
Abstract
A wide variety of tumor antigens have been targeted in cancer immunotherapy studies. Traditionally, the focus has been on commonly overexpressed antigens shared across many patients and/or tumor types. As the field has progressed, the identity of human tumor rejection antigens has broadened. Immunologic monitoring of clinical trials has slowly elucidated candidate biomarkers of immune response and clinical response, and conversely, of immune dysfunction and suppression. We have utilized MART-1/Melan-A in our melanoma studies and observed a high frequency of immune responses and several significant clinical responses in patients vaccinated with this melanosomal protein. Alpha-fetoprotein is a shared, overexpressed tumor antigen and secreted glycoprotein that we have tested in hepatocellular cancer vaccines. Our recent studies have identified immunosuppressive and immune-skewing activities of this antigen. The choice of target antigen and its form can have unexpected effects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cancer vaccination is designed to promote antitumor immunity. A substantial amount of preclinical model data supports the central importance of cytotoxic T lymphocytes (CTL) in effective antitumor immunity to promote the lysis of tumor cells. Many cancer vaccines are designed to activate CTL using many forms of antigens [1] including MHC-restricted peptide epitopes, long peptides, proteins, and cDNAs. The targeted tumor antigens are formulated with adjuvants of many kinds and administered as peptides, proteins, DNA, recombinant viral vectors, and autologous or allogeneic cells. In many trials, the majority of patients are successfully vaccinated, even to non-mutated self-antigens.
Many cancer vaccine clinical trials have shown dramatic tumor regressions in a minority of patients (5–10 %), and some large studies have shown significant trends in improved outcomes for successfully vaccinated patients. However, there have also been many negative studies with minimal immunogenicity and without evidence of therapeutic efficacy. To date, there are no biomarkers of a successful vaccine that can invoke potent antitumor immunity. There are no biomarkers yet for patients who will respond immunologically or clinically, nor for the exact type of CTL immune response (or other type of response) needed to elicit a significant clinical response. The field continues to move forward slowly, testing different vaccine strategies and, more recently, combinations of vaccine elements with other types of therapies (e.g., engineered allogeneic cells and recombinant bacteria) and combinations with newly approved checkpoint blockades, standard of care, etc. [2].
A number of different types of antigens have been tested in clinical trials [3, 4]. Some are considered “tumor-associated” antigens (TAA) that include non-mutated self-antigens that are differentially expressed by tumors, and “tumor-specific” antigens (TSA) that include mutated and viral antigens. Several examples are shown in Table 1. Among the first characterized were those recognized by tumor-infiltrating lymphocytes (TIL) in melanoma tumors, including melanoma antigen family A1 (MAGE-A1) and melanoma antigen recognized by T cells (MART-1)/aka Melan-A. Some are more immunogenic and widely tested than others (MART-1, NY-ESO-1), and recent studies indicate that the most potent target antigens may be the patient-specific mutated antigens [4].
Our group has tested cancer vaccines in both melanoma and hepatocellular cancer (HCC), starting in 1996. In melanoma, we have tested MART-1, and in HCC, we have focused on alpha-fetoprotein (AFP). This series of studies focused on these shared, non-mutated antigens known to be highly upregulated in the majority of the two tumor types examined.
Discussion
Melanoma vaccine background
Melanoma is the deadliest form of skin cancer and has an annual global incidence of 132,000 cases per year. Our melanoma vaccine trials tested dendritic cell (DC)-based vaccines, initially pulsed with a single HLA-A2-restricted MART-1 epitope (MART-127–35 AAGIGILTV), and subsequently transduced with a recombinant adenovirus (AdV) encoding the full-length MART-1 cDNA [5–7]. We wanted to take advantage of the potent immune stimulatory nature of DC to promote melanoma-specific immunity. DC are known to both initiate immunity and shape the quality of the response. DC vaccines, prepared by 3- to 7-day in vitro culture of peripheral blood monocytes in GM-CSF and IL-4 cytokines, have been tested in many trials, for many different tumor types, loaded with many different antigens. We found that the majority of patients could be successfully vaccinated with MART-1 in all three trials, resulting in increased frequencies of circulating MART-1-specific CD8+ CTL and CD4+ T cells by MHC tetramer and/or IFNγ ELISPOT assays.
Observations from immune monitoring
Importantly, no measure of MART-1-specific T cell reactivity correlated with clinical outcome including IFNγ ELISPOT, intracellular cytokine staining for IFNγ and IL-4, MHC tetramer frequency or cytotoxicity after in vitro stimulation. These assays did identify vaccinated patients and suggested the dose of DC and route of administration resulting in higher T cell frequencies. Because there are many other well-characterized shared tumor antigens in melanoma, we also tested for spontaneous development of immunity to antigens not delivered in the vaccine, or determinant spreading [8]. This antigen spreading phenomenon was originally characterized in the setting of autoimmunity.
In each of these studies, the patients with the most favorable clinical outcomes exhibited antigenically broader immune responses to include gp100 and tyrosinase-specific CD8+ and CD4+ T cells, in addition to MART-1. We are not the only group to detect this; there were also reports from others who also observed this phenomenon [9, 10]. These data suggest that a potential biomarker of more effective antitumor immunity is a broad CD8+ and CD4+ T cell response to many different tumor antigens. It may also suggest that in vivo cross-presentation and determinant spreading from vaccine-delivered antigens to other antigens expressed by the tumor may be a mechanism to promote immunity to private, patient-specific mutated antigens. Such mutation-specific T cells may be the most effective, clinically relevant antitumor effector cells due to the increased likelihood of harnessing high-avidity T cells which have not undergone negative selection.
Building on the lessons learned
Based on the data suggesting that broader immunity is important and that promotion of in vivo cross-presentation may result in more effective antitumor immunity, we designed a new DC vaccine to activate a more effective polyclonal response with the vaccine. We retained the AdV as the vector providing the tumor antigens (as genes) for several reasons: It allows for efficient gene transfer of the antigen cDNAs into human DC and allows for long-term transgene expression (7–10 days in vitro) [11–13]. It is not affected by systemic neutralizing anti-AdV antibodies (as shown earlier in a mouse model) [14] and can have positive maturation effects on human DC (promoting a slightly more mature phenotype and altering the cytokine production profile) [15]. When compared head to head, AdV-mediated antigen transfer shows superior T cell activation when compared directly to peptide-pulsed DC [16, 17]. By expressing full-length antigen, AdV-engineered DC activate CD8+ and CD4+ T cells simultaneously [13, 16, 18] and promote chemokine secretion (and subsequent NK cell migration) [19, 20]. It also allows for simultaneous activation of high-frequency type 1-skewed virus-specific memory CD8+ and CD4+ T cells, regardless of circulating anti-AdV antibody status [21].
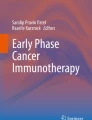
Based on human in vitro preclinical data [17], we designed the current trial to test a more broadly immunogenic DC vaccine that could promote in vivo cross-presentation and determinant spreading because it is engineered with three full-length, defined, tumor antigens to activate multiple CD8+ and CD4+ T cell clones (Fig. 1). We identified a maturation cocktail (LPS + IFNγ) specifically matched to AdV transduction signals that more potently activate T cells in vitro. We also showed that the vaccine could activate innate immunity by secreting chemokines which induce NK cell migration and activation [19, 20]. Lastly, we added an immune boost with one month of systemic high-dose IFNα which has been shown to promote endogenous DC skewing to type 1 function, improved in vivo cross-priming and to have direct positive effects on T cells [22, 23].

Diagram of the melanoma antigen-engineered DC vaccine trial is presented. Top The diagram depicts the vaccine of autologous DC engineered with the recombinant AdV and lists some of the immunologic monitoring underway. Middle The intervention schedule is shown. Bottom The recombinant adenoviral vector map is shown
In this ongoing trial, one goal was to observe improved clinical outcomes compared to previous DC vaccines (>7 % complete and partial responses). There are many junctures at which DC vaccines may not be sufficiently potent, including in their ability to activate type 1-skewed effector T cells, activate effector cells that can traffic to and fully infiltrate tumors, activate cells that can resist the suppressive tumor microenvironment, and retain their activity. The other goal was to gain substantial biomarker data about the patients’ tumors, their immune responses, and their DC vaccines. By learning about the vaccine biology, responding and non-responding tumors, and the immune responses to multiple tumor antigens (vaccine encoded and AdV vector) and the innate immune response, these data should help to move the vaccine field forward.
Hepatocellular carcinoma (HCC) vaccines
Hepatocellular cancer (HCC) is the second highest cause of global cancer deaths. HCC has increased 62 % in the last 20 years to over 750,000 new cases globally and over 35,000 new US cases every year [24, 25]. In the USA, hepatitis B and C viruses (HBV, HCV) and alcoholic cirrhosis are leading causes, and metabolic syndromes are also increasing HCC. While a minority of patients is eligible for curative surgery or transplantation, many patients will recur.
Immunologically, the liver is a tolerogenic organ [26] with inherently non-stimulatory antigen presentation function. HCC patients also exhibit significant systemic immune suppression. Several recent reports have documented high frequencies of circulating regulatory T cells (Treg) and myeloid-derived suppressor cells (MDSC), as well as defects in natural killer (NK) cell function in HCC patients [27]. A greater understanding of the multiple mechanisms of HCC-mediated immune suppression and immune modulation will lead to new approaches to combat these defects. Both adequate immune function and controlled immune suppression are critical for effective antitumor immunity, including the immunity that can be induced by radiofrequency ablation, surgery, vaccines, and checkpoint blockade.
We have studied the HCC-secreted oncofetal antigen AFP, which is produced by over 50 % of HCC tumors, as a target for cancer vaccines. More recently, we have investigated the multiple immunosuppressive mechanisms of AFP. AFP secretion by tumors is correlated with poorer patient outcomes [28], increased tumor growth, and tumor stem cell-like properties [29, 30], indicating it is more than a “passenger” protein in tumors.
Alpha-fetoprotein
An oncofetal protein synthesized in the yolk sac and fetal liver, AFP is the most abundant serum protein in the fetus [31]. AFP is transcriptionally repressed shortly after birth, and normal adult levels range between 1 and 40 ng/ml. Elevated AFP levels in the circulation of adults are associated with liver regeneration, hepatitis, chronic liver diseases, and malignant growth [29]. Various glycoforms of AFP have been identified in the serum of HCC patients [32]. The fucosylated variant AFP-L3 is the major glycoform found in individuals with HCC and is associated with poor prognosis. While cord blood-derived normal AFP (nAFP) contains <5 % of the fucosylated variant, >80 % of the fucosylated variant of tumor-derived AFP (tAFP) has been observed in HCC patient serum.
Several functions of AFP have been described. With its structural similarity to albumin, it has been hypothesized to play a role in the transport of serum components, including fatty acids, steroids, and heavy metals [29]. Early studies revealed an inhibitory effect of cord blood-derived nAFP on lymphocyte function, whereas more recent reports suggest that AFP exerts its immunosuppressive activity through the induction of DC dysfunction [33–36]. However, there is little consensus about which cell subsets and/or signaling pathways are the primary targets of AFP-mediated immunosuppression.
AFP-specific immune responses
To investigate AFP as a target for immunotherapy, we initially identified several MHC class I-restricted epitopes and found that the epitope hierarchy of the CD8+ T cell response is altered in AFP+ HCC patients [37]. Our group observed that CD8+ T cells from HLA-A*0201+ healthy donors can recognize four dominant and 10 subdominant peptides in vitro [38]. Two clinical trials were performed to test the four immunodominant AFP peptides in (1) Montanide adjuvant and (2) on autologous DC [16, 39, 40]. Although no objective clinical responses were observed in the small numbers of vaccinated patients, AFP-specific T cell responses were either activated or enhanced in the majority of patients, providing proof of principle for the immunogenicity of AFP-targeted immunotherapeutic approaches. To learn more about AFP processing and presentation and to identify AFP uptake and intracellular processing pathways in DC, we recently showed that DC take up in both nAFP and tAFP very efficiently and that the protein accumulates in the perinuclear space. Loading DC with different forms of genetic and protein AFP forms results in alterations in subsequent CD8+ and CD4+ T cell responses [41].
Lessons learned from targeting AFP
In HCC patients exhibiting high levels of serum tAFP, we have observed a lower ratio of myeloid-to-plasmacytoid circulating DC compared to patients with low serum AFP levels and healthy donors [42]. To test the possible effect of nAFP or tAFP on DC differentiation, peripheral blood monocytes were cultured in vitro in the presence of nAFP or HCC-derived tAFP, and DC phenotype and function was assessed [42]. Although the nAFP and tAFP isoforms only differ at one glycosylation site, low levels of tAFP significantly inhibited DC differentiation while nAFP had a more modest impact. tAFP-exposed DC expressed lower levels of DC maturation markers, retained a monocyte-like morphology, exhibited limited production of inflammatory mediators, and failed to induce robust T cell proliferative responses. Mechanistic studies revealed that the suppressive activity of tAFP is dependent on the presence of low molecular weight (LMW) species that co-purify with tAFP. The suppressive activity was not associated with a co-purifying (or contaminating) protein, as shown by protein mass spectroscopy. Enzymatic elimination of fucose groups as well as of all sugar groups attached to tAFP did not eliminate the suppressive activity [42]. These data reveal the unique ability of tAFP to serve as a chaperone protein for a nonprotein/non-glycan LMW molecule which functions cooperatively with AFP protein to impair DC differentiation and function. Because AFP is known to bind to bilirubin, neopterin, and prostaglandin E2 (PGE2), we tested and eliminated those molecules as well. AFP is also well known to bind to a variety of lipid molecules which we have begun to investigate.
To further elucidate the molecular mechanisms of nAFP and tAFP-mediated immune suppression by monocytic DC that are exposed to these two forms of protein, we performed a full transcriptome analysis of monocytes from healthy donors exposed to nAFP, tAFP or a control protein from the albuminoid family. These studies are identifying several areas where AFP affects myeloid DC function.
AFP and NK cells
NK cells are effector cells of innate immunity that rapidly recognize and eliminate microbial pathogens and transformed cells, secrete immunomodulating cytokines, and regulate adaptive immune functions [43]. They represent 5–20 % of PBMC, but 25–50 % of resident liver leukocytes [44]. Compared with circulatory NK cells, hepatic NK cells have enhanced cytotoxic properties [44]. Due to their abundance and killing properties, hepatic NK cells play a critical role in the host’s defense against pathogens, tumor transformation, and in liver regeneration [44, 45].
NK function is reduced in HCC patients compared to healthy donors [46]. HCC patient NK cells have been shown to have impaired ability to kill tumor targets and secrete cytokines [47]. Additionally, overall frequencies of peripheral blood and liver NK cells are reduced [48], and low infiltration of NK cells into tumors is associated with poor prognosis in HCC patients. NK cells have been found to have impaired INF-γ production which has been associated with increased regulatory T cells (Treg) and myeloid-derived suppressor cells (MDSC) [49].
AFP was previously shown to indirectly impair NK cell activation by inhibiting IL-12 production by DC and was shown to inhibit NK cell activity by enhancing both the number and activity of suppressor cells. In contrast, the mechanism of how AFP might directly impact NK cell function has not been addressed. Limited literature suggests that AFP desensitizes NK cells to IFN-α, poly I:C or IL-2-mediated activation [33, 50]. Defining the impact of circulating tAFP on NK cells may be of central importance to understand the NK cell functional deficits described in HCC patients, and for the development of more effective HCC-targeting immunotherapies.
Recently, we compared the ability of nAFP to that of tAFP to modulate human NK cell activity and longevity in vitro. Short-term exposure to tAFP and especially nAFP proteins induces a pro-inflammatory, activated phenotype in healthy donor NK cells as indicated by CD69 and CD25 upregulation, IL-1β, IL-6, and TNF secretion, and enhanced tumor cell killing. In contrast, extended co-culture with tAFP, but not nAFP, inhibits NK cell proliferation and viability. NK cell activation is directly mediated by the AFP protein itself, while NK cell viability is affected by the low molecular mass cargo that co-purified with tAFP. Overall, these data show that nAFP and tAFP induce critical changes in NK cell function and viability, respectively.
Conclusions
In our series of clinical trials testing vaccines targeting non-mutated, overexpressed tumor antigens, we have found that activating and expanding CD8+ and CD4+ T cells specific to these antigens can be accomplished. There have been limited correlations between self-antigen T cell frequencies and clinical outcomes observed; hence, the immunologic mechanisms of tumor eradication are incompletely understood. In vivo cross-presentation of tumor-specific antigens may be critical to broaden the immune response, but how to promote this in vivo is not yet known. The many mechanisms of immune suppression and dysregulation by tumors are also incompletely understood. Uncovering the multiple ways in which tumor-secreted factors, including the oncofetal antigen AFP, can impair immunity will help direct future efforts at combating HCC and other tumors.
Abbreviations
- AdV:
-
Adenovirus
- AFP:
-
Alpha-fetoprotein
- CEA:
-
Carcinoembryonic antigen
- DC:
-
Dendritic cells
- EGFR:
-
Epidermal growth factor receptor
- HCC:
-
Hepatocellular cancer
- HPV:
-
Human papilloma virus
- LMW:
-
Low molecular weight
- MAGE-A1:
-
Melanoma antigen family A1
- MART-1:
-
Melanoma antigen recognized by T cells (aka Melan-A)
- nAFP:
-
Cord blood-derived normal alpha-fetoprotein
- NK:
-
Natural killer
- OFA:
-
Oncofetal antigen
- PGE2 :
-
Prostaglandin E2
- TAA:
-
Tumor-associated antigen
- tAFP:
-
Tumor-derived alpha-fetoprotein
- TIL:
-
Tumor-infiltrating lymphocytes
- Treg:
-
Regulatory T cells
- TSA:
-
Tumor-specific antigen
- WT-1:
-
Wilm’s tumor-1
References
Butterfield LH (2015) Cancer vaccines. BMJ 350:h988. doi:10.1136/bmj.h988
Le DT, Wang-Gillam A, Picozzi V, Greten TF, Crocenzi T, Springett G et al (2015) Safety and survival with GVAX pancreas prime and Listeria Monocytogenes-expressing mesothelin (CRS-207) boost vaccines for metastatic pancreatic cancer. J Clin Oncol 33(12):1325–1333. doi:10.1200/JCO.2014.57.4244
Finn OJ, Binder RJ, Brickner AG, Butterfield LH, Ferris RL, Kalinski P et al (2009) Human tumor antigens as targets of immunosurveillance and candidates for cancer vaccines. In: Gires O, Seliger B (eds) Tumor-associated antigens: identification, characterization and clinical applications. Wiley-VCH Verlag, GmbH & Co., Weinheim, pp 23–43
Cheever MA, Allison JP, Ferris AS, Finn OJ, Hastings BM, Hecht TT et al (2009) The prioritization of cancer antigens: a national cancer institute pilot project for the acceleration of translational research. Clin Cancer Res 15(17):5323–5337. doi:10.1158/1078-0432.CCR-09-0737
Butterfield LH, Ribas A, Dissette VB, Amarnani SN, Vu HT, Oseguera D et al (2003) Determinant spreading associated with clinical response in dendritic cell-based immunotherapy for malignant melanoma. Clin Cancer Res 9(3):998–1008
Ribas A, Glaspy JA, Lee Y, Dissette VB, Seja E, Vu HT et al (2004) Role of dendritic cell phenotype, determinant spreading, and negative costimulatory blockade in dendritic cell-based melanoma immunotherapy. J Immunother 27(5):354–367
Butterfield LH, Comin-Anduix B, Vujanovic L, Lee Y, Dissette VB, Yang JQ et al (2008) Adenovirus MART-1-engineered autologous dendritic cell vaccine for metastatic melanoma. J Immunother 31(3):294–309. doi:10.1097/CJI.0b013e31816a8910
Sercarz EE, Lehmann PV, Ametani A, Benichou G, Miller A, Moudgil K (1993) Dominance and crypticity of T cell antigenic determinants. Annu Rev Immunol 11:729–766. doi:10.1146/annurev.iy.11.040193.003501
Disis ML (2011) Immunologic biomarkers as correlates of clinical response to cancer immunotherapy. Cancer Immunol Immunother 60(3):433–442. doi:10.1007/s00262-010-0960-8
Ranieri E, Kierstead LS, Zarour H, Kirkwood JM, Lotze MT, Whiteside T et al (2000) Dendritic cell/peptide cancer vaccines: clinical responsiveness and epitope spreading. Immunol Invest 29(2):121–125
Arthur JF, Butterfield LH, Roth MD, Bui LA, Kiertscher SM, Lau R et al (1997) A comparison of gene transfer methods in human dendritic cells. Cancer Gene Ther 4(1):17–25
Ribas A, Butterfield LH, McBride WH, Jilani SM, Bui LA, Vollmer CM et al (1997) Genetic immunization for the melanoma antigen MART-1/Melan-A using recombinant adenovirus-transduced murine dendritic cells. Cancer Res 57(14):2865–2869
Butterfield LH, Jilani SM, Chakraborty NG, Bui LA, Ribas A, Dissette VB et al (1998) Generation of melanoma-specific cytotoxic T lymphocytes by dendritic cells transduced with a MART-1 adenovirus. J Immunol 161(10):5607–5613
Ribas A, Butterfield LH, McBride WH, Dissette VB, Koh A, Vollmer CM et al (1999) Characterization of antitumor immunization to a defined melanoma antigen using genetically engineered murine dendritic cells. Cancer Gene Ther 6(6):523–536. doi:10.1038/sj.cgt.7700076
Schumacher L, Ribas A, Dissette VB, McBride WH, Mukherji B, Economou JS et al (2004) Human dendritic cell maturation by adenovirus transduction enhances tumor antigen-specific T-cell responses. J Immunother 27(3):191–200
Liu Y, Daley S, Evdokimova VN, Zdobinski DD, Potter DM, Butterfield LH (2006) Hierarchy of alpha fetoprotein (AFP)-specific T cell responses in subjects with AFP-positive hepatocellular cancer. J Immunol 177(1):712–721
Blalock LT, Landsberg J, Messmer M, Shi J, Pardee AD, Haskell R et al (2012) Human dendritic cells adenovirally-engineered to express three defined tumor antigens promote broad adaptive and innate immunity. Oncoimmunology 1(3):287–357. doi:10.4161/onci.18628
Evdokimova VN, Liu Y, Potter DM, Butterfield LH (2007) AFP-specific CD4+ helper T-cell responses in healthy donors and HCC patients. J Immunother 30(4):425–437. doi:10.1097/CJI.0b013e31802fd8e2
Vujanovic L, Szymkowski DE, Alber S, Watkins SC, Vujanovic NL, Butterfield LH (2010) Virally infected and matured human dendritic cells activate natural killer cells via cooperative activity of plasma membrane-bound TNF and IL-15. Blood 116(4):575–583. doi:10.1182/blood-2009-08-240325
Vujanovic L, Ballard W, Thorne SH, Vujanovic NL, Butterfield LH (2012) Adenovirus-engineered human dendritic cells induce natural killer cell chemotaxis via CXCL8/IL-8 and CXCL10/IP-10. Oncoimmunology 1(4):448–457
Naveh HP, Vujanovic L, Butterfield LH (2013) Cellular immunity induced by a recombinant adenovirus human dendritic cell vaccine for melanoma. J Immunother Cancer 1:19. doi:10.1186/2051-1426-1-19
Mailliard RB, Wankowicz-Kalinska A, Cai Q, Wesa A, Hilkens CM, Kapsenberg ML et al (2004) alpha-type-1 polarized dendritic cells: a novel immunization tool with optimized CTL-inducing activity. Cancer Res 64(17):5934–5937. doi:10.1158/0008-5472.CAN-04-1261
Curtsinger JM, Valenzuela JO, Agarwal P, Lins D, Mescher MF (2005) Type I IFNs provide a third signal to CD8 T cells to stimulate clonal expansion and differentiation. J Immunol 174(8):4465–4469
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V et al (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
Forner A, Llovet JM, Bruix J (2012) Hepatocellular carcinoma. Lancet 379(9822):1245–1255. doi:10.1016/S0140-6736(11)61347-0
Pardee AD, Butterfield LH (2012) Immunotherapy of hepatocellular carcinoma: unique challenges and clinical opportunities. Oncoimmunology 1(1):48–55. doi:10.4161/onci.1.1.18344
Ormandy LA, Hillemann T, Wedemeyer H, Manns MP, Greten TF, Korangy F (2005) Increased populations of regulatory T cells in peripheral blood of patients with hepatocellular carcinoma. Cancer Res 65(6):2457–2464. doi:10.1158/0008-5472.CAN-04-3232
Lee JS, Chu IS, Heo J, Calvisi DF, Sun Z, Roskams T et al (2004) Classification and prediction of survival in hepatocellular carcinoma by gene expression profiling. Hepatology 40(3):667–676. doi:10.1002/hep.20375
Mizejewski GJ (2002) Biological role of alpha-fetoprotein in cancer: prospects for anticancer therapy. Expert Rev Anticancer Ther 2(6):709–735. doi:10.1586/14737140.2.6.709
Yang ZF, Ho DW, Ng MN, Lau CK, Yu WC, Ngai P et al (2008) Significance of CD90+ cancer stem cells in human liver cancer. Cancer Cell 13(2):153–166. doi:10.1016/j.ccr.2008.01.013
Tomasi TB Jr (1977) Structure and function of alpha-fetoprotein. Annu Rev Med 28:453–465. doi:10.1146/annurev.me.28.020177.002321
Mizejewski GJ (2001) Alpha-fetoprotein structure and function: relevance to isoforms, epitopes, and conformational variants. Exp Biol Med (Maywood) 226(5):377–408
Cohen BL, Orn A, Gronvik KO, Gidlund M, Wigzell H, Murgita RA (1986) Suppression by alpha-fetoprotein of murine natural killer cell activity stimulated in vitro and in vivo by interferon and interleukin 2. Scand J Immunol 23(2):211–223
Yachnin S (1976) Demonstration of the inhibitory effect of human alpha-fetoprotein on in vitro transformation of human lymphocytes. Proc Natl Acad Sci USA 73(8):2857–2861
Um SH, Mulhall C, Alisa A, Ives AR, Karani J, Williams R et al (2004) Alpha-fetoprotein impairs APC function and induces their apoptosis. J Immunol 173(3):1772–1778
Ritter M, Ali MY, Grimm CF, Weth R, Mohr L, Bocher WO et al (2004) Immunoregulation of dendritic and T cells by alpha-fetoprotein in patients with hepatocellular carcinoma. J Hepatol 41(6):999–1007. doi:10.1016/j.jhep.2004.08.013
Butterfield LH, Koh A, Meng W, Vollmer CM, Ribas A, Dissette V et al (1999) Generation of human T-cell responses to an HLA-A2.1-restricted peptide epitope derived from alpha-fetoprotein. Cancer Res 59(13):3134–3142
Butterfield LH, Meng WS, Koh A, Vollmer CM, Ribas A, Dissette VB et al (2001) T cell responses to HLA-A*0201-restricted peptides derived from human alpha fetoprotein. J Immunol 166(8):5300–5308
Butterfield LH, Ribas A, Meng WS, Dissette VB, Amarnani S, Vu HT et al (2003) T-cell responses to HLA-A*0201 immunodominant peptides derived from alpha-fetoprotein in patients with hepatocellular cancer. Clin Cancer Res 9(16 Pt 1):5902–5908
Butterfield LH, Ribas A, Dissette VB, Lee Y, Yang JQ, De la Rocha P et al (2006) A phase I/II trial testing immunization of hepatocellular carcinoma patients with dendritic cells pulsed with four alpha-fetoprotein peptides. Clin Cancer Res 12(9):2817–2825. doi:10.1158/1078-0432.CCR-05-2856
Pardee AD, Yano H, Weinstein AM, Ponce AA, Ethridge AD, Normolle DP et al (2015) Route of antigen delivery impacts the immunostimulatory activity of dendritic cell-based vaccines for hepatocellular carcinoma. J Immunother Cancer 3:32. doi:10.1186/s40425-015-0077-x
Pardee AD, Shi J, Butterfield LH (2014) Tumor-derived alpha-fetoprotein impairs the differentiation and T cell stimulatory activity of human dendritic cells. J Immunol 193(11):5723–5732. doi:10.4049/jimmunol.1400725
Caligiuri MA (2008) Human natural killer cells. Blood 112(3):461–469. doi:10.1182/blood-2007-09-077438
Gao B, Radaeva S, Park O (2009) Liver natural killer and natural killer T cells: immunobiology and emerging roles in liver diseases. J Leukoc Biol 86(3):513–528. doi:10.1189/JLB.0309135
Vujanovic NL, Polimeno L, Azzarone A, Francavilla A, Chambers WH, Starzl TE et al (1995) Changes of liver-resident NK cells during liver regeneration in rats. J Immunol 154(12):6324–6338
Taketomi A, Shimada M, Shirabe K, Kajiyama K, Gion T, Sugimachi K (1998) Natural killer cell activity in patients with hepatocellular carcinoma: a new prognostic indicator after hepatectomy. Cancer 83(1):58–63
Jinushi M, Takehara T, Tatsumi T, Hiramatsu N, Sakamori R, Yamaguchi S et al (2005) Impairment of natural killer cell and dendritic cell functions by the soluble form of MHC class I-related chain A in advanced human hepatocellular carcinomas. J Hepatol 43(6):1013–1020. doi:10.1016/j.jhep.2005.05.026
Sha WH, Zeng XH, Min L (2014) The correlation between NK cell and liver function in patients with primary hepatocellular carcinoma. Gut Liver 8(3):298–305. doi:10.5009/gnl.2014.8.3.298
Hoechst B, Voigtlaender T, Ormandy L, Gamrekelashvili J, Zhao F, Wedemeyer H et al (2009) Myeloid derived suppressor cells inhibit natural killer cells in patients with hepatocellular carcinoma via the NKp30 receptor. Hepatology 50(3):799–807. doi:10.1002/hep.23054
Cardoso E, Valdez G, Comini E, Matera L (1991) Effect of human alpha-fetoprotein on native and in vitro-stimulated NK activity. J Clin Lab Immunol 34(4):183–188
Acknowledgments
This work was supported by University of Pittsburgh Skin SPORE/National Institutes of Health Grant P50 CA121973; National Institutes of Health R01 Grant CA104524; and National Institutes of Health R01 Grant CA138635. This project used the University of Pittsburgh Cancer Institute Immunologic Monitoring and Cellular Products Laboratory shared resource (Lisa H. Butterfield, Director) that is supported in part by National Institutes of Health Grant award P30CA047904. The author acknowledges the support of Melanoma Program colleagues Dr. John M. Kirkwood, Dr. Ahmad A. Tarhini, and Dr. Hussein Tawbi in the current melanoma clinical studies. The author also thanks the current and recent members of the Butterfield research laboratory (Lazar Vujanovic, Patricia Santos, and Angela D. Pardee).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Lisa H. Butterfield is co-inventor of patents covering aspects of alpha-fetoprotein as a target for T cell-mediated anti-hepatocellular cancer immunity.
Additional information
This paper is a Focussed Research Review based on a presentation given at the Fourth International Conference on Cancer Immunotherapy and Immunomonitoring (CITIM 2015), held in Ljubljana, Slovenia, 27th–30th April 2015. It is part of a series of Focussed Research Reviews and meeting report in Cancer Immunology, Immunotherapy.
Rights and permissions
About this article

Cite this article
Butterfield, L.H. Lessons learned from cancer vaccine trials and target antigen choice. Cancer Immunol Immunother 65, 805–812 (2016). https://doi.org/10.1007/s00262-016-1801-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00262-016-1801-1