
Abstract
There are many mechanisms that regulate and dampen the immune response to cancers, including several types of regulatory T cells. Besides the T reg cell, we have identified another immunoregulatory circuit initiated by NKT cells that produce IL-13 in response to tumor growth and this IL-13 then induces myeloid cells to make TGF-β that inhibits cytotoxic T cell-mediated tumor immunosurveillance in several mouse tumor models. This finding created a paradox in the role of NKT cells in tumor immunity, in that they can also contribute to protection. We resolve this paradox by the finding that the suppressive NKT cell is a type II NKT cell that lacks the canonical invariant T cell receptor, whereas the protective cell is a type I NKT cell that expresses the invariant receptor. Further, we see that these two subsets of NKT cells counter-regulate each other, defining a new immunoregulatory axis. The balance along this axis may determine the outcome of tumor immunosurveillance as well as influence the efficacy of anti-cancer vaccines and immunotherapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
We know that cancer vaccines can often induce substantial levels of tumor-specific cytotoxic T lymphocytes (CTL) measured in vitro, but much less often induce clinical tumor regression. Why? The reason probably has to do with a number of types of immunoregulatory mechanisms that constrain or suppress the T cell immune response or its effector function. These include downregulation of class I MHC molecules or processing machinery, expression of suppressive cytokines, activation of off-signaling receptors on T cells like CTLA-4 or PD-1, and suppression by immune cells. The latter include myeloid-derived suppressor cells (MDSC), granulocyte suppressors, M2 macrophages, T regulatory cells, and NKT cells. This study focused on the role of NKT cells.
NKT cells are true T cells, not NK cells, in that they have a true T cell receptor (TCR) and CD3, but they also have some innate immune functions, and some express NK1.1. However, the biggest difference from conventional T cells is that instead of recognizing a peptide presented by a classical class I or II molecule, they recognize a lipid antigen presented by the non-classical class I-like MHC molecule, CD1d [3, 12]. Thus, the NKT cells are completely absent in CD1d knockout (KO) mice. Further, the majority are CD4+, although some are also CD4/CD8 double negative, but the role of CD4 in their function is not well understood, given that they don’t recognize class II MHC molecules.
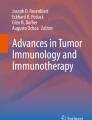
We studied a tumor model of an immunogenic BALB/c fibrosarcoma, 15-12RM, that expresses the HIV envelope protein as well as mutant ras and myc. Because it expresses a foreign viral antigen, it is immunogenic, and starts to regress in most mice that are subcutaneously challenged, but then it almost always escapes and recurs and kills the animals. By depleting with anti-CD8, we showed that the initial regression event is dependent on CD8+ T cells. However, depleting with anti-CD4 did not affect regression, but rather blocked recurrence. This result suggested that there was an immunosuppressive or regulatory CD4+ T cell that prevented the regression from being complete and allowed the tumor to recur [13]. However, we found that the regulatory CD4+ T cell was not a classical CD25+ T reg cell, as it was not depleted by treatment in vivo with the PC61, anti-CD25 antibody known to deplete T reg cells [26]. Rather, the regulatory CD4+ cell turned out to be an NKT cell, in that it was absent in CD1d KO mice, in which the tumors did not recur [22]. This led to our definition of a new immunoregulatory pathway in which an immunogenic tumor elicits CTL that can cause regression, but also elicits CD4+ NKT cells, perhaps through a tumor glycolipid presented by CD1d on a dendritic cell (DC), since the tumor itself is CD1d negative. We found that the suppression of tumor immunosurveillance by the NKT cells was dependent on IL-13, not IL-4 [22] (Fig. 1). However, since the CTL that were suppressed did not express IL-13 receptors, we knew that there must be some other steps downstream of the IL-13 [25]. We found that indeed, the IL-13 acted on a cell in the myeloid lineage that was CD11b+ and Gr-1+, but probably CD11c negative [24]. This cell expressed an IL-13 receptor, and was induced by IL-13 to make TGF-β, which was able to suppress the CTL response. The pathway could be completely abrogated by blocking or removing any one of the four key components: by removing the NKT cell or the myeloid cell, or by blocking the IL-13 or the TGF-β. This immunoregulatory circuit seemed to suppress tumor immunosurveillance in tumor models in which T reg cells did not seem to play much of a role (Fig. 1).

Schematic diagram of the NKT cell regulatory pathway. An immunogenic tumor can induce CD8+ T cells that can cause regression, but it also leads to activation of CD1d-retricted CD4+ NKT cells that make IL-13, which in turn induces CD11b+Gr-1+ myeloid cells to make TGF-β, which then suppresses the T cell activation and prevents the tumor immunosurveillance from being complete. Modified from [24] with permission
As this circuit was defined with a tumor that was naturally subject to immunosurveillance because of its expression of a foreign viral antigen, we wanted to know whether the regulatory circuit might be working in the background to prevent immunosurveillance in tumor models in which immunosurveillance was not apparent. Indeed this was the case. We studied the syngeneic BALB/c colon carcinoma CT26, that when injected iv results in lung metastases that will kill the animal, without evidence of spontaneous immunosurveillance. The same pathway appeared to work in this tumor model, in that the number of lung metastases was greatly reduced in CD1d KO mice that lack NKT cells [17]. The protection in CD1d KO mice was dependent on CD8+ T cells, and not further improved by depleting CD4+ T cells, suggesting that the CD4+ regulatory T cell was already absent in CD1d KO mice. The regulatory cell was not depleted by anti-CD25, indicating that it was not a CD25+ T reg cell. Thus, otherwise inapparent immunosurveillance could be unmasked by eliminating NKT cells. Immunosurveillance could also be unmasked by blockade of IL-13 or TGF-β but not by blockade or deficiency of IL-4, consistent with the cytokine mechanism found in the fibrosarcoma model. We conclude that in both tumor models, a regulatory NKT cell initiated a novel pathway suppressing tumor immunosurveillance that would otherwise spontaneously occur, in the absence of a cancer vaccine.
These observations led to an apparent paradox in the role of NKT cells in tumor immunity. A number of laboratories [5–7, 11, 21, 27] had reported protective effects of NKT cells against tumors, mediated by IFN-γ, whereas these current findings suggested a suppressive role mediated by IL-13. Was it the same cell that had opposing effects, depending on the cytokines produced, or were there two different types of NKT T cells mediating these opposite effects? Indeed, there were two classes of NKT cells known, the classical one (type I) expressing a canonical, relatively invariant TCR, using the Vα14Jα18 chain and a limited choice of Vβ chains, and another type called type II with more diverse TCRs [8]. Both are CD1d restricted, and both respond to glycolipids, but to different ones. The type I respond to α-Galactosylceramide (α-GalCer) [11] and a number of related variant lipids [4, 20] as well as cellular lipids [9, 31] and some microbial lipids [4, 28], whereas the type II do not recognize α-GalCer, although a substantial number of them respond to a lipid isolated from myelin called sulfatide [10]. Although the natural ligands for type II NKT cells have not been as thoroughly explored as those for type I, it should be noted that unlike α-GalCer, sulfatides are natural mammalian products present not only in myelin in the nervous system, but also in cell membranes such as those of tumor cells [18]. Human type II NKT cells also recognize phenyl-2,2,4,6,7-pentamethyldihydrobenzofuran-5-sulfonate [29], but its role in vivo and its activity in mice remain to be explored. Thus, we could use two ways to distinguish them, using knockout (KO) mice or specific ligands. CD1d KO mice lack both subsets, whereas Jα18 KO mice lack only type I but retain type II NKT cells, so we can examine their function in KO mice. Also, unlike Th1 and Th2 subsets of CD4+ T cells, where the same TCRs and antigen specificity can be found among clones of T cells within both subsets, and any given antigen stimulates only a small fraction of all the Th1 or Th2 cells, in the case of NKT cells, a single ligand like α-GalCer can stimulate all the type I NKT cells, and a ligand like sulfatide can stimulate a large portion of type II NKT cells. This allows us to selectively stimulate most or all of the cells of a particular subset to determine their function.
First, using KO mice, we found, in four different tumor models studied in our lab and three different collaborative labs, that tumor immunosurveillance was suppressed in Jα18 KO mice that lack type I NKT cells, just as in wild-type mice that have both types, whereas suppression was lost in CD1d KO mice that lack both types of NKT cells [26] (Fig. 2). These findings implied that type II NKT cells were sufficient to suppress tumor immunosurveillance, even without type I NKT cells. Furthermore, using an in vivo killing assay for tumor-specific cytotoxic T lymphocytes (CTL), we found that lytic activity against a specific tumor antigen was increased in tumor-bearing CD1d KO mice, but not in tumor-bearing wild type or Jα18 KO mice [2]. Thus, suppression of tumor immunosurveillance correlated with suppression of CTL activity, and type II NKT cells were sufficient to suppress both. These results provided a solution to the paradox that NKT cells could both contribute to anti-tumor immunity and suppress it, since it was known that the type I NKT cells could protect, and now we found that the type II NKT cells were able to suppress immunity.

Type II NKT cells are sufficient to suppress tumor immunosurveillance. The immunogenic 15–12RM fibrosarcoma grows, regresses, but then recurs in wild type BALB/c mice and in Jα18 KO mice that lack type I NKT cells, but not in CD1d KO mice that lack both type I and type II NKT cells. Five mice per group were injected sc with one million 15–12RM tumor celsl on day 0, and tumor size monitored over time. CD1d KO mice were different at P < 0.05 by a log-rank test from wild type or Jα18KO mice in two different experiments, of which a representative is shown. Modified from [26] with permission
If type I NKT cells contribute to protection and type II suppress that protection, then in the absence of type I NKT cells in Jα18 KO mice, one might predict that the suppression of immunosurveillance would be greater. We tested this hypothesis by looking very early in the course of development of lung metastases after giving the CT26 colon carcinoma cells iv. Indeed, early on, we saw a greater number of lung nodules in the Jα18 KO mice than in the wild type mice, although later they reached the same level. Therefore, we found that indeed, in the absence of type I NKT cells, the suppression of immunosurveillance was greater and the tumor growth was accelerated [2].
To further examine the role of these two subsets of NKT cells, instead of using KO mice, we used lipids that specifically activated one subset or the other. As noted, α-GalCer is a strong agonist for type I NKT cells. OCH is a weaker agonist for type I NKT cells, and has been shown to skew the cytokine pattern more toward a Th2-like profile [15]. Sulfatide is a lipid from myelin found to stimulate type II NKT cells and to ameliorate experimental allergic encephalitis. It was shown using CD1d tetramers loaded with either α-GalCer or sulfatide that the populations of NKT cells recognizing these two ligands are non-overlapping [10].
First, we found that treatment of mice in vivo with α-GalCer protected against CT26 lung metastases and prevented recurrence of the 15–12RM fibrosarcoma [2]. This protection was consistent with protection afforded by α-GalCer treatment in a number of tumor models reported previously. The protection was dependent on type I NKT cells because the α-GalCer had no effect in Jα18 KO mice that lack only type I NKT cells but are otherwise immunologically intact. Since we had found the suppressive effect of NKT cells to be dependent on their production of IL-13, we asked whether skewing of the type I NKT cell cytokine profile more toward Th2 would lead to suppression rather than protection. OCH was confirmed to induce a higher ratio of IL-4 and IL-13 to IFN-γ. However, OCH in vivo also protected against CT26 lung metastases. Therefore, stimulation of type I NKT cells produced protection independent of the ratio of cytokines induced, within the range we could test. However, it must be noted that OCH still induces a significant amount of IFN-γ production, so it would still be of interest to test an agonist that stimulates only Th2 cytokine production to test whether this might give type I NKT cells a more suppressive phenotype.
To examine the role of type II NKT cells, we treated the mice with sulfatide, and found that the number of CT26 lung nodules was increased. This increase in suppression was dependent on a CD4+ T cell, since it was abrogated by CD4 depletion of the mice. Further, the effect was seen in Jα18 KO mice but not in CD1d KO mice, demonstrating that the sulfatide effect was dependent on a cell that was present in the former but not the latter, namely a type II NKT cell. Combined with the CD4 depletion result, this study demonstrated that the suppressive cell responding to sulfatide was a CD4+ type II NKT cell [2].
In view of the opposite roles found for type I and type II NKT cells, we asked whether there was crosstalk between them [2]. We tested this both in vitro and in vivo. First, in vitro, we examined the effect of sulfatide on the proliferation of type I NKT cells induced by α-GalCer. When used to stimulate spleen cells, α-GalCer induced about five times as much thymidine incorporation, as a measure of proliferation, as did sulfatide, consistent with the fact that type I NKT cells are about five times more prevalent among splenocytes than type II NKT cells. When both were given in the same culture, the sulfatide reduced the proliferation induced by the α-GalCer. This was specific for type I NKT cells, not just an effect on proliferation of bystander cells, because we could see the same inhibition of proliferation when we measured it by dilution of CFSE in labeled type I NKT cells stained with CD1d-α-GalCer tetramers. Furthermore, we could rule out the trivial explanation that sulfatide merely competed for binding to CD1d and inhibited that way, because we could independently pulse different antigen-presenting cells with α-GalCer and with sulfatide, wash, and then mix those cells, and still see the inhibition. Thus, it was the activation of type II NKT cells by sulfatide presented by CD1d that inhibited the proliferation of type I NKT cells, not a direct of sulfatide on the cell presenting antigen to the type I NKT cells. Similar inhibition could be seen in cytokine production assays.
Finally, we asked whether the type II NKT cells could also suppress the protective effect of type I NKT cells in vivo. In the 15–12RM fibrosarcoma model, α-GalCer completely prevented tumor recurrence whereas sulfatide did not, and may have even accelerated tumor recurrence, although not quite statistically significantly. However, when sulfatide was given with α-GalCer, it completely abrogated the protection afforded by the α-GalCer [2] (Fig. 3). Similarly, in the CT26 lung metastasis model, α-GalCer markedly reduced the number of lung nodules whereas sulfatide actually increased them. When both were given together, the sulfatide partially reduced the protective effect of the α-GalCer, and conversely, the α-GalCer reduced the number of lung nodules that had been increased by sulfatide. Thus, the type I and II NKT cells appeared to counter-regulate each other in vivo in controlling tumor immunosurveillance [2].

Type II NKT cells suppress the protective effect of type I NKT cells. Wild type BALB/c mice were injected sc as in Fig. 2 with a million 15–12RM tumor cells and then injected the same day ip with either vehicle, α-GalCer (4 μg/mouse), sulfatide (25 μg/mouse), or both (with sulfatide injected 15–30 minutes later than α-GalCer to avoid competition). The complete protection from recurrence afforded by the α-GalCer activation of type I NKT cells was completely abrogated by treatment with sulfatide (P = 0.0001 by log rank test). Modified from [2] with permission
In summary, we found that in addition the now-classical T reg cell that can inhibit tumor immunosurveillance in some tumor models [16, 19], there is a second immunoregulatory cell, the type II NKT cell, that can suppress immunosurveillance in tumor models in which the T reg cell does not seem to play a role. We have characterized the regulatory pathway initiated by this suppressive NKT cell, involving production of IL-13 that induces a cell in the myeloid lineage to produce TGF-β that inhibits CTL induction against the tumor. Type I NKT cells protect against tumors whereas type II NKT cells can suppress. Type II NKT cells also suppress the induction of CTL specific for tumor antigens in tumor bearing mice also. Type II NKT cells reduce the protective efficacy of type I NKT cells and show greater suppression in the absence of type I NKT cells, indicating that they can counter-regulate each other. Overall, these results provide a solution to the paradox of opposite roles for NKT cells in tumor immunity. They provide a new functional activity for the poorly understood type II NKT cells. In addition, they define a new immunoregulatory axis of type I vs type II NKT cells that cross-regulate each other in a way analogous to the axis between Th1 and Th2 cells [2, 23]. This new immunoregulatory axis may have broader implications beyond tumor immunity, since the cytokines produced rapidly by NKT cells may set the balance of cytokines that determines the quality of the subsequent adaptive immune response. Also, NKT cells play a regulatory role in autoimmune disease and asthma [1, 14, 30], so this axis may have an impact in these diseases as well. The relationship between this immunoregulatory axis and T reg cells is being investigated. Inhibition of type II NKT cells may synergize with vaccines and immunotherapies of cancers and chronic viral infections. Thus, the balance along this axis may determine the outcome of tumor immunosurveillance as well as influence the efficacy of anti-cancer vaccines and immunotherapy.
References
Akbari O, Stock P, DeKruyff RH, Umetsu DT (2003) Role of regulatory T cells in allergy and asthma. Curr Opin Immunol 15:627
Ambrosino E, Terabe M, Halder RC, Peng J, Takaku S, Miyake S, Yamamura T, Kumer V, Berzofsky JA (2007) Cross-regulation between type I and type II NKT cells in regulating tumor immunity: a new immunoregulatory axis. J Immunol 179:5126
Bendelac A, Savage PB, Teyton L (2007) The biology of NKT cells. Annu Rev Immunol 25:297
Brutkiewicz RR (2006) CD1d ligands: the good, the bad, and the ugly. J Immunol 177:769
Crowe NY, Smyth MJ, Godfrey DI (2002) A critical role for natural killer T cells in immunosurveillance of methylcholanthrene-induced sarcomas. J Exp Med 196:119
Crowe NY, Coquet JM, Berzins SP, Kyparissoudis K, Keating R, Pellicci DG, Hayakawa Y, Godfrey DI, Smyth MJ (2005) Differential antitumor immunity mediated by NKT cell subsets in vivo. J Exp Med 202:1279
Cui J, Shin T, Kawano T, Sato H, Kondo E, Toura I, Kaneko Y, Koseki H, Kanno M, Taniguchi M (1997) Requirement for Valpha14 NKT cells in IL-12-mediated rejection of tumors. Science 278:1623
Godfrey DI, MacDonald HR, Kronenberg M, Smyth MJ, Van Kaer L (2004) NKT cells: what’s in a name? Nat Rev Immunol 4:231
Gumperz JE, Roy C, Makowska A, Lum D, Sugita M, Podrebarac T, Koezuka Y, Porcelli SA, Cardell S, Brenner MB, Behar SM (2000) Murine CD1d-restricted T cell recognition of cellular lipids. Immunity 12:211
Jahng A, Maricic I, Aguilera C, Cardell S, Halder RC, Kumar V (2004) Prevention of Autoimmunity by Targeting a Distinct, Noninvariant CD1d-reactive T Cell Population Reactive to Sulfatide. J Exp Med 199:947
Kawano T, Cui J, Koezuka Y, Toura I, Kaneko Y, Motoki K, Ueno H, Nakagawa R, Sato H, Kondo E, Koseki H, Taniguchi M (1997) CD1d-restricted and TCR-mediated activation of valpha14 NKT cells by glycosylceramides. Science 278:1626
Kronenberg M (2005) Toward an understanding of NKT cell biology: progress and paradoxes. Annu Rev Immunol 23:877
Matsui S, Ahlers JD, Vortmeyer AO, Terabe M, Tsukui T, Carbone DP, Liotta LA, Berzofsky J (1999) A model for CD8+ CTL tumor immunosurveillance and regulation of tumor escape by CD4 T cells through an effect on quality of CTL. J Immunol 163:184
Meyer EH, Goya S, Akbari O, Berry GJ, Savage PB, Kronenberg M, Nakayama T, DeKruyff RH, Umetsu DT (2006) Glycolipid activation of invariant T cell receptor+ NK T cells is sufficient to induce airway hyperreactivity independent of conventional CD4+ T cells. Proc Natl Acad Sci USA 103:2782
Oki S, Chiba A, Yamamura T, Miyake S (2004) The clinical implication and molecular mechanism of preferential IL-4 production by modified glycolipid-stimulated NKT cells. J Clin Invest 113:1631
Onizuka S, Tawara I, Shimizu J, Sakaguchi S, Fujita T, Nakayama E (1999) Tumor rejection by in vivo administration of anti-CD25 (interleukin-2 receptor alpha) monoclonal antibody. Cancer Res 59:3128
Park JM, Terabe M, van den Broeke LT, Donaldson DD, Berzofsky JA (2004) Unmasking immunosurveillance against a syngeneic colon cancer by elimination of CD4+ NKT regulatory cells and IL-13. Int J Cancer 114:80
Roberts DD (1986) Sulfatide-binding proteins. Chem Phys Lipids 42:173
Shimizu J, Yamazaki S, Sakaguchi S (1999) Induction of tumor immunity by removing CD25+ CD4+ T cells: a common basis between tumor immunity and autoimmunity. J Immunol 163:5211
Sidobre S, Hammond KJ, Benazet-Sidobre L, Maltsev SD, Richardson SK, Ndonye RM, Howell AR, Sakai T, Besra GS, Porcelli SA, Kronenberg M (2004) The T cell antigen receptor expressed by Valpha14i NKT cells has a unique mode of glycosphingolipid antigen recognition. Proc Natl Acad Sci USA 101:12254
Smyth MJ, Thia KY, Street SE, Cretney E, Trapani JA, Taniguchi M, Kawano T, Pelikan SB, Crowe NY, Godfrey DI (2000) Differential tumor surveillance by natural killer (NK) and NKT cells. J Exp Med 191:661
Terabe M, Matsui S, Noben-Trauth N, Chen H, Watson C, Donaldson DD, Carbone DP, Paul WE, Berzofsky JA (2000) NKT cell-mediated repression of tumor immunosurveillance by IL-13 and the IL-4R-STAT6 pathway. Nat Immunol 1:515
Terabe M, Berzofsky JA (2007) NKT cells in immunoregulation of tumor immunity: cross-regulation between two subsets. Trends Immunol 28:491
Terabe M, Matsui S, Park J-M, Mamura M, Noben-Trauth N, Donaldson DD, Chen W, Wahl SM, Ledbetter S, Pratt B, Letterio JJ, Paul WE, Berzofsky JA (2003) Transforming Growth Factor-b production and myeloid cells are an effector mechanism through which CD1d-restricted T cells block Cytotoxic T Lymphocyte-mediated tumor immunosurveillance: abrogation prevents tumor recurrence. J Exp Med 198:1741
Terabe M, Park JM, Berzofsky JA (2003) Role of IL-13 in negative regulation of anti-tumor immunity. Cancer Immunol Immunother 53:79
Terabe M, Swann J, Ambrosino E, Sinha P, Takaku S, Hayakawa Y, Godfrey DI, Ostrand-Rosenberg S, Smyth MJ, Berzofsky JA (2005) A nonclassical non-Va14Ja18 CD1d-restricted (type II) NKT cell is sufficient for down-regulation of tumor immunosurveillance. J Exp Med 202:1627
Toura I, Kawano T, Akutsu Y, Nakayama T, Ochiai T, Taniguchi M (1999) Cutting edge: inhibition of experimental tumor metastasis by dendritic cells pulsed with alpha-galactosylceramide. J Immunol 163:2387
Tupin E, Kinjo Y, Kronenberg M (2007) The unique role of natural killer T cells in the response to microorganisms. Nat Rev Microbiol 5:405
Van Rhijn I, Young DC, Im JS, Levery SB, Illarionov PA, Besra GS, Porcelli SA, Gumperz J, Cheng TY, Moody DB (2004) CD1d-restricted T cell activation by nonlipidic small molecules. Proc Natl Acad Sci USA 101:13578
Wilson SB, Delovitch TL (2003) Janus-like role of regulatory iNKT cells in autoimmune disease and tumour immunity. Nat Rev Immunol 3:211
Zhou D, Mattner J, Cantu C 3rd, Schrantz N, Yin N, Gao Y, Sagiv Y, Hudspeth K, Wu YP, Yamashita T, Teneberg S, Wang D, Proia RL, Levery SB, Savage PB, Teyton L, Bendelac A (2004) Lysosomal glycosphingolipid recognition by NKT cells. Science 306:1786
Acknowledgments
We thank our collaborators Elena Ambrosino, Mark Smyth, Jeremy Swann, Yoshihiro Hayakawa, Dale Godfrey, Suzanne Ostrand-Rosenberg, Pratima Sinha, Shun Takaku, Judy Peng, Takashi Yamamura, Sachiko Miyake, Vipin Kumar, and Ramesh Halder for their most valuable collaboration, without which the work reviewed here would not have been possible.
Author information
Authors and Affiliations
Corresponding authors
Additional information
This article is a symposium paper from the conference “Progress in Vaccination against Cancer 2007 (PIVAC 7)”, held in Stockholm, Sweden, on 10–11 September 2007.
Rights and permissions
About this article
Cite this article
Berzofsky, J.A., Terabe, M. A novel immunoregulatory axis of NKT cell subsets regulating tumor immunity. Cancer Immunol Immunother 57, 1679–1683 (2008). https://doi.org/10.1007/s00262-008-0495-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00262-008-0495-4