
Abstract
Purpose
To retrospectively investigate the value of magnetic resonance imaging (MRI) in detecting complications following pancreas transplant.
Materials and methods
Institutional review board approved this retrospective HIPAA-compliant study and waived informed patient consent. We identified all allograft pancreas transplant patients at our institution from 2001 to January 2014 who had all pertinent post-transplant imaging and clinical data available. Transplant type was documented. Patients were divided into two groups according to post-transplant period (group A; <12 months, group B; ≥12 months). We evaluated the parenchymal enhancement using contrast-enhanced MRI of the allograft and determined the mean percentage of parenchymal enhancement (MPPE) overall and in various abnormalities, the vessel patency, any peripancreatic fluid collection, and the ductal anatomy. We correlated these with clinical results using t test, χ 2, and Fisher’s exact test; p < 0.05 was considered significant.
Results
51 patients (34 male, mean age 43.7 years) were identified, 28 (55%) of whom had abnormal imaging findings; transplant rejection-related necrosis (n = 7), fluid collections (n = 7), vascular stenosis (n = 4), isolated venous thromboses (n = 3), acute pancreatitis (n = 3), pancreatic and peripancreatic abscesses (n = 2), pseudoaneurysm (n = 1), and small-bowel obstruction (n = 1). Pre vs. post-contrast pancreatic MPPE at 1 min was 120% in the normal allografts and 115% in the allografts with pancreatitis and without necrosis (p > 0.05). MPPE at 1 min was only 9% in the allografts rejections with necrosis/infarction. More complications were found in group A than group B (p < 0.05).
Conclusions
Contrast-enhanced MRI is useful for the non-invasive assessment of pancreas transplant complications.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Pancreas allograft transplant has proven to be reliable to normalize blood sugar level and to improve quality of life in patients with Type 1 diabetes [1]. Types of pancreas transplant include isolated pancreas transplant, pancreas after kidney transplant (PKT) or simultaneous pancreas and kidney (SPK) transplant, and multi-visceral transplant. PKT or SPK transplant is increasingly used for treating end-stage renal disease secondary to insulin-dependent diabetes mellitus.
Despite significant advancements made in recipient and donor selection, surgical techniques, post-operative treatment, and pancreas transplants still have a higher rate of postsurgical complications as compared to other solid organ transplants [2]. Unfortunately, no reliable clinical or readily performed laboratory tests directly related to the function of the allograft pancreas have been established for the diagnosis of complications, other than routine pancreatic enzyme tests. To avoid the perceived risk of complications, few pancreatic biopsy procedures for allograft pancreas are performed.
It can be challenging to interpret the various complications of allograft pancreas, using ultrasonography (US) or computed tomography (CT) [3–5]. US can detect the change in blood flow but cannot assess vessel contour abnormality. US is unable to reliably identify other complications including rejection or pancreatitis as it is often unable to visualize the transplanted pancreas due to overlapping bowel gas. While CT is widely available, relatively inexpensive, and allows rapid image acquisition, yet, the risk of contrast-induced nephropathy has limited its use in repeated examinations beyond the immediate post-operative period.
Magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) with and without intravenous (IV) contrast medium have become an invaluable imaging modality in cases of impaired pancreatic function or suspected post-operative complications such as acute pancreatitis, parenchymal necrosis, pancreatic ductal injuries, and vascular complications [3–8]. The purpose of our study is to review our experience in MRI in evaluating complications after allograft pancreas transplant.
Materials and methods
Patients
Institutional review board (IRB) approved this retrospective HIPAA-compliant study and waived informed patient consent. Pancreas grafts were procured using an en-bloc technique with aortic flush [5–7]. The donor iliac artery “Y” graft was anastomosed to the recipient common iliac artery (usually on the right side) or rarely to the aorta, and systemic venous drainage was established to the recipient right common iliac vein or the vena cava. The enteric drainage of the pancreas was created using an end-to-end circular stapler to anastomose the donor duodenum to the proximal small bowel of the recipient.
We reviewed clinical and radiologic databases at our institution from January 2001 to January 2014, and identified all patients who underwent allograft pancreas transplant. We then identified those patients who underwent abdominal MRI examination following transplant, and who had all pertinent imaging available on our radiology archive and clinical follow-up information. Four patients with severe artifacts on MRI (e.g., due to motion) were excluded. The reason for examination was noted, and confirmation that the indication for MRI was likely attributable to post-transplant disorders was made. We documented the reason for transplant and the type of transplant surgery performed.
Magnetic resonance imaging
All MRI exams were performed with a 1.5 Tesla magnet (Avanto; Siemens Medical Solutions, Malvern, PA) or 3.0 Tesla magnet (TIM Trio; Siemens Medical Solutions, Malvern, PA) using surface phased-array coil. After three-plane scout view acquisition, axial T1-weighted unenhanced fast low-angle shot (FLASH) gradient echo (GRE) sequence and coronal and axial half-Fourier acquisition single-shot turbo spin-echo (HASTE) with relaxation enhancement sequences were employed. All patients underwent IV contrast enhancement exams, 10 patients had MRA exams, and 14 patients had MRCP exams.
For MRCP, the pancreatic duct was imaged using a single-shot fast spin-echo pulse sequence, with a single 40-mm-thick coronal “slab” positioned over the pancreas. The matrix size was 256 × 256; the field of view (FOV) varied from patient to patient and was typically 22 × 22 cm. Fat saturation was used in the sequence. Acquisition time was approximately 1–2 s per scan and obtained during breath holding. A thin slice coronal T2-weighted sequence was also employed along with a respiratory synchronized three-dimensional turbo spin-echo sequence.
Magnetic resonance angiography (MRA) and contrast-enhanced MRI were performed using a T1-weighted fat-saturation GRE sequence volumetric interpolated breath-hold examination (VIBE). MRA data were reconstructed with maximum intensity projection (MIP) and multi-planner reformation (MPR). For IV contrast material, 0.1 mmol of gadobenate dimeglumine (Multihance; Bracco, Princeton, NJ) per kilogram of body weight was injected at 2 mL/s. In order to remove the high signal from overlying stomach and duodenum, the patient either fasted for 4–6 h before the examination was given 300 mL of ferumoxsil oral suspension as a negative contrast agent (Gastromark, Mallinckrodt Medical, Raleigh, NC), or given pineapple juice [4]. Two-phase imaging was obtained at approximately 1 and 5 min after injection of the contrast agent.
Image and related data analysis
All the images were retrospectively reviewed by two experienced abdominal radiologists with 12 and 14 years of experience. The allograft mean percentage of parenchymal enhancement (MPPE) was analyzed, MPPE = [contrast-enhanced mean glandular signal intensity (MGSI) − unenhanced MGSI)/(unenhanced MGSI)] × 100%. The MGSI for the pancreas allograft was derived on the unenhanced T1 imaging by averaging two regions of interest (ROIs) from a representative image section that encompassed the allograft. Focal areas of signal intensity abnormalities were excluded from sampling due to heterogeneous pancreatic enhancement. The same ROIs were measured on the post-contrast-enhanced images. Patients were divided into two groups: less than 12 months and greater than or equal to 12 months since the time of transplant. The differences in morbidities due to complications between the two groups were compared. MPPE was compared between normal allografts and particular disease states.
Statistical analysis
For analyzing categorical frequency data, the χ 2 and Fisher’s exact probability procedures were applied. For comparing continuous variables in two independent groups, the t test and Mann–Whitney test were used. A value of p < 0.05 was considered significant. Receiver operating characteristic curve analysis was performed, and the area under the curve was determined for the MPPE variables. Based on this analysis, a threshold was determined for the most accurate measurement.
Results
51 allograft pancreatic transplant patients (34 male, mean age 43.7 years; age range 20-61 years) were identified. Among those 51 patients, 32 (63%) underwent SPK transplant; 9 (18%) patients had an isolated pancreas transplant; 5 (10%) patients underwent a PKT; 4 (8%) patients had a multi-visceral transplant including the pancreas, liver, and small bowel; and 1 (2%) patient had a simultaneous pancreas and lung transplant. All patients were referred for MRI exams because of abnormal laboratory assay results such as elevated blood glucose, amylase and lipase, or clinical findings such as abdominal pain, fever, or increased venous pulsation.
There was no evidence of glandular parenchymal or peripancreatic allograft-related complications in 23 patients.
Pancreatic allografts removals were performed in 7 patients due to infarction/necrosis, severe hyperglycemia that required insulin administration, and severe unremitting abdominal pain. The MRI findings were correlated with the histopathologic evidence of severe necrosis or infarction of the 7 allograft specimens. Four patients with an allograft rejection without necrosis or infarction were treated with corticosteroids and were followed up for more than 1 year.
Table 1 displays all MPPE measurements. MPPE measurements at 1 min were 120% in the normal allografts and 9% in the allograft rejections with necrosis or infarction. The MPPE in normal allografts rose approximately 20% from 120% at 1 min to 139% at 5 min measured time intervals (Fig. 1). There was a sensitivity of 74% when the MPPE cutoff value was set at 100% to represent the normal value. The specificity was 100% when the MPPE cutoff value was set at 20% to determine allograft necrosis or infarction.

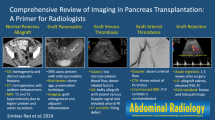
47-year-old man with normal transplanted pancreas. A Transverse T2-weighted image with fat saturation shows a normal transplanted pancreas with normal size and homogeneous signal intensity (arrow). B, C Transverse T1-weighted image with fat saturation (B) shows mean signal intensity (SI) of 151.6 at 1 min post-contrast enhancement (C) shows mean SI of 348.8 at 5 min, providing a mean percentage of parenchymal enhancement (MPPE) of 130.0%.
The pancreas allograft was hyperintensity on T2WI and showed no enhancement when it was in a state of complete necrosis or infarction. These removed allografts with necrosis or infarction had a mean MPPE well below that of normal patients, and remained at 9% and 14% at 1 and 5 min, respectively (Fig. 2).

20-year-old woman with complete pancreatic necrosis of the transplanted pancreas. A, B Transverse T1-weighted image with fat saturation (A) shows mean signal intensity (SI) of 111.4 at 1 min post-contrast enhancement (B) shows mean SI of 114.3 at 5 min providing a mean percentage of parenchymal enhancement (MPPE) of 2.6%.
In three patients with acute pancreatitis, the MPPE measurements in the allografts at 1 and 5 min were 115% and 149%, respectively (Fig. 3). There was no significant difference in this group compared with the normal allografts (p > 0.05). All the patients with acute pancreatitis showed similar imaging findings of non-allograft pancreatitis such as edema, peripancreatic fluid collection, enlargement and heterogeneity of the glandular parenchyma, and elevated amylase. The peripancreatic fluid collections were more common and extensive in the allograft pancreatitis patients than in the rejection allograft patients. All the acute pancreatitis patients recovered with treatment.

25-year-old woman with acute pancreatitis of the transplanted pancreas. A, B Transverse T1-weighted image with fat saturation (A) shows edema of pancreas with a mean signal intensity (SI) of 179.1 at 1 min post-contrast enhancement (B) shows mean SI of 351.6 at 5 min providing a mean percentage of parenchymal enhancement (MPPE) of 96.4%.
Other complications included 7 patients with fluid collections alone, 4 patients with vascular stenosis at the anastomotic sites, and 3 patients with non-allograft venous thrombosis. These included one patient with left portal vein thrombosis, one patient with main portal vein thrombosis, and one patient with middle hepatic vein thrombosis. 2 patients developed pancreatic parenchymal and peripancreatic abscesses (Fig. 4). One patient had a pseudoaneurysm. One patient developed a partial small-bowel obstruction due to extensive adhesions. There were no abnormal pancreatic ductal abnormalities on secretin-stimulated MRCP exams.

40-year-old man with abscess of transplanted pancreas and peripancreatic tissue. A Coronal T2-weighted image shows edema of pancreas (long arrow), heterogeneous hyperintensity of pancreas (short arrow). B, C Coronal (B) and transverse (C) T1-weighted image post-contrast enhancement shows rim enhancement of transplanted pancreatic parenchyma (long arrow) and peripancreatic tissue (short arrow).
When the patients were divided into two groups (<12-month group and ≥12-month group) according to the time of post-transplant (Fig. 5), the <12-month group was significantly more likely to have an abnormality on MRI (p < 0.05).

Population pyramid graph of MRI findings in different group patients with post-pancreas transplant. X axis refers to number of patients, Y axis refers to MRI findings (0 = normal finding, 1 = fluid collection, 2 = necrosis, 3 = vascular stenosis, 4 = pancreatitis, 5 = venous thrombosis, 6 = abscess, 7 = pseudoaneurysm, 8 = bowel obstruction). There is significant difference in rate of complications before and after 12 months of pancreas transplant (p < 0.05).
Discussion
Pancreas transplant is the most reliable method to achieve normoglycemia in a select group of Type 1 diabetics that qualify for this procedure. With improvements in surgical technique, preservation solutions, and immunosuppression, enteric drainage rather than bladder drainage in combination with systemic venous drainage has become the preferred implantation technique at most centers. In order to decrease tension on the enteric anastomosis, many centers have also begun to place the pancreas with the head facing upward rather than toward the pelvis, and have moved the vascular anastomoses cephalad as well using common iliac artery and the vena cava or the common iliac vein rather than the external iliac vessels. As a result of this modified placement, the pancreas is now situated deeper, higher, and more posteriorly in the abdomen rendering the allograft more difficult to visualize with US imaging. And it is difficult to detect complications using CT without IV contrast enhancement.
Therefore, it is important to develop a sensitive and non-invasive technique to detect complication in a pancreas allograft. Small cohort studies have shown that MRI has become valuable in detecting pancreatic allograft complications [7–13]. Currently, in our institution, MRI is used as a second-line imaging modality for post-allograft patients who could not be adequately evaluated by CT or US.
MRI without IV contrast enhancement can reveal abnormalities of pancreatic allograft, but there is no specificity. Prior studies [14–18] demonstrated that the unenhanced MRI had variable results and limitations in evaluating dysfunctional pancreatic allograft. The allograft edema and heterogeneity that occurs in rejection can be identified by conventional sequence including T1- and T2-weighted imaging [10, 11, 13–19], parenchymal edema alone is not a specific finding of allograft rejection, and it is difficult to differentiate rejection from acute pancreatitis or ischemia using the finding of edema. Fernandez et al. [15] demonstrated that the percentage of post-contrast enhancement in normal allograft was greater than that in dysfunctional allograft. In their study, the mean percentage of enhancement at 1 min was 98% in 6 normal allografts as compared with 42% in 6 dysfunctional allografts. Krebs et al. [11] compared the results of MRI with histopathologic analysis in 25 patients and found that the percentage of enhancement (at 1 min) in the normal group was greater, 106%, compared with 50% enhancement in the dysfunctional group. In our study, the percentage of enhancement in the normal allografts was greater, 120%, compared with 9% in the necrotic allografts. These results are similar to those of Fernandez et al. [15] and Krebs et al. [11].
Allograft pancreatitis usually occurs secondary to impaired microcirculation. It may be suspected in the presence of elevated serum amylase and lipase levels. The diagnosis of allograft pancreatitis is suggested when changes isolated to the pancreas including peripancreatic fluid associated with an ill-defined pancreas and edema are shown [12]. A peripancreatic fluid collection, elevated amylase without elevated glucose, and imaging follow-up after pancreatitis is suspected may be important in differentiating acute pancreatitis from rejection.
Graft thrombosis either venous or arterial that leads to allograft necrosis or infarction is one of major causes of allograft loss. It can occur secondary to a vascular graft anastomotic abnormality or microvascular disease [11]. Another reason for thrombosis usually due to severe rejection with alloimmune arteritis and occlusion of small vessels. The relatively smaller microcirculatory blood flow of transplanted pancreas (1.3% of cardiac output) may account for the accordingly higher incidence of thrombosis involving the pancreatic graft [20].
It is important to detect total allograft thrombosis with necrosis/infarction, if it is identified, then allograft pancreatectomy is usually required to avoid severe systemic complications [21]. In our study, the earliest thrombosis identified specifically by MRI occurred at transplant post-op day 5 and the furthest post-transplant episode occurred at 20 months. The allograft with an MPPE of 9% had necrosis or infarction and were identified using contrast-enhanced MRI. In our study, 7 allografts were explanted secondary to allograft thrombosis that resulted in necrosis.
MRA was found to be a reliable imaging technique to identify vascular complications such as occlusion, stenosis, and infarction [22, 23]. In our study, 4 patients with stenosis of vascular anastomosis were detected.
Fluid collections are the most common complication after a pancreas transplant. The clinical presentation and imaging findings are similar to those of an enteric leak. MRI can also be helpful to identify fluid collection and distinguish it from a hematoma by detecting T1 hyperintensity. Infection may occur in 50% patients of pancreatic allografts [24, 25]. Pseudoaneurysm is associated with a risk of hemorrhage and a higher incidence of graft loss [26–30]. Pseudoaneurysms typically develop in the early post-operative period as either a technical complication or as a result of infection or abscess adjacent to the arterial anastomosis. In our study, one pseudoaneurysm resulted in bleeding presenting at transplant post-op day 5.
The most common intestinal complications following the pancreas transplant are small-bowel obstruction, anastomotic leak, and pseudomembranous or cytomegalovirus colitis. Small-bowel obstruction due to adhesion or internal herniation secondary to intraperitoneal placement of the allograft can also occur. These obstructions secondary to adhesions tend to occur in the anterior abdomen and are usually low grade [31].
This study had several limitations. In our institution, MRI examination is not the primary imaging modality for evaluating the complications of pancreas allograft. MRI is used only for the cases that could not be adequately evaluated using US or CT. In order to review MRI features of a pancreas allograft, we had to exclude abundant CT and US exams of the patients after pancreas transplants. Some patients had to be excluded due to severe MRI artifacts or the inability to administer contrast enhancement. Thus our patient population may not reflect the distribution of complications of pancreas transplants in our institution.
In conclusion, this study demonstrates that MRI evaluation is a valuable non-invasive, accurate imaging modality to differentiate, and detect post-transplant complications.
References
Robertson RP, Sutherland DE, Kendall DM, et al. (1996) Metabolic characterization of long-term successful pancreas transplants in type 1 diabetes. J Invest Med 44:549–555
Troppmann C, Gruessner AC, Dunn DL, et al. (1998) Surgical complications requiring early relaparotomy after pancreas transplantation: a multivariate risk factor and economic impact analysis of the cyclosporine era. Ann Surg 227:255–268
Sansalone CV, Maione G, Aseni P, et al. (2005) Surgical complications are the main cause of pancreatic allograft loss in pancreas-kidney transplant recipients. Transplant Proc 37:2651–2653
Akisik MF, Sandrasegaran K, Aisen AA, et al. (2006) Dynamic secretin-enhanced MR cholangiopancreatography. Radiographics 26:665–677
Gruessner AC (2011) 2011 update on pancreas transplantation: comprehensive trend analysis of 25,000 cases followed up over the course of twenty-four years at the international pancreas transplant registry (IPTR). Rev Diabet Stud 8:6–16
Gaber AO, Shokouh-Amiri H, Grewal HP, et al. (1993) A technique for portal pancreatic transplantation with enteric drainage. Surg Gynecol Obstet 177:417–419
Fridell JA, Rogers J, Stratta RJ (2010) The pancreas allograft donor: current status, controversies, and challenges for the future. Clin Transplant 24:433–449
Wong JJ, Krebs TL, Klassen DK, et al. (1996) Sonographic evaluation of acute pancreatic transplant rejection: morphology-Doppler analysis versus guided percutaneous biopsy. AJR 166:803–807
Aideyan OA, Schmidt AJ, Trenkner SW, et al. (1996) CT-guided percutaneous biopsy of pancreas transplants. Radiology 201:825–828
Vandermeer FQ, Manning MA, Frazier AA, et al. (2012) Imaging of whole-organ pancreas transplants. Radiographics 32:411–435
Krebs TL, Daly B, Wong-You-Cheong JJ, et al. (1999) Acute pancreatic transplant rejection: evaluation with dynamic contrast-enhanced MR imaging compared with histopathologic analysis. Radiology 210:437–442
Benz S, Bergt S, Obermaier R, et al. (2001) Impairment of microcirculation in the early reperfusion period predicts the degree of graft pancreatitis in clinical pancreas transplantation. Transplantation 71:759–763
Hagspiel KD, Nandalur K, Burkholder B, et al. (2005) Contrast-enhanced MR angiography after pancreas transplantation: normal appearance and vascular complications. AJR 184:465–473
Yuh WT, Hunsicker LG, Nghiem DD, et al. (1989) Pancreatic transplants: evaluation with MR imaging. Radiology 170:171–177
Fernandez MP, Bernadino ME, Neylan JF, et al. (1991) Diagnosis of pancreatic transplant dysfunction: value of gadopentetate dimeglumine-enhanced MR imaging. AJR 156:1171–1176
Kelcz F, Sollinger HW, Pirsh JD (1991) MRI of the pancreas transplant: lack of correlation between imaging and clinical status. Magn Reson Med 21:30–38
Yuh WT, Wiese JA, Abu-Yousef MM, et al. (1988) Pancreatic transplant imaging. Radiology 167:679–683
Vahey TN, Glazer GM, Francis IR, et al. (1988) MR diagnosis of pancreatic transplant rejection. AJR 150:557–560
Nakhleh RE, Sutherland DE (1992) Pancreas rejection. Significance of histopathologic findings with implications for classification of rejection. Am J Surg Pathol 16:1098–1107
Boeve WJ, Kok T, Tegzess AM, et al. (2001) Comparison of contrast enhanced MR-angiography-MRI and digital subtraction angiography in the evaluation of pancreas and/or kidney transplantation patients: initial experience. Magn Reson Imaging 19:595–607
Corry RJ, Nghiem DD, Schulak JA, et al. (1986) Surgical treatment of diabetic nephropathy with simultaneous pancreatic duodenal and renal transplantation. Surg Gynecol Obstet 162:547–555
Dobos N, Roberts DA, Insko EK, et al. (2005) Contrast-enhanced MR angiography for evaluation of vascular complications of the pancreatic transplant. Radiographics 25:687–695
Hagspiel KD, Nandalur K, Pruett TL, et al. (2007) Evaluation of vascular complications of pancreas transplantation with high-spatial-resolution contrast-enhanced MR angiography. Radiology 242:590–599
Goodman J, Becker YT (2009) Pancreas surgical complications. Curr Opin Organ Transplant 14:85–89
Troppmann C (2010) Complications after pancreas transplantation. Curr Opin Organ Transplant 15:112–118
Tan M, Di Carlo A, Stein LA, et al. (2001) Pseudoaneurysm of the superior mesenteric artery after pancreas transplantation treated by endovascular stenting. Transplantation 72:336–338
Khan TF, Ciancio G, Burke GW 3rd, et al. (1999) Pseudoaneurysm of the superior mesenteric artery with an arteriovenous fistula after simultaneous kidney-pancreas transplantation. Clin Transplant 13:277–279
Paduch DA, Conlin M, Dematos A, et al. (2000) Arterial duodenovesical fistula after simultaneous pancreas and kidney transplantation. J Urol 164:1296
Green BT, Tuttle-Newjall J, Suhocki P, et al. (2004) Massive gastrointestinal hemorrhage due to rupture of a donor pancreatic artery pseudoaneurysm in a pancreas transplant patient. Clin Transplant 18:108–111
Fujita S, Fujikawa T, Mekeel KL, et al. (2006) Successful endovascular treatment of a leaking pseudoaneurysm without graft loss after simultaneous pancreas and kidney transplantation. Transplantation 82:717–718
Lall CG, Sandrasegaran K, Maglinte DT, et al. (2006) Bowel complications seen on CT after pancreas transplantation with enteric drainage. AJR 187:1288–1295
Disclosures
This project was performed at Department of Radiology and Imaging Sciences, Indiana University School of Medicine.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Liu, Y., Akisik, F., Tirkes, T. et al. Value of magnetic resonance imaging in evaluating the pancreatic allograft transplant complications. Abdom Imaging 40, 2384–2390 (2015). https://doi.org/10.1007/s00261-015-0408-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-015-0408-x