
Abstract
Aim
Distant metastasis has a negative impact on survival in differentiated thyroid carcinoma (DTC). The timing of this manifestation, however, is of unknown prognostic relevance. The aim of this retrospective study was to investigate the potential significance of discriminating synchronous versus metachronous distant metastases (SDM vs. MDM) for the outcome of patients with DTC.
Methods
We retrospectively analyzed a consecutive cohort of n = 89 patients with distant metastases of DTC (43 with follicular, 46 with papillary DTC histology; mean age 52.6 ± 17.7 years) undergoing radioiodine treatment at our institution. All patients were treated with the same protocol consisting of ablative radioiodine therapy (RIT, 3.7 GBq) and one post-ablation treatment after 3 months (3.7–11.1 GBq). Further cycles of RIT were administered for recurrent, progressive or newly developed metastatic disease. We distinguished 2 types of distant metastases according to the time of manifestation: SDM (within ≤12 months after DTC diagnosis) and MDM (occurring >12 months after diagnosis). Tumor-related survival was analyzed using the Kaplan–Meier method. Uni- and multivariate analyses including the Cox proportional hazards model were performed with a significance level of p < 0.05.
Results
The mean follow-up period was 13.8 ± 1.2 years. SDM were present in 49 (55.1 %), MDM in 40 (44.9 %) patients. MDM were associated with shorter tumor-related survival (p = 0.002). 5-year and 10-year survival rates were 68.5 % and 34.8 % for MDM, and 84.3 % and 66.9 % for SDM, respectively. Within both age subgroups of <45 and ≥45 years, SDM were also linked with longer survival. No effect on tumor-related survival was found for the co-variables sex, lymph node metastases and histologic type.
Conclusion
Distinguishing synchronous from metachronous manifestation of distant metastases may add an important prognostic feature to risk stratification in DTC, as proven metachronous appearance is associated with impaired survival.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Differentiated thyroid cancer (DTC) accounts for more than 90 % of all thyroid cancers and is characterized by an indolent course of disease [1]. Standard treatment for DTC consists of total thyroidectomy followed by radioiodine (131I) ablation therapy (RIT) of remnant tissue [2–5]. The overall prognosis of DTC is excellent, with a 10-year disease-specific survival rate exceeding 85 % [6, 7]. Distant metastatic involvement along with advancing age, aggressive histological features, and inability to concentrate 131I are the main factors for impaired survival [8–11]. Synchronous distant metastases (SDM) are present at the time of initial thyroid cancer diagnosis in 1–3 % of patients and metachronous distant metastases (MDM) occur in 7–23 % patients particularly within the first years after the initial treatment [11]. The prognostic significance of the temporal onset of distant metastases in DTC is, to date, unclear. The purpose of this retrospective study was to investigate this issue, the prognostic difference of SDM versus MDM regarding the outcome of patients with DTC.
Material and methods
Eighty nine patients (32 males and 57 females, mean age 52.6 ± 17.7 years) with histologically confirmed DTC and distant metastasis receiving RIT according to the same protocol previously used in our institute between 1979 and 2009 were retrospectively analyzed [12, 13]. The cut-off date was chosen to allow a sufficient follow-up duration. To facilitate comparative analysis, only patients treated with the same empirical treatment protocol based on previous national guidelines [14–16] were included: All patients underwent surgical thyroidectomy, ablative RIT with an activity of 3.7 GBq (100 mCi) 4–5 weeks after thyroidectomy, and subsequent RIT 3 months after ablative therapy. No thyroid hormone replacement was initiated before ablative RIT with sufficient endogenous thyroid-stimulating hormone (TSH) stimulation (TSH >30 mU/l) required for treatment. Patients were instructed to avoid significant stable iodine exposure, and the semi-quantitative urine test prior to RIT excluded iodine excess (>150 μg/g creatinine) in all patients. A post-ablation whole body scan (WBS) was performed 5–7 days after the administration of 131I. Based on the results of WBS, post-ablative RIT was performed with 3.7–7.4 GBq if no distant metastases were present and with 11.1 GBq for patients with synchronous metastatic involvement.
After the completion of RIT, hormone replacement with Levothyroxine in doses achieving TSH suppression was started. Measurement of serum thyroglobulin levels after endogenous or exogenous TSH stimulation along with diagnostic radioiodine scanning was used for surveillance during the follow-up [3, 5]. Further cycles of RIT were administered for recurrent, progressive, or newly developed metastatic disease using the same activities as for post-ablative RIT. Patients with potentially interfering elevated Tg-specific auto-antibodies in the serum were not included in the study.
Patients were retrospectively divided into two groups based on the temporal onset of metastatic disease: SDM were defined as the metastases present at initial diagnosis or treatment of DTC (i.e. within 12 months from initial diagnosis) and MDM as appearance of metastases later than 12 months after initial diagnosis. Survival analysis was performed with the Kaplan–Meier method. Tumor-related survival (TRS) was assessed from the onset of distant metastases, and death from DTC was considered as an event. Survival outcomes were stratified by various variables and compared using the log-rank test with a significance level set at p < 0.05. Multivariate analysis using with the Cox proportional hazards model was performed for significant factors in univariate analysis. The software package SPSS 20 was used for statistical analysis.
Results
Forty six patients (51.7 %) had papillary and 43 patients (48.3 %) follicular histology of thyroid cancer. Lymph node involvement was observed in 51 patients (57.3 %). Metastatic sites were as follows: 40 pulmonary; 22 bone; 1 brain; 17 pulmonary and bone; 2 pulmonary and brain; 4 bone and brain; 2 pulmonary, bone and brain; 1 pulmonary, bone and liver. 49 patients (55.1 %) had SDM and 40 patients (44.9 %) developed MDM during the follow up. The mean time interval between initial diagnosis and onset of metastatic disease in patients with MDM was 5.7 ± 0.8 years. The SDM and MDM groups were well balanced regarding the variables of sex, age, lymph node involvement and histologic type of DTC (Table 1).
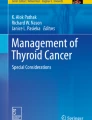
The mean follow-up period was 13.8 ± 1.2 years. 37 patients died during the follow-up, of which 30 were DTC-related deaths. The median tumor-related survival (TRS) from the diagnosis of metastatic disease was 11 years (95%CI, 5.4–16.6) for the entire cohort. On univariate analysis, patients with MDM had shorter survival from the onset of distant metastases (median TRS 8 years, 95%CI 5.7–10.2) compared to patients with SDM (median TRS not reached, p = 0.002). Five-year and 10-year survival rates were 84.3 ± 5.5 % and 66.9 ± 8.8 % for patients with SDM, and 68.5 ± 8.5 % and 34.8 ± 11.3 % for patients with MDM, respectively. Figure 1 shows the Kaplan–Meier curves of the patients stratified by SDM and MDM onset.

Tumor-related survival (TRS) stratified by the SDM versus MDM appearance of distant metastases. Survival was significantly worse in patients with MDM development of distant metastases (median TRS 8 years [95 % CI 5.7–10.2]) compared to those with SDM distant metastatic disease (median TRS not reached), p = 0.002
Advanced age at diagnosis of distant metastasis was the other significant risk factor of impaired survival in our analysis. Patients with age ≥45 years had shorter tumor-related survival (median TRS 8.7 years, 95 % CI 6.5–11) than patients of age <45 years (median TRS not reached, p = 0.002; Fig. 2). In both age subgroups, temporal onset of distant metastatic disease (synchronous vs. metachronous) was of prognostic relevance and MDM was associated with shorter TRS in both subgroups (Fig. 3). Lymph node involvement (p = 0.965), sex (p = 0.430), histologic type (p = 0.326), and the presence of pulmonary metastases (n = 62 with pulmonary, n = 27 with only extra-pulmonary distant metastases) had no impact on disease-related outcome in our cohort (p = 0.895, Table 2). On multivariate analysis, both patient age ≥45 y (HR 10.0; 95 % CI, 1.3–75.0; p = 0.024) and metachronous onset of distant metastases (HR 2.6; 95 % CI, 1.2–5.4; p = 0.014) remained as independent negative predictors for tumor-related survival. Table 2 summarizes the results of univariate and multivariate analyses regarding the endpoint of TRS.

Tumor related survival (TRS) stratified by age. Patients with ≥45 years of age at the time of diagnosis of metastatic disease had a significantly shorter survival (median TRS: 8.7 years [95 % CI: 6.5–11]) than patients <45 years (median TRS not reached), p = 0.002

Significant prognostic difference of SDM and MDM in a patients <45 years (10-year TRS: 100 % vs. 65.7 ± 27.3 %; p = 0.063) and b ≥45 years of age (10 year TRS: 52.4 ± 11.2 % vs. 26.7 ± 13.2; p = 0.022)
Discussion
This retrospective study on 89 patients with metastatic differentiated thyroid carcinoma undergoing “high-dose” RIT according to the same treatment protocol demonstrates the prognostic difference of synchronous and metachronous distant metastases. Presence of distant metastases (DM) is a well-established factor for poor prognosis in DTC [10, 17, 18] but there is few data regarding the prognostic relevance of its time of onset. In our study, patients with SDM had a better prognosis compared to patients developing MDM.
Few studies have reported higher 10-year disease-specific survival rates in patients with DM, but with no significant difference [19, 20]. In contrast to this, we observed a favorable TRS in patients presenting with initial distant metastatic DTC (median TRS not reached during the follow-up period of 13.8 ± 1.2 years) compared to patients who develop metachronous metastases during later follow-up (median TRS 8 years, 95 % CI 5.7–10.2; p = 0.002; Fig. 1). This finding is in accordance with a recent report suggesting metachronous bone metastases as a risk factor for impaired outcome in patients with DTC, employing only univariate analysis [21]. In our study, metachronous onset of distant metastases proved to be a negative independent predictor of outcome also on multivariate analysis (Table 2).
Advanced age is a predictive factor for recurrence and mortality in DTC and various staging systems have incorporated age with a cut-off of 45 y for risk stratification and management allocation of patients (UICC, AJCC, NTCTCS, ATA) [2, 22–25]. Applying the same cut-off, age was the only factor among the baseline patient characteristics that showed a significant contribution to survival in our cohort. Interestingly, MDM was associated with impaired survival in patients of both age groups. Therefore, time of metastatic manifestation may complement age for prognostic stratification of patients with distant metastatic DTC.
Not surprisingly, the presence of lymph node metastases was of no prognostic significance in our cohort with distant metastases. Similarly, other prognostic parameters in unselected DTC cohorts such as papillary vs. follicular histology type may have little influence in the presence of distant metastases, as in our cohort analysis [19, 26].
Limitations
There are obvious limitations of this study associated with the retrospective nature of the analysis. Firstly, the used treatment protocol covering 30 years of RIT inevitably differs from the current international guidelines advocating the administration of lower activities (i.e. 1–3.7 GBq) especially in the absence of metastatic disease [2, 27]. However, confining the cohort to patients treated with the same empirical protocol, albeit dated, excludes the treatment protocol as a contributing factor to different survival outcomes of the two groups (i.e. with SDM vs. MDM). The low number of events in the subgroup analysis of patients aged <45 years may weaken the strength of conclusions in this particular patient subset. Furthermore, the heterogeneity of metastatic sites in our cohort hampered the comparative analysis of the prognostic impact of each site. The preliminary finding of the prognostic impact of the onset of metastases has to be confirmed by larger analyses before applying it into clinical practice and decision-making.
Conclusions
Distinction between synchronous and metachronous manifestation of distant metastases may add an important prognostic feature to risk stratification of DTC. The metachronous onset seems to constitute an independent negative predictor for the diagnosis of distant metastases. This insight may impact future patient management if confirmed by larger studies.
References
Sherman SI. Thyroid carcinoma. Lancet. 2003;361:501–11.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133. doi:10.1089/thy.2015.0020.
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214. doi:10.1089/thy.2009.0110.
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006;16:109–42. doi:10.1089/thy.2006.16.ft-1.
Pacini F, Castagna MG, Brilli L, Pentheroudakis G. Differentiated thyroid cancer: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009;20 Suppl 4:143–6. doi:10.1093/annonc/mdp156.
Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. 1998;338:297–306. doi:10.1056/NEJM199801293380506.
Dean DS, Hay ID. Prognostic indicators in differentiated thyroid carcinoma. Cancer Control. 2000;7:229–39.
Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91:2892–9. doi:10.1210/jc.2005-2838.
Sampson E, Brierley JD, Le LW, Rotstein L, Tsang RW. Clinical management and outcome of papillary and follicular (differentiated) thyroid cancer presenting with distant metastasis at diagnosis. Cancer. 2007;110:1451–6. doi:10.1002/cncr.22956.
Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case–control study. Cancer. 2006;106:524–31. doi:10.1002/cncr.21653.
Haq M, Harmer C. Differentiated thyroid carcinoma with distant metastases at presentation: prognostic factors and outcome. Clin Endocrinol (Oxf). 2005;63:87–93. doi:10.1111/j.1365-2265.2005.02304.x.
Menzel C, Grunwald F, Schomburg A, Palmedo H, Bender H, Spath G, et al. “High-dose” radioiodine therapy in advanced differentiated thyroid carcinoma. J Nucl Med. 1996;37:1496–503.
Grunwald F, Ruhlmann J, Ammari B, Knopp R, Hotze A, Biersack HJ. Experience with a high-dose therapy concept in metastatic differentiated thyroid cancer. Nuklearmedizin. 1988;27:266–71.
Dietlein M, Dressler J, Eschner W, Grunwald F, Lassmann M, Leisner B, et al. Procedure guidelines for radioiodine therapy of differentiated thyroid cancer (version 3). Nuklearmedizin. 2007;46:213–9.
Dietlein M, Dressler J, Farahati J, Grunwald F, Leisner B, Moser E, et al. Procedure guidelines for radioiodine therapy of differentiated thyroid cancer (version 2). Nuklearmedizin. 2004;43:115–20. doi:10.1267/NUKL04040115.
Dietlein M, Dressler J, Farahati J, Leisner B, Moser E, Reiners C, et al. Guidelines for radioiodine therapy (RIT) in differentiated thyroid cancer. Nuklearmedizin. 1999;38:221–2.
Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery. 1993;114:1050–7. discussion 7–8.
Gilliland FD, Hunt WC, Morris DM, Key CR. Prognostic factors for thyroid carcinoma. A population-based study of 15,698 cases from the Surveillance, Epidemiology and End Results (SEER) program 1973–1991. Cancer. 1997;79:564–73. doi:10.1002/(SICI)1097-0142(19970201)79:3<564::AID-CNCR20>3.0.CO;2-0.
Shoup M, Stojadinovic A, Nissan A, Ghossein RA, Freedman S, Brennan MF, et al. Prognostic indicators of outcomes in patients with distant metastases from differentiated thyroid carcinoma. J Am Coll Surg. 2003;197:191–7. doi:10.1016/S1072-7515(03)00332-6.
Mihailovic JM, Stefanovic LJ, Malesevic MD, Erak MD, Tesanovic DD. Metastatic differentiated thyroid carcinoma: clinical management and outcome of disease in patients with initial and late distant metastases. Nucl Med Commun. 2009;30:558–64. doi:10.1097/MNM.0b013e32832cc2ab.
Orita Y, Sugitani I, Matsuura M, Ushijima M, Tsukahara K, Fujimoto Y, et al. Prognostic factors and the therapeutic strategy for patients with bone metastasis from differentiated thyroid carcinoma. Surgery. 2010;147:424–31. doi:10.1016/j.surg.2009.10.009.
Pitoia F, Bueno F, Urciuoli C, Abelleira E, Cross G, Tuttle RM. Outcomes of patients with differentiated thyroid cancer risk-stratified according to the American thyroid association and Latin American thyroid society risk of recurrence classification systems. Thyroid. 2013;23:1401–7. doi:10.1089/thy.2013.0011.
D’Avanzo A, Ituarte P, Treseler P, Kebebew E, Wu J, Wong M, et al. Prognostic scoring systems in patients with follicular thyroid cancer: a comparison of different staging systems in predicting the patient outcome. Thyroid. 2004;14:453–8. doi:10.1089/105072504323150778.
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17:1471–4. doi:10.1245/s10434-010-0985-4.
Mihailovic J, Stefanovic L, Malesevic M, Markoski B. The importance of age over radioiodine avidity as a prognostic factor in differentiated thyroid carcinoma with distant metastases. Thyroid. 2009;19:227–32. doi:10.1089/thy.2008.0186.
Lang BH, Wong KP, Cheung CY, Wan KY, Lo CY. Evaluating the prognostic factors associated with cancer-specific survival of differentiated thyroid carcinoma presenting with distant metastasis. Ann Surg Oncol. 2013;20:1329–35. doi:10.1245/s10434-012-2711-x.
Schlumberger M, Catargi B, Borget I, Deandreis D, Zerdoud S, Bridji B, et al. Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N Engl J Med. 2012;366:1663–73. doi:10.1056/NEJMoa1108586.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This article does not contain any studies with animals.
Informed consent
For this type of study, formal consent is not required.
Additional information
Amir Sabet and Ina Binse contributed equally to this work.
Rights and permissions
About this article

Cite this article
Sabet, A., Binse, I., Dogan, S. et al. Distinguishing synchronous from metachronous manifestation of distant metastases: a prognostic feature in differentiated thyroid carcinoma. Eur J Nucl Med Mol Imaging 44, 190–195 (2017). https://doi.org/10.1007/s00259-016-3485-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-016-3485-3