
Abstract
Purpose: Ketamine is a commonly abused recreational drug in Southeast Asia. There are emerging reports on ketamine abuse causing liver injury and biliary dilatation. This retrospective study aims to investigate the clinical and radiological features of this condition. Methods: A retrospective search in the database of our institute was performed from January 2008 to February 2014 for patients who were ketamine abusers, with deranged liver function and/or epigastric pain, and had computed tomography of the abdomen or magnetic resonance cholangiopancreatography. Patient demographics, clinical data, and radiological findings were reviewed. Results: Twenty-six patients (11 male and 15 female) were included in this study. Eighteen (69 %) patients had fusiform dilatation of the common bile ducts (CBDs) without evidence of intrinsic or extrinsic obstruction, and non-dilated intrahepatic ducts. The degree of CBD dilatation correlated with duration of abuse. In five patients who achieved abstinence, the CBD dilatation showed improvement. Conclusions: Ketamine-related cholangiopathy manifested as fusiform dilatation of the CBD without evidence of obstructive lesions. Severity of CBD dilatation appears to be correlated with the duration of ketamine, and the condition is potentially reversible in abstinent patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Ketamine is an N-methyl-d-aspartate receptor antagonist and is used as a sedative agent in clinical practice. However, owing to its hallucinogenic properties, ketamine is also a commonly abused recreational drug in Hong Kong and Southeast Asia. According to the statistics from the Central Registry of Drug Abuse [1], ketamine is the most commonly abused psychotropic substance, constituting 31.5 % of all drug abusers in Hong Kong. In the US, it was estimated that 2.3 million persons aged 12 or above had used ketamine in their lifetime [2]. The effect of ketamine abuse on the urinary bladder has been well established [3, 4]. Recently, there are several case reports suggesting that liver injury and biliary dilatation could be associated with ketamine abuse [5–10]. The imaging features of ketamine-related cholangiopathy have not been well established in the literature. This study aims to investigate the clinical and radiological features of ketamine-associated cholangiopathy.
Methods
We performed a retrospective search in our database from January 2008 to February 2014. The keyword “ketamine” was used to search for all computed tomography (CT) and magnetic resonance imaging (MRI) examinations. Patients who had CT of the abdomen or MR cholangiopancreatography (MRCP) performed in our institute, with history of ketamine abuse, who had abdominal pain and/or abnormal liver function tests were included in the study. Patients were kept nil per oral for 4 h prior to CT and MRCP examinations. Patient demographics, duration of ketamine abuse, clinical symptoms, clinical follow-up details, liver function tests, endoscopic retrograde cholangiopancreatography (ERCP) findings (if available), liver biopsy results (if available), and the imaging findings were recorded.
Abnormal liver function tests were defined as elevation of liver biochemistry at least two times above the upper limit of normal [11]. The type of liver function abnormality was defined as cholestatic when the alkaline phosphatase (ALK) was elevated, and hepatocellular when the alanine aminotransferase (ALT) was elevated.
The MRCP was performed using 3.0T MRI (Philips X-series Best, Netherlands) with standardized protocol, including axial T1-weighted, axial T2-weighted with fat saturation, and a heavily T2-weighted sequence in oblique coronal plane for imaging of the biliary system, with 1 mm contiguous slices. Subsequent reconstruction with maximum intensity projection was performed. The CT scans were performed using 64-detector helical CT (Lightspeed 64 VCT, GE Healthcare, Sweden), using 5 mm-thick contiguous axial sections, and reconstructed to 0.625 mm thick axial slices. All images were reviewed, the morphology and the maximum diameter of the common bile duct (CBD) were recorded. A dilated CBD was defined as a diameter more than 6 mm. The presence of any intrahepatic ductal dilatation was noted. Concomitant finding of hydronephrosis, if present, was also recorded.
Statistical analysis was performed using SPSS Version 20.0 for Mac (IBM Corporation, Armonk, NY, USA). Descriptive analysis was performed for the clinical data and the imaging findings. Correlation was performed by calculating Pearson correlation coefficient (Pearson’s r). Independent sample t test was used to compare the means between two groups. Wilcoxon Signed Rank test was used to compare the differences of CBD diameter before and after ketamine abstinence. Statistical significance was defined as p value <0.05.
Results
Demographics
Twenty-six patients (11 male, 15 female) were included in the study. Their age ranged from 21 to 41 years old (mean age 27.4 ± 4.1 years). The duration of ketamine abuse ranged from 2 to 16 years (mean 6.8 ± 3.3 years). Eleven patients were abstinent from ketamine use during the study period, and the remainders were active abusers. All patients were reported good past health with no other co-existing medical conditions. Twelve patients (46 %) were non-drinkers, 12 (46 %) were social drinkers, and 2 (8 %) were ex-drinkers. None of them were reported active alcohol abuse.
Clinical findings
Fourteen patients (54 %) had symptom of epigastric pain or right upper quadrant pain, while five were asymptomatic. For the remaining seven patients, this information could not be retrieved from the patient record. All, except two patients in whom serology was not tested, were negative for hepatitis B or C.
Liver function abnormality was evident in 21 patients (81 %), 19 being cholestatic (19/21, 90 %), and 2 being hepatocellular (2/21, 10 %). In the remaining five patients who did not fulfill the criteria for deranged liver function, only one patient had completely normal liver biochemistry. The other four patients had mildly elevated ALK level beyond the normal range, but not exceeding two times of the upper limits of normal. Nine patients had both abdominal pain and abnormal liver function tests.
Radiological findings
Six patients had both CT abdomen and MRCP performed, 12 had CT only, and 8 had MRCP only. The indications for imaging included abnormal liver function (16/26, 62 %), epigastric pain or right upper quadrant pain (6/26, 23 %), and others (including loin pain and trauma, 4/26, 15 %). In the “others” subgroup, two patients also had concurrent epigastric pain, while other two were asymptomatic but had abnormal liver function. In the 11 patients who achieved abstinence of ketamine, 5 had imaging studies before and after ketamine abstinence, while 6 had imaging studies only after abstinence. The summary is presented in Table 1.
In the 26 patients, 18 (69 %) had abnormal dilatation of the CBD. The CBD diameter ranged from 7 to 17 mm. The radiological findings were uniform in this group of patients. They all showed a fusiform dilatation of the CBD, with smooth distal tapering. There was no extrinsic lesion or intraductal filling defects to account for the dilated CBD. The intrahepatic ducts were not dilated (Fig. 1). No gallstones were evident in any of the patients. Concurrent ketamine cystitis was evident in 81 % of patients (21/26). Nine patients had co-existing hydronephrosis on the scans (Fig. 2). For patients who had both MRCP and CT studies, the imaging findings correlated well (Fig. 3).

MRCP of a patient demonstrating dilated common bile duct (CBD) to 8 mm. Note the smooth distal tapering of the CBD (white arrow). The intrahepatic ducts are not dilated. Gallbladder is denoted (*).

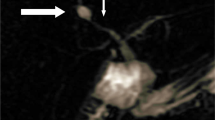
MRCP of another patient shows that the CBD is dilated with smooth distal tapering (white arrow). The intrahepatic ducts are not dilated. Concurrent finding of bilateral hydronephrosis is seen (⇑).

A MRCP and B contrast CT abdomen with multiplanar reformat of the same patient. Both demonstrate the presence of fusiform dilatation CBD with smooth distal tapering. The imaging findings correlate well with each other.
Five patients who achieved abstinence during the study period had follow-up imaging. All of them demonstrated an improvement in the degree of CBD dilatation (Table 1, Patients 1–5). Wilcoxon Signed Rank test showed a statistically significant difference between the CBD diameter before and after abstinence (p = 0.042). An example is shown in Fig. 4. For the six patients who only had imaging after abstinence, two had mildly dilated CBD to 8 mm, while others had normal CBD caliber.

Follow-up MRCP of a patient with A showing MRCP during active ketamine abuse, the liver function was ALK 3199 IU/L, ALT 406 IU/L, bilirubin 32 μmol/L. CBD measures 11 mm. Coexisting right hydronephrosis is shown. B MRCP 18 months after abstinence, the liver function was ALK 333 IU/L, ALT 46 IU/L, bilirubin 16 μmol/L. CBD measures 8 mm.
Correlating clinical and radiological findings
In the patients with abnormal liver function, 71 % (15/21) had dilated CBD; while in the patients with abdominal pain, 64 % (9/14) had dilated CBD. For patients with both abdominal pain and abnormal liver function, 67 % (6/9) had dilatation of CBD. In the remaining five patients who had abdominal pain as presenting symptoms, but liver function tests not reaching the definition of abnormal, three of them had CBD dilatation.
During the study period, 20 patients had imaging performed during active use of ketamine and 11 patients had scan performed during abstinence of ketamine. When comparing the mean CBD diameter between the two groups (active versus abstinence = 10.10 ± 3.68 versus 6.55 ± 2.88 mm, p = 0.006), there is a statistically significant difference.
The maximum CBD diameter shows a moderate correlation with the duration of ketamine use, adjusted for age and sex (adjusted Pearson’s r = 0.577, p = 0.008). The ALK level shows no significant correlation with the maximum CBD diameter (Pearson’s r = 0.055, p = 0.791).
ERCP findings
Three patients had ERCP performed for investigation of abnormal liver function. Their bilirubin levels were within normal range. The ERCP in all three patients showed dilatation of the CBD and distal narrowing. They were treated as having distal CBD stricture. Two patients (Patients 2 and 5 in Table 1) had insertion of biliary stent, while one patient had insertion of nasobiliary drain. The stents and drain were subsequently removed. Patients 2 and 5 achieved abstinence after ERCP and stent removal. Brush cytologies were negative for malignancy and follow-up imaging showed improvement in CBD dilatation for these two patients. The third patient remained an active user of ketamine, and the CBD dilatation was persistent on follow-up. The ERCP images of Patient 5 were retrospectively reviewed which showed dilatation of the CBD with distal tapering, similar to the imaging findings of MRCP and CT in other patients (Fig. 5). The ERCP images of the other two patients were irretrievable.

ERCP of a patient (Patient 5 in Table 1) shows fusiform dilatation of the CBD with distal tapering. A finding similar to the MRCP/CT features of other patients with dilated CBD.
Liver biopsy
Ten patients had non-lesional liver biopsy performed for investigation of abnormal liver function. Five had the biopsy during active ketamine use and five after abstinence. Active bile duct injury was observed in nine patients and evident by the presence of biliary epithelial disarray, lymphocytic cholangitis, and ductular reaction. There were no pathological features of large bile duct obstruction, primary biliary cirrhosis, primary sclerosing cholangitis, or fatty liver disease. One patient who had liver biopsy 14 months after abstinence, showed a normal liver biopsy. The MRCP, which was performed 12 months after abstinence, also showed a non-dilated CBD (6 mm).
Discussion
Ketamine is an N-methyl-d-aspartate receptor antagonist, a dissociative drug commonly used as a sedative and anesthetic agent in clinical practice [12]. Ketamine is increasingly used as a recreational drug due to its effects on the central nervous system, including vivid dreams, hallucination and floating sensation, and its short acting properties. It is a particularly popular recreational drug in Hong Kong adolescents, ranking the first in the age group under 21 [1]. This prevalence is also demonstrated by the young age in our series.
Ketamine is metabolized in liver and excreted by kidney [12]. The effect of ketamine on urinary bladder is well established. There is now emerging evidence that ketamine abuse is associated with liver injury and biliary dilatation in several case reports [5–9]. The common presentations of these patients included epigastric pain and deranged liver function. Therefore, we used epigastric pain and liver function abnormality as inclusion criteria in our study, acting as possible indicators of underlying ketamine-related cholangiopathy.
In Wong et al.’s [10] cohort of ketamine abusers, liver injury as evidenced by raised parameters in liver biochemistry panels, was found in 9.8 %. Elevated liver function enzymes are thought to be due to ketamine abuse in this cohort of patients as all of the patients were young without history of alcohol abuse, or other significant past medical history and were not carriers of hepatitis B or C. The exact mechanism for ketamine causing impaired liver function and biliary dilatation is still unknown. It has been postulated that the effect could be related to direct action on the biliary smooth muscles or central action [9], while some suggested concurrent parenchymal injury with bile ductular damage, and effect on smooth muscle of sphincter of Oddi leading to large bile duct dilatation [10].
Our study is so far the largest series reporting the radiological features of ketamine-related cholangiopathy. The common features of this group of patients include a fusiform dilatation of the CBD with smooth distal tapering, without intrahepatic ductal dilatation. In the study by Bachar et al. [13], the measurement of the extrahepatic bile duct in the age group 20–30 years old was found to be 1.2–4.9 mm, with a mean value of 2.7 mm. In our series, the CBD dilatation ranged from 7 to 17 mm. The appearance may mimic choledochal cyst as previously reported [5]. The other causes of dilated CBD, including extrinsic compression and intraductal lesion, were excluded by the MRCP and/or CT findings. Although three patients with ERCP were initially treated as having distal CBD stricture with sphincterotomy and stent placement, it was difficult to ascertain whether it was genuine CBD stricture. CBD dilatation with distal narrowing was an unanimous finding in all the study subjects. The bilirubin levels of these three patients were not elevated, and two showed improvement in CBD dilatation after abstinence, without the presence of CBD stents or prior dilatation. The biopsy results in nine patients confirmed the presence of bile duct injury and the absence of large duct obstruction. Sphincter of Oddi dysfunction leading to functional obstruction of the distal bile duct could have also been present. There was a study by Varadarajulu et al. [14] which demonstrated that 20 mg of ketamine administered intravenously had no effect on the sphincter of Oddi manometry. This study may not accurately reflect our clinical setting, as ketamine abusers had chronic and repeated exposure to ketamine, which is different from their study design. For future investigation, more invasive examinations such as sphincter of Oddi manometry may need to be performed on chronic ketamine abusers to ascertain the mechanism of CBD dilatation and the exact role of the sphincter of Oddi.
We demonstrated a moderate correlation of the CBD diameter with the duration of ketamine abuse. It is difficult to quantify the ketamine use by the abusers as ketamine is abused by inhalation, the purity and the exact dose cannot be precisely documented. This association suggests that the severity of biliary dilatation and ketamine consumption are related, however, further studies are needed to clarify the effect.
We found that the five patients who achieved abstinence showed an improvement in the degree of CBD dilatation, and most demonstrated improvement in the abnormal liver function. There is also a statistically significant difference between the CBD diameter of the active user group and the abstinence group. Although the exact clinical course for abstinent patients could not be established due to the limited study period, this suggests that ketamine-related cholangiopathy is reversible. The current study is also limited by the small sample size, its retrospective nature, and inconsistent timing of imaging during the course of ketamine abuse. Further studies would be needed to establish the prevalence of ketamine-related cholangiopathy, its natural history, the reversibility of this condition.
The prevalence of ketamine-related cholangiopathy is yet to be established. In Wong et al.’s [10] cohort of 297 subjects, liver injury occurred in 9.8 % of ketamine abusers, all of whom were symptomatic for urinary tract dysfunction. We found that concurrent ketamine cystitis was present in 81 % of our subjects. In a previous series reported by Chu et al. [3] on 10 ketamine abusers with bladder dysfunction, all of them demonstrated abnormal liver function tests. This suggests s that there may be a higher occurrence of ketamine-related cholangiopathy in abusers who have already developed cystitis. In Ng et al.’s [15] series of 223 ketamine abusers presenting to the emergency department, 21 % had abdominal pain as the major complaints, and liver function abnormalities were present in 16 % of patients. Further studies will be required to assess the prevalence of ketamine-related cholangiopathy in the abuse population. In summary, we presented the clinical and imaging findings of ketamine-related cholangiopathy. Characteristic features include fusiform dilatation of the CBD without obstructive lesion, and no dilatation of the intrahepatic biliary ducts. Possible indicators for underlying cholangiopathy include epigastric pain and impaired liver function. Severity of CBD dilatation appears to correlate with the duration of ketamine and there is also evidence that the condition may be reversible in abstinent patients. Radiologists and clinicians should be aware of the radiological manifestation of this condition to avoid misdiagnosis.
References
Central Registry of Drug Abuse Sixty-First Report (2002–2011) http://www.nd.gov.hk/en/crda_61st_report.htm. Accessed 13 March 2014
Substance Abuse and Mental Health Services Administration, Office of Applied Studies (2008) Use of Specific Hallucinogens. Rockville: Substance Abuse and Mental Health Services Administration, Office of Applied Studies
Chu PS, Kwok SC, Lam KM, et al. (2007) ‘Street ketamine’-associated bladder dysfunction: a report of ten cases. Hong Kong Med J = Xianggang yi xue za zhi/Hong Kong Acad Med 13(4):311–313
Chu PS, Ma WK, Wong SC, et al. (2008) The destruction of the lower urinary tract by ketamine abuse: a new syndrome? BJU Int 102(11):1616–1622. doi:10.1111/j.1464-410X.2008.07920.x
Wong SW, Lee KF, Wong J, et al. (2009) Dilated common bile ducts mimicking choledochal cysts in ketamine abusers. Hong Kong Med J = Xianggang yi xue za zhi/Hong Kong Acad Med 15(1):53–56
Seto WK, Ng M, Chan P, et al. (2011) Ketamine-induced cholangiopathy: a case report. Am J Gastroenterol 106(5):1004–1005. doi:10.1038/ajg.2010.485
Lui KL, Lee WK, Li MK (2014) Ketamine-induced cholangiopathy. Hong Kong Med J = Xianggang yi xue za zhi/Hong Kong Acad Med 20(1):78.e71–78.e72. doi:10.12809/hkmj133796
Gutkin E, Hussain SA, Kim SH (2012) Ketamine-induced biliary dilatation: from Hong Kong to New York. J Addict Med 6(1):89–91. doi:10.1097/ADM.0b013e3182399216
Lo RS, Krishnamoorthy R, Freeman JG, Austin AS (2011) Cholestasis and biliary dilatation associated with chronic ketamine abuse: a case series. Singap Med J 52(3):e52–e55
Wong GL, Tam YH, Ng CF, et al. (2014) Liver injury is common among chronic abusers of ketamine. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. doi:10.1016/j.cgh.2014.01.041
Danan G, Benichou C (1993) Causality assessment of adverse reactions to drugs—I. A novel method based on the conclusions of international consensus meetings: application to drug-induced liver injuries. J Clin Epidemiol 46(11):1323–1330
Haas DA, Harper DG (1992) Ketamine: a review of its pharmacologic properties and use in ambulatory anesthesia. Anesth Prog 39(3):61–68
Bachar GN, Cohen M, Belenky A, Atar E, Gideon S (2003) Effect of aging on the adult extrahepatic bile duct: a sonographic study. J Ultrasound Med Off J Am Inst Ultrasound Med 22(9):879–882; quiz 875–883
Varadarajulu S, Tamhane A, Wilcox CM (2008) Prospective evaluation of adjunctive ketamine on sphincter of Oddi motility in humans. J Gastroenterol Hepatol 23(8 Pt 2):e405–e409. doi:10.1111/j.1440-1746.2007.05024.x
Ng SH, Tse ML, Ng HW, Lau FL (2010) Emergency department presentation of ketamine abusers in Hong Kong: a review of 233 cases. Hong Kong Med J = Xianggang yi xue za zhi/Hong Kong Acad Med 16(1):6–11
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yu, WL., Cho, C.CM., Lung, P.FC. et al. Ketamine-related cholangiopathy: a retrospective study on clinical and imaging findings. Abdom Imaging 39, 1241–1246 (2014). https://doi.org/10.1007/s00261-014-0173-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-014-0173-2