiments (r = 0.98, Supple figure S1A) and inter experiments (r = 0.97, Supple figure S1B), the average CVs in batch and between batches were 4% and 7%, respectively, indicating good reproducibility of our self-prepared ELISA method.
The preexisted anti-PD1 and anti-PDL1 AAb IgG can be detected in the plasma of 10 types of cancer patients, non-hierarchical clustering analysis indicated that the IgG subclasses clustered differently from each other, demonstrating the distinct function of these AAb families in cancer patients (Fig. 1A), while the heatmap by cancer types showed no obvious distribution difference (Supple figure S2). For anti-PD1 IgG, the concentration in colorectal cancer and esophageal cancer was lower, while the breast cancer and ovary cancer owed a high production level (Fig. 1B), only the production between colorectal cancer and ovary cancer showed statistical significance (p = 0.03, Supple table S4). The anti-PDL1 AAb IgG in colorectal cancer, cervical cancer and lymphoma was relatively low produced compared to liver cancer and breast cancer (Fig. 1B), while no statistical significance was reached in multiple comparisons (Supple table S4).

Global detection of anti-PD1 and PDL1 autoantibody IgG in 10 types of cancer patients. A Clustering of anti-PD1 and anti-PDL1 AAb in 10 types of cancer patients, the heatmap was executed using z-score normalization. B and C show anti-PD1/PDL1 IgG and IgG subclass distribution in 10 types of cancer patients, respectively. LC: lung cancer, GC: gastric cancer, CC: colorectal cancer, LiC: liver cancer, BC: breast cancer, EC: esophageal cancer, CeC: cervical carcinoma, ML: lymphoma, PC: prostatic cancer, OC: ovarian cancer. The median IgG level is plotted for each cancer type, * represents p < 0.05
We further compared each subclass of anti-PD1 and anti-PDL1 IgG across different cancer types, the IgG1 of anti-PD1 and anti-PDL1 AAb was highest in breast and esophageal cancer, respectively (Fig. 1C, Supple table S5). Of the IgG2 subclass, anti-PDL1 IgG2 in prostate cancer was higher than the value in lung cancer (p = 0.024), there was no significant distribution difference for anti-PD1 IgG2 across different cancer types (Fig. 1C, Supple table S5). Of the IgG3 subclass, anti-PD1 IgG3 in esophageal cancer was higher than that of colorectal cancer (p = 0.041), while anti-PDL1 IgG3 showed no significance across different cancer types (Fig. 1C, Supple table S5). The anti-PD1 IgG4 in esophageal cancer was higher than ovarian cancer (p = 0.008), the anti-PDL1 IgG4 in ovarian cancer was higher than that in cervical cancer (p = 0.010) (Fig. 1C, Supple table S5).
Anti-PD1/PDL1 IgG subclass distribution in 10 types of cancer patients
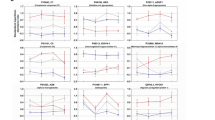
The normalized levels for anti-PD1 IgG1, IgG2 subclasses were significantly higher than values of IgG3 and IgG4 in colorectal cancer, esophageal cancer, liver cancer, gastric cancer and ovarian cancer(p < 0.05, Fig. 2A, Supple table S6). In lung cancer and breast cancer, IgG1 subclass was higher than IgG4, while no significance was observed between IgG2 and IgG3, IgG4 subclasses (Fig. 2A, Supple table S6). In cervical cancer and prostate cancer, the mean ODs of anti-PD1 IgG2 were significantly higher than IgG3 and IgG4 subclasses; however, IgG1 was not significantly highly detected(Fig. 2A, Supple table S6).

Anti-PD1/PDL1 IgG subclass distribution in nine types of cancer patients. A and B show anti-PD1 and anti-PDL1 IgG subclass distribution in colorectal cancer, esophageal cancer, liver cancer, gastric cancer, ovarian cancer, lung cancer, breast cancer, cervical carcinoma and prostatic cancer. The median level is plotted for each subclass type. The up and down edges of the boxes correspond to the 25th and 75th percentiles. *,**,***,**** represent p < 0.05, < 0.01, < 0.001, < 0.0001. ns: not significant
For the anti-PDL1 IgG subclass, we found that in colorectal cancer, IgG1 and IgG2 subclasses were significantly higher than IgG3 and IgG4 (p < 0.05, Fig. 2B, Supple table S7). The anti-PDL1 IgG1 was found highly produced in the other two cancer types including lung cancer, esophageal cancer (p < 0.05, Fig. 2B, Supple table S7). In the remaining cancer types, IgG2 was with the highest level (Fig. 2B, Supple table S7). Along with lymphoma subclass distribution in our previous work[17], our results demonstrated that IgG1 and IgG2 were revealed to be the major subtypes for anti-PD1 and anti-PDL1 IgG.
Correlation analysis of anti-PD1/PDL1 IgG subclasses with clinical data
We performed a comprehensive correlation analysis of clinical and laboratory information with AAbs levels, the results displayed distinct patterns in various cancer types (Fig. 3). C-reactive protein (CRP) reflecting increased inflammation was clustered with variables in liver function, thus suggesting the association between these variables. Adenosine deaminase (ADA) is an enzyme participated in purine metabolism and was first found involved in the development and maintenance of the immune system[18].The ADA was found positively correlated with anti-PD1/PDL1 IgG3, IgG2, IgG1 in lung cancer, colorectal cancer and ovarian cancer, respectively. In liver cancer, the HBV infection is a risk factor, the results showed that HBsAg was correlated with anti-PD1 IgG4 and anti-PD1/PDL1 IgG3, the correlation between HBV infection and anti-PD1 IgG3 was also found in lymphoma. Other correlations were also investigated between clinical data with AAb subtypes, e.g., anti-PD1/PDL1 IgG2 with MCV, MCHC in gastric cancer, anti-PD1/PDL1 IgG4 with blood lipid in colorectal cancer, anti-PD1/PDL1 IgG4 with coagulation function in esophageal cancer. Our results demonstrated that in different cancer types, there may be distinct interactions between AAbs with clinical parameters.

Correlation analysis of AAb with clinical data in 10 types of cancer patients. The correlations of multiple clinical parameters including complete blood count, the comprehensive metabolic panel, coagulation function test, virus infection test and AAb levels were analyzed. The cluster method was ward.D2. Blue and red indicate a negative and positive correlation, respectively. Framed black boxes represent highly positive correlations between AAbs and clinical variables
Random forest model for clinical relevance with different cancer types
The distinct distribution pattern in various cancer types suggests that it is possible to explore the most relevant AAb and clinical data with cancer types. We first randomly assigned these cancer patients into training (70%) and validation (30%) groups. The random forest was used to select features among multiple clinical data and AAb levels to construct decision trees (Fig. 4A), the bootstrap procedure improves model performance because it decreases the variance of the model, without increasing the bias, at last, the classification was made by taking the majority vote among trees [19]. In liver cancer, cervical cancer and lymphoma, the random forest model based on clinical data and AAbs showed the best consistency, with 60%, 60%, 89% accuracy in the training group, 83%, 83% and 50% accuracy in the validation group (Fig. 4B). The top ten variables most relevant with cancer types were Age, HBsAg, PD1-IgG4, Sex, MONO-number, SOD, PDL1-IgG4, NEUT-number, HCY, PD1-IgG3(Fig. 4C), indicating the association of these parameters with cancer, the detailed interaction procedure in cancer of AAbs such as PD1/PDL1-IgG4 and PD1-IgG3 remained to be illustrated.

Classification model for different cancer types using random forest. A The model scheme by random forest, different distribution of clinical data and AAb in various cancer types make it possible for stratification, after random setting of 7:3 in training and validation groups, random forest was used for classification. The circles in different colors represent different types of cancer. B Predictive accurancy for each cancer type. The blue circle indicates the percentage of classify accurancy. C The top thirty important factors in random forest, the top ten was framed in red
Predictive value of anti-PD1 IgG4 in NSCLC with anti-PD1 therapy
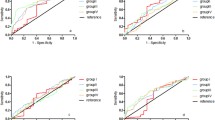
Our results indicated that PD1/PDL1-IgG4 and PD1-IgG3 levels are associated with cancers, but whether they had an effect on anti-PD1 immunotherapy remains unknown. We examined these AAb baseline levels in 76 NSCLC patients with anti-PD1 therapy, analyzed the correlation of the AAb levels with progression-free survival (PFS) and overall survival (OS). Kaplan–Meier survival curves demonstrated that low anti-PD1 IgG4 level displayed a favorable, albeit not statistically significant PFS in NSCLC patients (Fig. 5A; p = 0.088), and correlated with OS with a p value of 0.019 (Fig. 5B). No significant correlation was observed between anti-PD1 IgG, IgG1, IgG2, and IgG3 with PFS or OS (Fig. 5C–F). The anti-PDL1 IgG and subclasses showed no significant association with patients’ survival with anti-PD1 treatment (Supple figure S3). We further validated the association in an independent cohort of 32 NSCLC patients, and the results showed that patients with low anti-PD1 IgG4 obtained a longer OS time(p = 0.031), but not PFS(p = 0.6) (Fig. 6).

Correlation of anti-PD1 IgG and subtypes with survival in discovery cohort (n = 76). A and B show the correlation of anti-PD1 IgG4 with progression-free survival (PFS) and overall survival(OS), respectively. PFS and OS analyses of patients with different anti-PD1 IgG (C), anti-PD1 IgG1 (D), anti-PD1 IgG2 (E) and anti-PD1 IgG3 (F) contents at baseline. All the variables are splitted into two groups by putting all cases that are below the median into a “low” group and all cases that are above or equal to the median into a “high”group

Correlation of anti-PD1 IgG4 with survival in validation cohort (n= 32). A and B show the correlation of anti-PD1 IgG4 with progression-free survival (PFS) and overall survival (OS), respectively. All the variables are splitted into two groups by putting all cases that are below the median into a “low” group and all cases that are above or equal to the median into a “high”group
Discussion
Immune checkpoint inhibitors, especially antibodies targeting PD1/PDL1, have dramatically changed the landscape of cancer treatment. Besides these effective ectogenous antibodies, there are a wide range of AAbs existed in cancer patients. This study reported for the first time anti-PD1 AAb and anti-PDL1 AAb in 10 cancer types, the results indicated that IgG1 and IgG2 are the major subclasses, the comprehensive analysis indicated an association between multiple clinical data with AAbs, especially IgG4 subtype. Moreover, a high anti-PD1 IgG4 level correlated with poor prognosis, which may serve as a potential biomarker for the long time survival of anti-PD1 therapy.
AAbs globally exist in cancer patients, more than 2000 serologically positive AAbs were detected using protein arrays [20]. The AAb production was considered to correlate with protein altered expression, mutation or immune tolerance et. al, thus AAb detection was capable to reflect the tumor status or immune ability. A combination of several AAbs will improve the diagnostic specificity and sensitivity, a panel of 7 AAbs(p53, NY-ESO-1, CAGE, GBU4-5, SOX2, MAGEA4, and HuD) has been approved as an aid for early detection of lung cancer in people with high risk [21]. Though multiple AAbs have been reported as diagnostic or prognostic factors, little is known about anti-PD1 AAb or anti-PDL1 AAb. Our previous work has assessed these two AAbs in NSCLC, lymphoma and sarcoma [17]. In this study, we expanded to test anti-PD1 AAb and anti-PDL1 AAb in 10 cancer types of high incidence, including lung cancer, breast cancer, esophageal cancer, colorectal cancer, liver cancer, prostatic cancer, cervical carcinoma, ovarian cancer, gastric cancer and lymphoma. The results showed anti-PD1 AAb and anti-PDL1 AAb can be globally detected in these cancer patients. The Cancer Genome Atlas (TCGA) database reported RNA-seq data of PDCD1(PD1)and CD274(PDL1) in 17 cancer types, indicating the universe mRNA expression in cancer tissues [22]. Anti-PDL1 AAb in lymphoma is relatively low among 10 cancer types, while our previous study revealed that anti-PDL1 AAb in lymphoma is higher than NSCLC and sarcoma, this inconsistency may because we include non-Hodgkin` lymphoma in this study, while patients were mainly Hodgkin`s lymphoma in the previous study. These results further demonstrated that different histology types of the same cancer may have various AAb levels, thus a further study of different subtypes of cancers is warranted.
Of the IgG subclasses, although they are more than 90% identical on the amino acid level, each IgG subclass has a unique profile referring to structure, antigen binding, immune complex formation, complement reduction, the binding affinity of Fc receptor, half-life, and placental transport [23]. For each AAb, the distribution of subclasses may be different. Among antibodies against cyclic citrullinated peptides (CCP) and citrullinated vimentin (MCV), IgG1 and IgG4 were predominant subclasses in RA patients [24]. For Anti-myeloperoxidase (MPO) IgG subclass, IgG1 and IgG4 were detected to be major subclasses in vasculitis patients [25]. IgG1, IgG2 and IgG4 are predominant for proteinase 3 (PR3) -ANCA IgG in Wegener’s granulomatosis patients [26]. For anti-HBe, IgG1 and IgG4 were significantly higher than IgG2 and IgG3 [27]. Our study indicated IgG1 and IgG2 are the major types for anti-PD1 AAb and anti-PDL1 AAb in cancer patients. These may be explained that antibodies toward soluble protein antigens and membrane proteins primarily trigger IgG1, also accompanied by lower levels of other subclasses [28].
Moreover, we found distinct correlations existed between AAbs with multiple clinical parameters, especially the IgG4 subtype. IgG4 is known to bind and activate FcgRIa, all approved antibodies targeting PD1 by FDA are IgG4 form (Table1), antibody drugs were designed to be IgG4 types to avoid antibody-dependent cellular cytotoxicity (ADCC) or complement-dependent cytotoxicity (CDC) effect [29]. Interestingly, we found and validated a high level of anti-PD1 AAb IgG4 correlated with poor prognosis, which demonstrated that anti-PD1 AAb may influence the effect of anti-PD1 therapy. However, the detailed mechanisms or structure of AAb should be investigated further. Besides, the approved anti-PDL1 antibodies are IgG1 subtypes, whether there is an interaction between preexisted anti-PDL1 AAb IgG1 with anti-PDL1 therapy should be investigated in the future.
Despite these impressive results, there are several limitations in this study. The number of each cancer type was limited, thus the correlation of AAb subclasses with clinical parameters should be investigated in a larger cohort. More functional studies on AAbs and their interaction with antibody drugs remain to be implemented.
In conclusion, this study reports for the first time the distribution of preexisted anti-PD1/PDL1 AAbs and their subclasses in a wide range of cancer types. Moreover, anti-PD1 IgG4 was identified and validated to associate with survival of anti-PD1 therapy, it may serve as potential biomarker to predict anti-PD1 therapeutic survival in NSCLC and guide anti-PD1 treatment for cancer patients.
References
Topalian SL, Drake CG, Pardoll DM (2015) Immune checkpoint blockade: a common denominator approach to cancer therapy. Cancer Cell 27:450–461
Harel M, Ortenberg R, Varanasi SK, Mangalhara KC, Mardamshina M, Markovits E et al (2019) Proteomics of melanoma response to immunotherapy reveals mitochondrial dependence. Cell 179(1):236–250
Wei SC, Duffy CR, Allison JP (2018) Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov 8:1069–1086
Singh S, Hassan D, Aldawsari HM, Molugulu N, Shukla R, Kesharwani P (2020) Immune checkpoint inhibitors: a promising anticancer therapy. Drug Discov Today 25:223–229
Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R et al (2013) Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med 369:134–144
Peters S, Kerr KM, Stahel R (2018) PD-1 blockade in advanced NSCLC: a focus on pembrolizumab. Cancer Treat Rev 62:39–49
Motzer RJ, Rini BI, McDermott DF, Redman BG, Kuzel TM, Harrison MR et al (2015) Nivolumab for metastatic renal cell carcinoma: results of a randomized phase II trial. J Clin Oncol 33:1430–1437
Lee HT, Lee SH, Heo YS (2019) Molecular interactions of antibody drugs targeting PD-1, PD-L1, and CTLA-4 in immuno-oncology. Molecules 24(6):1190
Fridman WH, Pages F, Sautes-Fridman C, Galon J (2012) The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer 12:298–306
Zaenker P, Gray ES, Ziman MR (2016) Autoantibody production in cancer-the humoral immune response toward autologous antigens in cancer patients. Autoimmun Rev 15:477–483
Anderson KS, Sibani S, Wallstrom G, Qiu J, Mendoza EA, Raphael J et al (2011) Protein microarray signature of autoantibody biomarkers for the early detection of breast cancer. J Proteome Res 10:85–96
Song E, Oh HS, Jeon MJ, Chung KW, Hong SJ, Ryu JS et al (2019) The value of preoperative antithyroidperoxidase antibody as a novel predictor of recurrence in papillary thyroid carcinoma. Int J Cancer 144:1414–1420
Toi Y, Sugawara S, Sugisaka J, Ono H, Kawashima Y, Aiba T et al (2019) Profiling preexisting antibodies in patients treated with anti-PD-1 therapy for advanced non-small cell lung cancer. JAMA Oncol 5:376–383
Dong H, Strome SE, Matteson EL, Moder KG, Flies DB, Zhu G et al (2003) Costimulating aberrant T cell responses by B7–H1 autoantibodies in rheumatoid arthritis. J Clin Investig 111:363–370
Matsumoto K, Miyake Y, Matsushita H, Ohnishi A, Ikeda F, Shiraha H et al (2014) Anti-programmed cell death-1 antibody as a new serological marker for type 1 autoimmune hepatitis. J Gastroenterol Hepatol 29:110–115
Shi H, Ye J, Teng J, Yin Y, Hu Q, Wu X et al (2017) Elevated serum autoantibodies against co-inhibitory PD-1 facilitate T cell proliferation and correlate with disease activity in new-onset systemic lupus erythematosus patients. Arthritis Res Ther 19:52
Tan Q, Wang D, Yang J, Xing P, Yang S, Li Y et al (2020) Autoantibody profiling identifies predictive biomarkers of response to anti-PD1 therapy in cancer patients. Theranostics 10:6399–6410
Wilson DK, Rudolph FB, Quiocho FA (1991) Atomic structure of adenosine deaminase complexed with a transition-state analog: understanding catalysis and immunodeficiency mutations. Science 252:1278–1284
Dietterich TG (2000) An experimental comparison of three methods for constructing ensembles of decision trees: bagging, boosting, and randomization. Mach Learn 40:139–157
Li Y, Li CQ, Guo SJ, Guo W, Jiang HW, Li HC et al (2020) Longitudinal serum autoantibody repertoire profiling identifies surgery-associated biomarkers in lung adenocarcinoma. EBioMedicine 53:102674
Lam S, Boyle P, Healey GF, Maddison P, Peek L, Murray A et al (2011) EarlyCDT-Lung: an immunobiomarker test as an aid to early detection of lung cancer. Cancer Prev Res (Phila) 4:1126–1134
Hutter C, Zenklusen JC (2018) The cancer genome atlas: creating lasting value beyond its data. Cell 173:283–285
de Taeye SW, Rispens T, Vidarsson G (2019) The ligands for human IgG and their effector functions. Antibodies (Basel) 8(2):30
Engelmann R, Brandt J, Eggert M, Karberg K, Krause A, Neeck G et al (2008) IgG1 and IgG4 are the predominant subclasses among auto-antibodies against two citrullinated antigens in RA. Rheumatology (Oxford) 47:1489–1492
Akbay EA, Koyama S, Liu Y, Dries R, Bufe LE, Silkes M et al (2017) Interleukin-17A promotes lung tumor progression THROUGH neutrophil attraction to tumor sites and mediating resistance to PD-1 blockade. J Thorac Oncol 12:1268–1279
Liu Y, Liao XW, Qin YZ, Mo XW, Luo SS (2020) Identification of F5 as a prognostic biomarker in patients with gastric cancer. Biomed Res Int 2020:9280841
Wang L, Tsai TH, Huang CF, Ho MS, Lin DB, Ho YC et al (2007) Utilizing self-prepared ELISA plates for a cross-population study of different anti-HBe IgG subclass profiles. J Med Virol 79:495–502
Vidarsson G, Dekkers G, Rispens T (2014) IgG subclasses and allotypes: from structure to effector functions. Front Immunol 5:520
Yu J, Song Y, Tian W (2020) How to select IgG subclasses in developing anti-tumor therapeutic antibodies. J Hematol Oncol 13:45
Acknowledgements
This work was supported by the China National Major Project for New Drug Innovation (2017ZX09304015, 2019ZX09201-002), Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (CIFMS)( 2021-1-I2M-003) and National Natural Science Foundation of China(81972805).
Author information
Authors and Affiliations
Contributions
YKS and XHH concepted, designed and supervised the study. YKS, XHH, LYD, QYT, YRW, SXL, RRL, SSW, NL, HZC, YXT, YZ, QFZ, JLY, PYX, XSH, YTL, SYZ, JRY, DW, ZSZ and LT collected the plasma samples and clinical information. QYT, YRW and TL collected the data. QYT, LYD, YKS, XHH and XBY analyzed and interpreted the data. QYT, LYD, TL and NL did the statistical analysis. TQY and LYD wrote the manuscript, YKS and XHH revised the manuscript. All authors reviewed the manuscript and approved the final version to submission.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Tan, Q., Dai, L., Wang, Y. et al. Anti-PD1/PDL1 IgG subclass distribution in ten cancer types and anti-PD1 IgG4 as biomarker for the long time survival in NSCLC with anti-PD1 therapy. Cancer Immunol Immunother 71, 1681–1691 (2022). https://doi.org/10.1007/s00262-021-03106-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00262-021-03106-z