
Abstract
Purpose
The interaction of Fc fragments of antibodies with the Fcγ receptors is an essential checkpoint in antibody-dependent cellular cytotoxicity (ADCC). Specific polymorphisms at position 158 enhance FcγRIIIa affinity for IgG1 and are associated with improved clinical outcome in lymphoma patients treated with IgG1 anti-CD20 antibody. The role of ADCC in the therapeutic effects of the α-epidermal growth factor receptor (EGFR) mAb, cetuximab, in patients with squamous cell carcinoma of the head and neck (SCCHN) is poorly defined. We employed three SCCHN cell lines to test two hypotheses: (1) SCCHN is susceptible to cetuximab-mediated ADCC, (2) efficacy of ADCC is associated with polymorphisms at position 158 of FcγRIIIa.
Experimental design
FcγRIIIa-158 polymorphisms were determined for healthy donors, and their purified NK cells were used as effector cells against three SCCHN cell lines in ADCC assays. Cytotoxicity levels were compared for each polymorphism class. Proliferation and cell cycle assays were done to examine the direct effects of cetuximab.
Results
Our results indicate that SCCHN is susceptible to cetuximab-mediated ADCC in vitro. NK cytotoxic efficiency correlates with donor 158-polymorphisms in FcγRIIIa. Overall cytotoxicity was greatest for individuals having a single V allele when compared to homozygous F/F individuals; the cumulative percent cytotoxicity for each polymorphism among the cell lines was 58.2% V/V, 50.6% V/F, and 26.1% F/F (P < 0.001). Additionally, the presence of a V allele correlated with superior natural cytotoxicity against NK sensitive targets.
Conclusion
These data have both prognostic and therapeutic relevance and support the design of a prospective trial to determine the influence of FcγRIIIa polymorphisms on the clinical outcome of patients with SCCHN treated with α-EGFR mAbs.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Squamous cell carcinoma of the head and neck (SCCHN) affects nearly 40,000 new patients in the United States annually and half a million worldwide, accounting for nearly 5% of all new solid tumors [18]. Current SCCHN organ preservation options combine chemotherapy and radiation while newer approaches incorporate targeted therapeutics. Currently, the only approved targeted therapy for SCCHN is the epidermal growth factor receptor (EGFR) inhibitor, cetuximab (Erbitux®). Between 80 and 100% of SCCHNs over-express the EGF receptor, and the levels of over-expression are critical to overall tumor survival and are associated with increased treatment failures [1, 15]. Despite evidence that cetuximab in combination with radiotherapy improves outcome, its impact on both response rate and survival is incremental, with significant individual variability [4, 6, 7, 11]. One means to improve the therapeutic benefit of cetuximab is to define the population most likely to respond, through improved characterization of mode of action.
It is postulated that cetuximab’s primary mechanism of action results from EGFR blockade. Cetuximab is an IgG1 α-EGFR chimeric mAb that blocks the binding of natural receptor–ligand interactions, preventing ligand-dependent homodimerization, intracellular autophosphorylation, and activation of intracellular cascades that control cellular proliferation, adhesion, angiogenesis, and apoptosis [9, 10, 14]. Binding of cetuximab to the EGFR leads to internalization and degradation of the antibody–receptor complex and down-regulation of EGFR expression [6]. Because of the high propensity for over-expression of EGFR on SCCHN, cetuximab’s ability to block EFGR is especially advantageous in head and neck cancer.
Another potential mechanism of action of cetuximab, which has remained largely unexplored to date, is antibody-dependent cellular cytotoxicity (ADCC). ADCC is increasingly recognized as an important component of the clinical efficacy seen in targeted antibody therapy for solid tumors [6, 10, 20]. Growing experience with mAb targeted therapy in lymphoma patients demonstrates that select subpopulations experience superior clinical outcomes based upon FcγRIIIa polymorphisms known to influence ADCC. The most relevant polymorphisms regulating Fc:FcR interactions are phenylalanine (F) or valine (V) expression at position 158 of the Fc fragment [12, 19]. Indeed, Weng et al. demonstrated that the clinical response to rituximab in patients with non-Hodgkin’s lymphoma is predicted by the specific FcγRIIIa (CD16) polymorphism that they possess [33]. Similarly, in another study involving lymphoma patients treated with rituximab, individuals possessing the FcγRIIIa 158 V/V genotype experienced a better tumor response and survival [5]. It is postulated that the higher affinity binding of FcγRIIIa containing a V allele enhances ADCC and improves clinical response.
In this study we show for the first time that cetuximab can mediate ADCC in SCCHN, and more importantly, that these effects are more pronounced in individuals with a V at position 158 on FcγRIIIa. Unexpectedly, we also found that the presence of a V allele in donor NK cells is associated with enhanced tumoricidal activity against the NK sensitive K562 cell line, suggesting a broader enhanced cytotoxic phenotype associated with the V allele. Our results support the design and implementation of a clinical trial correlating FcγRIIIa polymorphisms with outcomes in SCCHN patients treated with cetuximab.
Materials and methods
Cell culture
Squamous cell carcinoma of the head and neck cell lines TU167 and TU159 were obtained from the University of Texas MD Anderson Cancer Center (Houston, TX, USA). The cell line 012SCC was donated by Bert O’Malley from the University of Pennsylvania School of Medicine (Philadelphia, PA, USA). Cells were cultured in RPMI 1640 complete media containing 10% heat-inactivated fetal bovine serum (Atlanta Biologics, Lawrenceville, GA, USA), 1% l-glutamine (Gibco, Carlsbad, CA, USA), 1% penicillin–streptomycin (Gibco, Carlsbad, CA, USA), and 1% HEPES buffer (Mediatech Inc., Herndon, VA, USA).
Flow cytometry
Squamous cell carcinoma of the head and neck cell lines were stained with the FITC-conjugated rat α-human EGFR mAb, clone ICR10 (Chemicon, Temecula, CA, USA) and APC-labeled cetuximab. Cetuximab was obtained from the University of Maryland School of Medicine, Marlene and Stewart Greenebaum Cancer Center Pharmacy (Baltimore, MD, USA) and conjugated by Invitrogen (Thousand Oaks, CA, USA) with APC fluorochrome. All SCCHN cell lines were also stained for α-human CD16 expression (BD Biosciences, San Jose, CA, USA). To evaluate NK purity after negative selection, isolated cells were stained with directly conjugated mouse α-human mAbs against CD56, CD11c, CD16, CD14, and CD3 (BD Biosciences, San Jose, CA, USA). A minimum of 10,000 events were acquired using a BD™ LSR II flow cytometer and analyzed with BD FACS DIVA Software.
NK cell separation
Healthy human buffy coat in acid citrate dextrose anticoagulant was purchased from Biological Specialty Corporation (Colmar, PA, USA). PBMCs were isolated from the buffy coat using Ficoll–Hypaque centrifugation method. NK cells were then negatively selected using a MACS® human NK cell isolation kit (Miltenyi Biotec, Auburn, CA, USA).
Determination of FcγRIIIa polymorphisms
Genomic DNA from human PBMCs was obtained using the Qiagen DNA extraction kit (Qiagen, Valencia, CA, USA) and stored at −20°C. The FcγRIIIa valine, V, or phenylalanine, F, at position 158 was determined by polymerase chain reaction (PCR), as described by Nieto et al., with modifications [26]. Briefly, the PCR reaction was optimized using 250 ng of DNA, 0.5 mM dNTPs, 1 U GoTaq polymerase (Promega, Madison, WI, USA) and corresponding 1× buffer containing 1.5 mM MgSO4 to a final volume of 50 μl. For PCR amplification, samples were subjected to an initial denaturation step at 94°C for 5 min, followed by 35 cycles at 94°C for 40 s, 52°C for 1 min, 72°C for 1 min, and a final extension at 72°C for 5 min.
Amplified PCR samples were cleaned using phenol extraction and ethanol precipitation prior to restriction digestion. Two digestions per sample were performed to distinguish the FcγRIIIa polymorphisms. First, 10 μl of the PCR product was incubated at 37°C overnight with 10 U of RsaI with the appropriate 1× buffer (Promega, Madison, WI, USA) to a final volume of 20 μl. For the second digestion, 10 μl of the RsaI digested sample was subsequently incubated at 37°C overnight with 40 U of Eco130I with the appropriate 1× buffer (Fermentas, Hanover, MD, USA) to a final volume of 30 μl. Both RsaI and RsaI/Eco130I digested products were separated on a 3% agarose gel with ethidium bromide and visualized under UV light.
Antibody-dependent cellular mediated cytotoxicity
Antibody-dependent cellular cytotoxicity assays were performed using SCCHN cells as targets, and purified NK cells as effectors. Target cells were incubated with 150 μCi of chromium-51 (51Cr) (Amersham, Piscataway, NJ, USA) at 37°C for 1 h, mixing thoroughly every 15 min, and washed twice with media. Cells were subsequently incubated with 10 μg/ml of cetuximab, 10 μg/ml of human IgG1 isotype, or media alone for another 30 min at 37°C, and washed twice with media to remove unbound antibodies. Effector and target cells were plated at 50:1, 25:1, and 12.5:1 in 96 well plates and incubated overnight. Each assay was set up in triplicate. Cell lysis supernatant was collected and mixed with the Optiphase Supermix scintillation fluid (Perkin Elmer, Boston, MA, USA) and counted in a MicroBeta 1450 scintillation counter (Wallac, Turku, Finland). The NK sensitive K562 tumor cell line was used as a positive control for all ADCC experiments. Results were expressed as the percentage of specific lysis according to the following formula:
Thymidine proliferation assay
Growth inhibition of SCCHN in the presence of cetuximab was evaluated using thymidine assays. Each cell line was seeded at day 1 to a 96-well tissue culture plate at 0.1 × 104 cells/well in 100 μl RPMI complete media. For dose-dependent inhibition assays, cetuximab or IgG1 isotype controls were added to final concentrations of 10, 0.1, 0.01, 0.001, and 0.0001 μg/ml to the appropriate wells. For media only controls, 100 μl of media was added to the appropriate wells. Plates were incubated at 37°C in a 5% CO2 atmosphere for 48 h. Thymidine was added on day 3 to a concentration of 1 μCi/well, and plates were incubated for an additional 14–16 h. Cells were embedded onto collection filters using the Packard Cell Harvester (Packard Biosciences, Shelton, CT, USA). The filters were dried and counted in β-scintillation fluid using the MicroBeta 1450 scintillation counter (Wallac, Turku, Finland).
Cell cycle distribution
A BrdU Flow Kit (BD Pharmingen, San Jose, CA, USA) with 7-AAD was utilized to determine the effect of cetuximab on SCCHN cell cycle and DNA content. Tumor cells were seeded in 6-well plates at 1.5 × 105 cells/well. Cetuximab or isotype controls were introduced at 10 μg/ml and incubated for 48 h. Then the cells were pulsed with BrdU on day 3 for 4 h at 37°C, and stained according to manufacturer’s protocol.
Statistical methods
Statistical analyses were performed using the SAS statistical software (SAS version 9.1; SAS Institute, Cary, NC, USA) and S-plus. Mean cytotoxicity was computed for each polymorphism according to the equation listed previously. Welch modified two-sample t-test (if the normality was not plausible), Student’s t-test (a Q–Q plot was used to assess the correctness of normality assumption) and analysis of variance were used to determine statistically significant differences in mean cytotoxicity among cells bearing FcγRIIIa polymorphisms. Differences were considered to be significant at P-value below 0.05.
Results
FcγRIIIa polymorphism distribution
To establish the genotype of the FcγRIIIa for each donor, we modified an existing protocol to obtain a robust PCR amplification/restriction digest methodology that permitted the typing of each donor sample. We evaluated the frequency of polymorphisms at amino acid 158 from 45 samples, which included 17 fresh donor PBMCs that were used for ADCC studies and an additional 28 frozen donor PBMC samples. The frequency for F allele was calculated to be 0.70, and V allele to be 0.30.
The combined distribution of polymorphic classes from our fresh and frozen donors was 51.1% F/F, 37.8% V/F, and 11.1% V/V.
Cetuximab treatment of NK cells containing the FcγRIIIa V allele increases efficiency of ADCC against SCCHN
In order to develop a model system to study ADCC for SCCHN, we initially characterized the EGFR expression on our tumor targets. We confirmed the EGFR over-expression for the three different tumor cell lines (TU167, TU159, and 012SCC) utilized in this study using both a monoclonal rat-derived α-human EGFR antibody and cetuximab (Fig. 1). In order to rule out positive staining due to secondary Fc binding, each tumor cell line was stained for the expression of FcγRIIIa (CD16) using commercially available α-CD16 mAb. Our data indicate that none of the SCCHN cell lines expressed CD16 (data not shown).

Epidermal growth factor receptor expression in SCCHN tumor cell lines. SCCHN cell lines TU167, TU59, and 012SCC were stained with a α-EGFR mAb (clone ICR10) with an IgG2a isotype control and b Cetuximab with human IgG1 isotype control. Open histograms represent the isotype control. Filled histograms represent the mAbs staining. All cell lines show a comparable shift for both α-EGFR and cetuximab mAbs
We first employed TU167 to determine whether cetuximab mediates ADCC, and to define the impact of FcγRIIIa polymorphisms. In our initial study, we employed TU167 as target cells. We found that cetuximab-mediated ADCC is enhanced against this cell line in individuals possessing a V allele at all effector to target ratios (Fig. 2). Combinatorial analysis of all ADCC experiments against TU167 revealed that donors with either V/V (64.0%) or V/F (47.5%) had superior cytotoxic activity against TU167 when compared to NK cells from F/F (22.5%) individuals at a 50:1 effector to target (E:T) ratio, (P = 0.04 and 0.004, respectively). This effect is not cell line specific as the advantage of having at least one V allele when compared to F/F was also seen for 012SCC, where individuals with at least one V allele (V/V and V/F) had a combined mean percent cytotoxicity of 65.0% compared to 34.5% for those with F/F (P = 0.0019) at 50:1 ratio. While we observed a similar trend in polymorphism-associated killing against TU159, differences were not statistically significant. This lack of significance was most likely due to the small sample size. Using an analysis of variance, we determined that there was a significant difference among the cumulative mean percent cytotoxicity for each polymorphism against all three SCCHN cell lines at 50:1 effector to target ratio: 58.2% V/V, 50.6% V/F, and 26.1% F/F (P < 0.001). Cetuximab-treated SCCHN cell lines were subjected to higher levels of ADCC compared with cells treated with isotype controls or media alone. These data provide strong evidence for cetuximab-mediated ADCC in SCCHN, and demonstrate a direct correlation between cytotoxicity and the presence of a V allele at position 158 of FcγRIIIa (Table 1).

NK FcγRIIIa polymorphisms influencing cytotoxic activity on cetuximab-treated SCCHN TU167. a NK cells purified from PBMCs of healthy donors expressing either F/F, V/F, or V/V alleles were tested for cytotoxicity against TU167 in a standard 51Cr-release assay. Before addition of effector cells, TU167 target cells were pretreated with media alone (dark filled diamond), human IgG1 isotype control at 10 μg/ml (dark filled square), or cetuximab 10 μg/ml (dark filled triangle). Data are representative of independent experiments performed in triplicates, with error bars indicating SEM. b NK cells purified from PBMCs of 17 individual donors F/F (open diamond), V/F (open square), and V/V (open triangle) alleles were tested for cytotoxicity against the TU167 SCCHN cell line using a standard 51Cr-release assay. Before addition of effector cells TU167 targets were pretreated with media alone, human IgG1 isotype control at 10 μg/ml, or cetuximab at 10 μg/ml. Donors with either FcγRIIIa V/V or FcγRIIIa V/F demonstrated significantly higher percent cytotoxicity compared to FcγRIIIa F/F, when incubated with 10 μg/ml cetuximab (P = 0.04 and 0.004, respectively)
The presence of a V allele is associated with enhanced NK killing of NK sensitive targets
Our study and others have demonstrated that the presence of a V allele at position 158 enhances ADCC in both SCCHN and lymphoma [16, 32, 33]. However, it is uncertain whether the impact of such polymorphisms correlates with other important intrinsic differences in NK cytotoxic potential. In order to test the hypothesis that NK cells with a V allele are associated with an enhanced cytotoxic potential unrelated to ADCC, we evaluated the cytotoxic ability of NK cells stratified by FcγRIIIa polymorphisms, against K562 tumor target, which is MHC Class I deficient. Interestingly, we observed that the presence of a V allele in donor NK cells was associated with significantly enhanced cytotoxicity against the NK sensitive K562 target (Fig. 3). Using the Welch modified two-sample t-test, we determined that donors possessing FcγRIIIa V/F and V/V at 50:1, 25:1 and 12.5:1 have significantly higher cytotoxic activity than that of FcγRIIIa F/F donors (P = 0.17, 0.044, and 0.043 respectively, CI = 90%). These data for the first time suggest that NK cells containing a single V allele provide better direct tumor killing in an antibody-independent manner.

FcγIIIaR V polymorphism is associated with enhanced natural cytotoxicity against K562 tumor targets. Tumor cell line K562 was subjected to direct NK cytotoxicity in the absence of antibody. Shown here, NK cells from healthy donors bearing FcγIIIaR F/F (open diamond), V/F (open square), and V/V (open triangle) alleles were tested for cytotoxicity against K562 using a standard 51Cr-release assay
Cetuximab induces anti-proliferative effects
In addition to studying cetuximab-mediated ADCC in SCCHN, we set out to evaluate the direct, anti-proliferative effect of cetuximab on SCCHN, using thymidine proliferation assays. A significant dose-dependent inhibition on cell growth was observed on TU159 in concentrations ranging between 10 pg/ml and 10 μg/ml of cetuximab when compared to cells cultured with isotype controls (Fig. 4). Interestingly, there was no dose-dependent inhibition observed with TU167 and 012SCC and the effect on proliferation of these two cell lines when co-incubated with cetuximab was less sensitive compared to TU159. Thus, among the three EGFR over-expressed (>90%) cell lines, inhibition by cetuximab did not correlate with EGFR expression.

Dose-dependent anti-proliferative activity of cetuximab measured by [3H] thymidine assays. TU159 cell line was cultured in the presence of various concentrations of cetuximab for 72 h. Proliferation was measured by thymidine incorporation. Cetuximab significantly inhibited TU159 in a dose-dependent fashion
In order to understand how cetuximab influences tumor growth, we employed BrdU/7-AAD strategy to determine the effects of cetuximab on the cell cycle. TU159 showed an approximate twofold increase in G2 + M phase of the cell cycle, while no overt pro-apoptotic effect was induced by cetuximab (Fig. 5). Consistent with our proliferation studies, 012SCC and TU167 did not demonstrate significant reductions in DNA synthesis. Distinct from its likely role in ADCC, cetuximab may demonstrate a specific anti-proliferative effect on SCCHN. This experiment supports the ability of cetuximab in directly inhibiting SCCHN growth, in some instances, via blockade of the EGFR mechanism rather than direct cytotoxicity.

Cell cycling and DNA synthesis activity of TU159 with 10 μg/ml cetuximab. Panels a, b, and c indicate representative experiments for TU159 in media alone, 10 μg/ml isotype control or 10 μg/ml cetuximab respectively. With cetuximab incubation, an increase in phase G2 + M (P5 quadrant) was observed compared to isotype control. S-phase (P6 quadrant) was decreased by at least twofold in panel c compared to panels a and b
Discussion
Targeted therapy with monoclonal antibodies, such as cetuximab, is an integral part of the management of a wide range of malignancies [2, 8, 20, 25, 33, 35]. In the present study, we demonstrate for the first time evidence for cetuximab-mediated ADCC in vitro among three different SCCHN cell lines. The effectiveness of ADCC is associated with FcγRIIIa donor polymorphisms recognized to enhance Fc:FcR interactions. Importantly, we also show that the presence of a V allele correlates with the ability of NK cells to kill sensitive targets in the absence of antibody. These data provide insight into the mechanism of action of cetuximab for SCCHN, and contribute to an increasing body of literature clarifying the role of FcγRIIIa polymorphisms in ADCC.
While the clinical relevance of ADCC is difficult to establish, we provide in vitro data that supports its presence in SCCHN. Several recent studies also provide strong evidence supporting the impact of ADCC in targeted therapies for lymphoma, esophageal, melanoma, and colon cancer [20, 25, 32, 35]. For example, Weng and Levy have demonstrated a rituximab-mediated cytotoxicity (ranging from 13.5 to 100%) for lymphoma cells from 43 patients using effector cells from healthy donors [32]. Recently, Kurai has provided evidence for cetuximab-mediated ADCC using low-expressing EGFR lung cancer cell lines as targets and healthy donor PMBCs as effectors. In this study, Kurai demonstrated that NK cells were the effector cells responsible for ADCC and that their cytotoxicity was enhanced by IL-2 [20]. Similarly, Naramura et al. demonstrated evidence for ADCC in a melanoma tumor model. These reports are consistent with and support our finding demonstrating that cetuximab mediates ADCC in SCCHN.
Perhaps the most compelling support for the clinical contribution of ADCC relates to the observation that polymorphic variations of NK FcγRIIIa influence clinical response and survival [32, 33]. This observation, coupled with the fact that NK cells are the principle effector cells facilitating ADCC, lends support to the clinical relevance of ADCC as an important mechanism of action for cetuximab. The V allele not only confers more efficient ADCC in vitro, but is also associated with better clinical outcomes. In addition to providing evidence for ADCC, our data also convincingly show that donor NK cells that contain a FcγRIIIa V polymorphism at position 158 demonstrate more efficient cytotoxicity against SCCHN cell lines. This important finding was seen in all three SCCHN cell lines. However, given the infrequency of homozygous V donors and relatively small number of samples, we did not see a statistically significant higher cytotoxicity to determine superiority of V/V over V/F. Incidentally, the frequency of the V allele in our sample of donors was 0.3, which is in keeping with the frequency found by others [5, 32, 35]. These findings are significant because they may have profound implications for the identification of SCCHN patients most likely to respond to cetuximab.
Other investigators also provide support for an enhanced effect of the 158-V polymorphism. Hatjiharissi et al. demonstrated the superior effect of having a single V allele on ADCC against two CD20 expressing target cells lines using rituximab and NK cells from 52 healthy donors [16]. Not only was rituximab-mediated ADCC activity higher with the presence of at least one valine compared to those homozygous for phenylalanine, but there was also a higher absolute number of CD16 receptors per NK cell for donors who expressed at least one V allele. It also has been well established that FcγRIIIa V binds to human IgG1 better than the FcγRIIIa F, and this increased affinity of the FcγRIIIa V translates to an enhanced ADCC in the presence of NK cells [29, 31]. Optimizing the binding of FcγRIIIa to the Fc portion of targeted mAbs may offer an effective mechanism to overcome individual variability in Fc:FcR interactions. Mechanistically, these data suggest that it is not only the higher affinity binding of the Fc:FcR for the V allele that confers ADCC benefits, but the higher absolute number of CD16 receptors among individuals with the V allele may contribute to the superiority observed by many investigators.
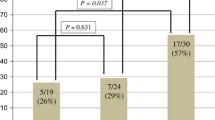
Additionally, there have been clinical studies reporting that individuals homozygous for the V allele have an advantage over those that are either heterozygous V/F or homozygous F. A retrospective clinical review of 136 lymphoma patients demonstrated a clinical 5-year progression free survival (PFS) for V/V, V/F, and F/F equaling 77, 38, and 48%, respectively [32]. Another analysis of 87 lymphoma patients by Weng et al. confirmed the clinical benefits of homozygous V with a 2-year PFS for V/V, V/F, and F/F that was 45, 12, and 16%, respectively [33]. In contrast to the in vitro studies, these clinical findings suggest that lymphoma patients with the homozygous V allele may experience better clinical outcomes when treated with rituximab.
While there is compelling support for the positive effect of a V allele on ADCC, there are studies that do not maintain this position. Zhang et al. recently suggested that V/V at amino acid position 158 was unfavorable among 35 patients with disseminated colon cancer [35]. However, only 5 (14%) of the patients in this study were V/V and the benefit attributed to having an F was not statistically significant in this small sample. No direct measure of ADCC was performed in this study to correlate with their observed clinical outcomes. Additionally, because many end-stage patients are relatively immunosuppressed and have significantly impaired NK function [20], the findings in this small, single institution study should be viewed in context. Other small studies were not able to provide evidence for or against the role of polymorphisms in outcomes using targeted antibody treatments, as well [13, 22]. While additional studies are necessary, our findings demonstrating the benefit of a V allele for cetuximab-mediated ADCC is supported by larger, reproducible clinical and in vitro ADCC studies described previously.
One of the principle goals of this study was to evaluate cetuximab-medicated ADCC in SCCHN, however we acknowledge that there are additional proposed mechanisms for cetuximab’s anti-tumor effect, such as complement dependent cytotoxicity, competitive inhibition, or possibly direct pro-apoptotic effects [21, 28]. Crystallography studies show that cetuximab interacts with the ligand binding domain of the receptor, resulting in steric hindrance of ligand binding and subsequent dimerization of the molecule, which prevents EGFR autophosphorylation and activation [17]. Therefore, we also evaluated the direct inhibition of the EGF receptor via proliferation and cell cycle experiments.
Our proliferation studies demonstrate significant inhibition only against TU159 in a dose-dependent fashion, resulting in cell cycle arrest at the S-phase, with an increased shift at the G0/G1 phase. We did not observe significant apoptosis any of the three cell lines. Thus, it appears that this anti-proliferative property of cetuximab relates to direct inhibition of ligand binding. However, we did not observe significant levels of cetuximab inhibition with TU167 and 012SCC compared to TU159, despite similar EGFR expression among the three cell lines. Our findings demonstrate that inhibition did not correlate with EGFR expression. In fact, some EGFR over-expressed cancers demonstrate an ability to become less sensitive to cetuximab and proliferate in a manner that is less dependent on the EGFR/tyrosine kinase pathway [17, 27, 28, 34]. Interestingly, even though there is variation in cetuximab inhibition among the three tumor targets, all three cell lines show a strong susceptibility to cetuximab-mediated ADCC.
In addition to ADCC, NK cells possess other important cytotoxic functions. Some of these include antibody-independent mechanisms of cytotoxicity, and their effectiveness in this capacity may also be associated with FcγRIIIa polymorphisms. Interestingly, we observed an unexpected, not previously described finding that donor NK cells with a V allele were associated with superior cytotoxicity against K562 in an antibody-independent mechanism. This is the first report documenting an association with the FcγRIIIa polymorphisms in antibody-independent cytotoxicity with NK. Thus, in addition to demonstrating more efficient ADCC against SCCHN cells, NK cells with a V allele also were associated with statistically significantly higher cytotoxicity against NK susceptible K562 in the absence of antibody.
The mechanism for the enhanced cytotoxic potential of NK cells bearing a V allele against NK sensitive targets is unknown. Sivori describes NK cells with phenotypically more proficient cytotoxic activity that have a higher surface density of NKp46, an important NK natural cytotoxicity receptor (NCR) [30]. Others have confirmed that individual donors have populations of NK with heterogeneous surface densities of NCRs as well as other NK co-receptors that correlate with NK cytotoxic activity [3, 23, 24, 30]. Additional studies are necessary to determine if the same polymorphisms that are associated with enhanced ADCC in SCCHN may also correlate with a phenotype that confers superior cytotoxicity.
The intent of our study was to determine if FcγRIIIa polymorphisms are important in predicting response to cetuximab in SCCHN tumor cells. We demonstrate, for the first time, that cetuximab can induce NK mediated ADCC in SCCHN in vitro. Furthermore, we show that CD16 polymorphisms play a critical role in the efficiency of ADCC in SCCHN. Specifically the addition of a V allele provides enhanced ADCC. This observation may prove to be an important marker for identifying individuals who can derive the greatest benefit from cetuximab based therapies. An additional finding is that the V allele may not only be associated with enhanced ADCC, but may also correlate with an enhanced antibody-independent cytotoxicity. Our observations provide insight into the mechanism by which cetuximab may mediate therapeutic effects in vivo and provide a rationale for developing clinical trials to determine the role of FcγRIII polymorphisms and response to cetuximab in patients with SCCHN.
References
Ang KK, Berkey BA, Tu X, Zhang HZ, Katz R, Hammond EH, Fu KK, Milas L (2002) Impact of epidermal growth factor receptor expression on survival and pattern of relapse in patients with advanced head and neck carcinoma. Cancer Res 62:7350–7356
Arnould L, Gelly M, Penault-Llorca F, Benoit L, Bonnetain F, Migeon C, Cabaret V, Fermeaux V, Bertheau P, Garnier J, Jeannin JF, Coudert B (2006) Trastuzumab-based treatment of HER2-positive breast cancer: an antibody-dependent cellular cytotoxicity mechanism? Br J Cancer 94:259–267
Biassoni R, Cantoni C, Pende D, Sivori S, Parolini S, Vitale M, Bottino C, Moretta A (2001) Human natural killer cell receptors and co-receptors. Immunol Rev 181:203–214
Bonner JA, Spencer SA (2006) Postoperative radiotherapy in non-small-cell lung cancer warrants further exploration in the era of adjuvant chemotherapy and conformal radiotherapy. J Clin Oncol 24:2978–2980
Bowles JA, Weiner GJ (2005) CD16 polymorphisms and NK activation induced by monoclonal antibody-coated target cells. J Immunol Methods 304:88–99
Burtness B (2005) The role of cetuximab in the treatment of squamous cell cancer of the head and neck. Expert Opin Biol Ther 5:1085–1093
Burtness B, Goldwasser MA, Flood W, Mattar B, Forastiere AA (2005) Phase III randomized trial of cisplatin plus placebo compared with cisplatin plus cetuximab in metastatic/recurrent head and neck cancer: an Eastern Cooperative Oncology Group study. J Clin Oncol 23:8646–8654
Cartron G, Dacheux L, Salles G, Solal-Celigny P, Bardos P, Colombat P, Watier H (2002) Therapeutic activity of humanized anti-CD20 monoclonal antibody and polymorphism in IgG Fc receptor FcgammaRIIIa gene. Blood 99:754–758
Choong NW, Cohen EE (2006) Epidermal growth factor receptor directed therapy in head and neck cancer. Crit Rev Oncol Hematol 57:25–43
Cohen EE, Lingen MW, Vokes EE (2004) The expanding role of systemic therapy in head and neck cancer. J Clin Oncol 22:1743–1752
Cunningham D, Humblet Y, Siena S, Khayat D, Bleiberg H, Santoro A, Bets D, Mueser M, Harstrick A, Verslype C, Chau I, Van Cutsem E (2004) Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 351:337–345
de Haas M, Koene HR, Kleijer M, de Vries E, Simsek S, van Tol MJ, Roos D, von dem Borne AE (1996) A triallelic Fc gamma receptor type IIIA polymorphism influences the binding of human IgG by NK cell Fc gamma RIIIa. J Immunol 156:3948–3955
Farag SS, Flinn IW, Modali R, Lehman TA, Young D, Byrd JC (2004) Fc gamma RIIIa and Fc gamma RIIa polymorphisms do not predict response to rituximab in B-cell chronic lymphocytic leukemia. Blood 103:1472–1474
Grandis JR, Sok JC (2004) Signaling through the epidermal growth factor receptor during the development of malignancy. Pharmacol Ther 102:37–46
Grandis JR, Zeng Q, Tweardy DJ (1996) Retinoic acid normalizes the increased gene transcription rate of TGF-alpha and EGFR in head and neck cancer cell lines. Nat Med 2:237–240
Hatjiharissi E, Xu L, Santos DD, Hunter ZR, Ciccarelli BT, Verselis S, Modica M, Cao Y, Manning RJ, Leleu X, Dimmock EA, Kortsaris A, Mitsiades C, Anderson KC, Fox EA, Treon SP (2007) Increased natural killer cell expression of CD16, augmented binding and ADCC activity to rituximab among individuals expressing the Fc{gamma}RIIIa-158 V/V and V/F polymorphism. Blood 110:2561–2564
Huether A, Hopfner M, Baradari V, Schuppan D, Scherubl H (2005) EGFR blockade by cetuximab alone or as combination therapy for growth control of hepatocellular cancer. Biochem Pharmacol 70:1568–1578
Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ (2005) Cancer statistics, 2005. CA Cancer J Clin 55:10–30
Koene HR, Kleijer M, Algra J, Roos D, von dem Borne AE, de Haas M (1997) Fc gammaRIIIa-158V/F polymorphism influences the binding of IgG by natural killer cell Fc gammaRIIIa, independently of the Fc gammaRIIIa-48L/R/H phenotype. Blood 90:1109–1114
Kurai J, Chikumi H, Hashimoto K, Yamaguchi K, Yamasaki A, Sako T, Touge H, Makino H, Takata M, Miyata M, Nakamoto M, Burioka N, Shimizu E (2007) Antibody-dependent cellular cytotoxicity mediated by cetuximab against lung cancer cell lines. Clin Cancer Res 13:1552–1561
Li S, Schmitz KR, Jeffrey PD, Wiltzius JJ, Kussie P, Ferguson KM (2005) Structural basis for inhibition of the epidermal growth factor receptor by cetuximab. Cancer Cell 7:301–311
Lin TS, Flinn IW, Modali R, Lehman TA, Webb J, Waymer S, Moran ME, Lucas MS, Farag SS, Byrd JC (2005) FCGR3A and FCGR2A polymorphisms may not correlate with response to alemtuzumab in chronic lymphocytic leukemia. Blood 105:289–291
Moretta L, Moretta A (2004) Unravelling natural killer cell function: triggering and inhibitory human NK receptors. EMBO J 23:255–259
Moretta A, Bottino C, Vitale M, Pende D, Cantoni C, Mingari MC, Biassoni R, Moretta L (2001) Activating receptors and coreceptors involved in human natural killer cell-mediated cytolysis. Annu Rev Immunol 19:197–223
Naramura M, Gillies SD, Mendelsohn J, Reisfeld RA, Mueller BM (1993) Therapeutic potential of chimeric and murine anti-(epidermal growth factor receptor) antibodies in a metastasis model for human melanoma. Cancer Immunol Immunother 37:343–349
Nieto A, Caliz R, Pascual M, Mataran L, Garcia S, Martin J (2000) Involvement of Fcgamma receptor IIIA genotypes in susceptibility to rheumatoid arthritis. Arthritis Rheum 43:735–739
Peruzzi B, Bottaro DP (2006) Targeting the c-Met signaling pathway in cancer. Clin Cancer Res 12:3657–3660
Raben D, Helfrich B, Chan DC, Ciardiello F, Zhao L, Franklin W, Baron AE, Zeng C, Johnson TK, Bunn PA Jr (2005) The effects of cetuximab alone and in combination with radiation and/or chemotherapy in lung cancer. Clin Cancer Res 11:795–805
Shields RL, Namenuk AK, Hong K, Meng YG, Rae J, Briggs J, Xie D, Lai J, Stadlen A, Li B, Fox JA, Presta LG (2001) High resolution mapping of the binding site on human IgG1 for Fc gamma RI, Fc gamma RII, Fc gamma RIII, and FcRn and design of IgG1 variants with improved binding to the Fc gamma R. J Biol Chem 276:6591–6604
Sivori S, Pende D, Bottino C, Marcenaro E, Pessino A, Biassoni R, Moretta L, Moretta A (1999) NKp46 is the major triggering receptor involved in the natural cytotoxicity of fresh or cultured human NK cells. Correlation between surface density of NKp46 and natural cytotoxicity against autologous, allogeneic or xenogeneic target cells. Eur J Immunol 29:1656–1666
Vance BA, Huizinga TW, Wardwell K, Guyre PM (1993) Binding of monomeric human IgG defines an expression polymorphism of Fc gamma RIII on large granular lymphocyte/natural killer cells. J Immunol 151:6429–6439
Weng WK, Levy R (2003) Two immunoglobulin G fragment C receptor polymorphisms independently predict response to rituximab in patients with follicular lymphoma. J Clin Oncol 21:3940–3947
Weng WK, Czerwinski D, Timmerman J, Hsu FJ, Levy R (2004) Clinical outcome of lymphoma patients after idiotype vaccination is correlated with humoral immune response and immunoglobulin G Fc receptor genotype. J Clin Oncol 22:4717–4724
Wheeler DL, Huang S, Kruser TJ, Nechrebecki MM, Armstrong EA, Benavente S, Gondi V, Hsu KT, Harari PM (2008) Mechanisms of acquired resistance to cetuximab: role of HER (ErbB) family members. Oncogene 27(28):3944–3956
Zhang W, Gordon M, Schultheis AM, Yang DY, Nagashima F, Azuma M, Chang HM, Borucka E, Lurje G, Sherrod AE, Iqbal S, Groshen S, Lenz HJ (2007) FCGR2A and FCGR3A polymorphisms associated with clinical outcome of epidermal growth factor receptor expressing metastatic colorectal cancer patients treated with single-agent cetuximab. J Clin Oncol 25:3712–3718
Acknowledgments
Scott E. Strome receives royalties through the Mayo Clinic College of Medicine through licensure of intellectual property related to specific co stimulatory molecules to various third parties. This work was supported in part by American Cancer Society Institutional Research Pilot grant IRG-97-153-04.
Author information
Authors and Affiliations
Corresponding author
Additional information
Contribution: S. Chan performed experiments and analyzed data; S.E. Strome, S. Chan, C.J. Voskens, L. Wei, D. Schulze, and R.J. Taylor designed and analyzed data; R.J. Taylor, S. Chan, D.H. Schulze, and S.E. Strome authored the manuscript. G. Tian and R.J. Taylor provided statistical consultation. Other important contributions were made by A. Wood, J. Wolf, and A. Chapoval. Cetuximab was obtained from University of Maryland School of Medicine, Marlene and Stewart Greenebaum Cancer Center Pharmacy (Baltimore, MD, USA). S.E. Strome is a co-founder and major stock holder of Gliknik Inc., a Biotechnology Company.
An erratum to this article can be found at http://dx.doi.org/10.1007/s00262-009-0720-9
Rights and permissions
About this article
Cite this article
Taylor, R.J., Chan, SL., Wood, A. et al. FcγRIIIa polymorphisms and cetuximab induced cytotoxicity in squamous cell carcinoma of the head and neck. Cancer Immunol Immunother 58, 997–1006 (2009). https://doi.org/10.1007/s00262-008-0613-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00262-008-0613-3