
Abstract
Purpose
The ε4 allele of the apolipoprotein E (APO-E4) gene, a genetic risk factor for Alzheimer’s disease (AD), also modulates brain metabolism and function in healthy subjects. The aim of the present study was to explore cerebral metabolism using FDG PET in healthy APO-E4 carriers by comparing cognitively normal APO-E4 carriers to noncarriers and to assess if patterns of metabolism are correlated with performance on cognitive tasks. Moreover, metabolic connectivity patterns were established in order to assess if the organization of neural networks is influenced by genetic factors.
Methods
Whole-brain PET statistical analysis was performed at voxel-level using SPM8 with a threshold of p < 0.005, corrected for volume, with age, gender and level of education as nuisance variables. Significant hypometabolism between APO-E4 carriers (n = 11) and noncarriers (n = 30) was first determined. Mean metabolic values with clinical/neuropsychological data were extracted at the individual level, and correlations were searched using Spearman’s rank test in the whole group. To evaluate metabolic connectivity from metabolic cluster(s) previously identified in the intergroup comparison, voxel-wise interregional correlation analysis (IRCA) was performed between groups of subjects.
Results
APO-E4 carriers had reduced metabolism within the left anterior medial temporal lobe (MTL), where neuropathological changes first appear in AD, including the entorhinal and perirhinal cortices. A correlation between metabolism in this area and performance on the DMS48 (delayed matching to sample-48 items) was found, in line with converging evidence involving the perirhinal cortex in object-based memory. Finally, a voxel-wise IRCA revealed stronger metabolic connectivity of the MTL cluster with neocortical frontoparietal regions in carriers than in noncarriers, suggesting compensatory metabolic networks.
Conclusion
Exploring cerebral metabolism using FDG PET can contribute to a better understanding of the influence of genetic factors on cerebral metabolism at both the local and network levels leading to phenotypical variations of the healthy brain and selective vulnerability.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The ε4 allele of the apolipoprotein E (APO-E4) gene is considered as a major genetic risk factor for Alzheimer’s disease (AD) [1, 2]. There is also increasing evidence from studies in healthy subjects with normal cognitive function that the APO-E4 has an impact on brain structure. An MRI study conducted in children and adolescents has shown cortical thinning of the left entorhinal cortex in APO-E4 carriers, suggesting that the alleles of the APO-E gene may modulate regional cortical thickness in the developing brain, but also raising the question as to whether reduced volumes of the entorhinal cortex in healthy individuals carrying the ε4 allele might contribute to the risk of AD [3]. Similarly, MRI studies in healthy adults who carry the ε4 allele have confirmed reduced volumes of the entorhinal cortex and the subiculum [4, 5].
Functional changes may be detected earlier than structural changes. In particular, changes in synaptic function probably precede degeneration and cell death, processes that ultimately result in tissue atrophy, as can be measured using structural MRI. In this regard, brain 18F-FDG PET can be used to measure changes in cerebral metabolic rate of glucose (CMRGlc) that is thought to reflect synaptic function [6]. Studies using FDG PET according to APO-E status in healthy adults have shown contradictory findings. While one study showed no evidence for hypometabolism [7], most have shown that healthy APO-E4 carriers display parietal, cingulate, and temporal hypometabolism [8–13], which is the metabolic pattern of hypometabolism in AD. More recently, hypometabolism restricted to the posterior cingulate, as classically found in prodromal AD, has been reported in healthy APO-E4 carriers aged 49 to 67 years [14].
Recently developed neuroimaging methods can also be used to explore neuronal networks in vivo. Changes in metabolic connectivity can be assessed by FDG PET using voxel-wise interregional correlation analysis (IRCA) [15]. Whether there are changes in interregional metabolic connectivity in healthy APO-E4 carriers, which could indicate processes that compensate for potential pathological changes in asymptomatic subjects, especially in younger subjects, remains unknown. It is also unclear how metabolic changes on FDG PET in APO-E4 carriers relate to cognitive function, in particular in younger healthy subjects. APO-E4 has been found to affect cognitive performance in elderly healthy APO-E4 carriers compared with noncarriers in some studies [16–19], but not in others [20]. Few studies have investigated the influence of APO-E4 on the relationship between data derived from brain imaging and cognition. Recently, a correlation between entorhinal white matter integrity and memory performance was found in healthy APO-E4 carriers using functional anisotropy on MRI [21], suggesting that APO-E4 carriers are more vulnerable to a relative disconnection within the medial temporal lobe (MTL) than noncarriers.
The aim of the present study was to explore cerebral metabolism further using FDG PET in healthy APO-E4 carriers by comparing cognitively normal APO-E4 carriers with noncarriers. We also assessed if patterns of metabolism are correlated with performance on cognitive tasks. Finally, metabolic connectivity patterns were established in order to study neural networks that could be implicated in both dysfunction and compensatory activities.
Materials and methods
Subjects
A total of 60 consecutive healthy subjects with strictly normal brain MRI, no cognitive complaints and no personal history of systemic disorders (especially treated diabetes or hypertension), or mental or neurological disorders, and without a family history of dementia were recruited by advertisement in the framework of a research programme. Subjects underwent an extensive neuropsychological assessment followed by FDG PET. APO-E genotype was also determined.
Neurocognitive assessment
General cognitive function was assessed using the Mini Mental State Examination (MMSE) [22] and the Mattis dementia rating scale (Mattis-DRS) [23]. Sustained attention was assessed using the Trail Making Test form A [24, 25]. Executive functions were evaluated using the Trail Making Test form B [24, 25], the Stroop test [25, 26], verbal fluency tasks [27], and the Frontal Assessment Battery [28]. Working memory was evaluated using the digit span-backwards and short term memory using the digit span forward subtest from the Wechsler Memory Scale (WMS-III) [29]. Anterograde memory was assessed using the French version of the Free and Cued Selective Reminding test (FCSRT) [30, 31], logical memory subtest of the WMS-III [29], delayed recall of the Rey-Osterrieth Complex Figure [32] and the DMS48, a visual recognition memory task [33]. Semantic memory concerning knowledge of famous events and people was evaluated using the Short-EVE test and TOP30 [34], respectively. Naming was assessed using the DO80 [35]. Visuoperceptive abilities were assessed using Benton’s facial recognition test [36] and visuospatial skills using the Copy condition of the Rey-Osterrieth Complex Figure test [32] and the Benton Judgement of Line Orientation test [37].
Memory was evaluated with the intensity scale of memory complaint (EIPM) [38], a ten-item scale developed in-house with a maximum score of 30 points. Normative data came from a population of 105 healthy subjects (mean EIPM score, m = 3.45 ± 3,0).
APO-E genotyping
Isotyping of amplified APO-E sequences was performed by Hha1 digestion and electrophoresis [39]. Eight units of Invitrogen Hha1 enzyme (cat no. 25212-010) were added to each 50 µl PCR mixture after amplification, without any specific restriction buffer added. The mixture was then heated for at least 3 h at 37 °C. After digestion, the samples were loaded onto an 8 % polyacrylamide gel contained between two 25 cm long glass plates 1.5 mm apart. Electrophoresis was run for 2 h under a constant current of 45 mA. The gel was then stained with ethidium bromide and the restriction fragments were visualized by UV transillumination. Their sizes were obtained by comparison with the GeneRuler 100 bp DNA ladder (Fermentas) loaded onto the gel.
PET study
CMRGlc was determined using FDG PET in all subjects under the same conditions. The PET scan was performed using an integrated PET/CT camera (Discovery ST, GE Healthcare, Waukesha, WI) with an axial resolution of 6.2 mm allowing 47 contiguous transverse sections of the brain of 3.27 mm thickness. FDG (150 MBq) was injected intravenously with the subject in an awake and resting state with eyes closed in a quiet environment. Image acquisition was started 30 min after injection and was ended 15 min later. Images were reconstructed using the ordered subsets expectation maximization algorithm with five iterations and 32 subsets, and corrected for attenuation using a CT transmission scan.
Data analysis
Clinical differences between subject groups were analysed using the chi-squared and Mann-Whitney tests. Whole-brain PET statistical analysis was performed at the voxel level using SPM8 software (Wellcome Department of Cognitive Neurology, University College, London, UK). The PET images were spatially normalized onto the Montreal Neurological Institute (MNI) atlas. The dimensions of the resulting voxels were 2 × 2 × 2 mm. The images were then smoothed with a Gaussian filter (8 mm full-width at half-maximum) to blur individual variations in gyral anatomy and to increase the signal-to-noise ratio. The “proportional scaling” routine was used to check for individual variations in global brain metabolism. Significant hypometabolism between APO-E4 carriers and noncarriers was determined using a threshold of p < 0.005, uncorrected, for the volume of the cluster (p < 0.05), with age, gender and level of education level as nuisance variables. Uncorrected thresholds were chosen at both the voxel level and cluster level (p < 0.005 and p < 0.05, respectively) to avoid type II errors, as previously recommended [40]. These analyses were nevertheless completed using small volume correction. This correction was based on a sphere with a volume equal to that of the anatomical region including the most significant voxel of the cluster [41]. The anatomical localization of the most significant voxels was then identified using Talairach Daemon (http://ric.uthscsa.edu/projects/talairachdaemon.html). The mean values of CMRGlc were extracted at the individual level, and correlation was searched with clinical/neuropsychological data using Spearman’s rank test in the whole group. Individual Z-scores were finally calculated from the extracted cluster by subtracting individual values from mean values of noncarriers and dividing by the standard deviation of this group.
To evaluate metabolic connectivity from metabolic cluster(s) previously identified in the intergroup comparison, IRCA was performed using SPM8 according to the procedure validated by Lee et al. [42]. Briefly, the mean extracted CMRGlc values were used as covariates to find regions showing significant voxel-wise interactions across subjects and between groups. This allowed a voxel-wise evaluation of the correlations between variables of interest and brain metabolism as assessed by PET comparing the two groups of subjects to determine stronger or weaker metabolic connectivity based on differences in the regression slopes. Contrasts were evaluated using inclusive mask within brain areas of positive correlations found in the group tested for presenting stronger metabolic connectivity (p < 0.005, uncorrected), in order to limit the analysis to existing significant correlations at the group level. SPM-T maps were displayed using a threshold of p < 0.005, uncorrected, for the volume of the cluster (p < 0.05), as described above, and secondarily completed by small volume correction.
Results
Of the 60 subjects investigated, 11 were APO-E4 carriers, all carrying one single APO-E4 allele. We secondarily selected a control group of 30 normal subjects who did not carry the APO-E4 allele, similar in age, gender and level of education. APO-E status was not disclosed to the participants.
Demographics and neuropsychological evaluation
The performance of all subjects on the neuropsychological assessment was within normal limits. APO-E4 carriers did not differ from noncarriers in terms of age, gender or level of education (Table 1), performance on the global cognitive assessment or any of the cognitive tasks (Table 2). The mean MMSE score was 29.45 for APO-E4 carriers and 29.57 for noncarriers. The mean age of the APO-E4 carriers was 48 years (range 20 – 73 years) and of the non-carriers was 47 years (range 25 – 74 years). According to the inclusion criteria, none of the APO-E4 carriers had a family history of dementia. Demographic data are summarized in Table 1 and neuropsychological features in Table 2.
PET findings
In comparison with noncarriers (p < 0.005, uncorrected), APO-E4 carriers showed significant hypometabolism within the left anterior MTL, including the entorhinal and the perirhinal cortices (T score = 5.20; k = 345; BA38, BA28, BA36; Fig. 1, Table 3). This cluster was statistically significant after small-volume correction (p = 0.017, corrected). At the individual level, in APO-E4 carriers, the Z-score of this cluster varied from −0.31 (in a 44-year-old subject) to −2.53 (in a 54-year-old subject). It is of note that a Z-score of −2.13 was found in a 25-year-old APO-E4 carrier.No significant hypometabolism was found with the opposite contrast.

PET imaging in an APO-E4 carrier shows significant hypometabolism in the left anterior medial temporal lobe, including the entorhinal and perirhinal cortices. In comparison to noncarriers, the voxel level significance was p < 0.005, uncorrected, and the cluster level significance was p < 0.05, small-volume corrected
The cluster of hypometabolism in the left anterior MTL was significantly correlated with performance on the DMS48 (rho = 0.34; p = 0.03) in the whole group of subjects. No significant correlations were found between this left temporal lobe cluster and other neuropsychological variables.
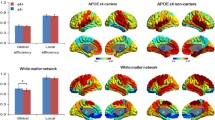
Metabolic connectivity was finally studied comparing carriers with noncarriers (p < 0.005, uncorrected). In APO-E4 carriers, the metabolic connectivity of the left anterior MTL cluster was stronger with the left middle and superior frontal gyri (BA8, BA9, BA10; correlation coefficient 0.77 in APO-E4 carriers, p = 0.005, vs. −0.30 in noncarriers, p = 0.11), with the left inferior parietal lobule (BA40; correlation coefficient 0.85 in APO-E4 carriers, p < 0.001), vs. −0.20 in non-carriers, p = 0.29), and with the medial frontal/cingulate cortex bilaterally (BA24, BA8, BA6; correlation coefficient 0.80 in APO-E4 carriers, p = 0.003, vs. 0.06 in noncarriers, p = 0.76; Table 3, Fig. 2). These clusters were statistically significant after small-volume correction (p = 0.010 to 0.023, corrected). No significant weaker connectivity for this cluster was found in APO-E4 carriers with the opposite contrast.

Stronger metabolic connectivity in APO-E4 carriers than in noncarriers (voxel level significance p < 0.005, uncorrected; cluster level significance p < 0.05, corrected for small volume). In APO-E4 carriers, metabolic connectivity of the left anterior MTL cluster was stronger with the left middle and superior frontal gyrus, with the left inferior parietal lobule, and with the bilateral medial frontal/cingulate cortex
Discussion
In this study, we compared cognitive performance and cerebral metabolism using FDG PET in healthy APO-E4 carriers and noncarriers, and tried to establish if there is a correlation between metabolism and performance on cognitive tasks. We also studied metabolic connectivity patterns to determine if APO-E4 affects the organization of neural networks. The main findings of this study are that healthy APO-E4 carriers had reduced PET metabolism within a region of the left anterior MTL when compared with noncarriers. This hypometabolism was not only found in older subjects, but also at an individual level in younger subjects. Moreover, this hypometabolism within the left MTL correlated with performance on the DMS48, a visual recognition memory task. Finally, a voxel-wise IRCA showed that the metabolic connectivity of this MTL cluster was stronger with neocortical frontoparietal regions in carriers than in noncarriers, in favour of a distinct organization of metabolic connectivity, and suggesting compensatory networks.
Mesiotemporal hypometabolism in healthy APO-E4 carriers
The APO-E4 carriers in this study were found to have reduced metabolism within a region of the left anterior MTL. This region, where cortical thinning has been reported in children and adolescents carrying the APO-E4 allele [3], is the site of neuropathological changes in the earliest stages of AD [43]. Thus, one interpretation could be that healthy APO-E4 carriers are at a presymptomatic stage of AD. An alternative hypothesis may be that individuals carrying the APO-E4 allele have increased vulnerability of the MTL which, in the event of a pathological insult related to AD, may lead to the expression of an amnestic phenotype of AD [44].
The topographic distribution of hypometabolism is, however, not in line with the findings of previous PET studies in healthy subjects, although significant MTL hypometabolism has been reported in patients with AD with more severe abnormalities in APO-E4 carriers than in noncarriers [45–47]. While one study found no changes on FDG PET in healthy adult APO-E4 carriers [7], several whole-brain studies have shown widespread hypometabolism in the parietal, cingulate and temporal regions, similar to the metabolic FDG PET profile of AD [8–12]. An “AD-signature” of hypometabolism in a large sample of APO-E4 carriers has also recently been reported in a study involving regions of interest (ROI) [13]. More recently, hypometabolism in the posterior cingulate, similar to that in prodromal AD, has also been reported using an a-priori hypothesis [14].
There are several explanations for the discrepancy between previous and the present findings. While only APO-E4 heterozygotes were included into the present study, both Reiman et al. [11] and Protas et al. [14] also included APO-E4 homozygotes, which might have influenced the results, especially since APO-E4 load is correlated with the pattern of hypometabolism in AD [11]. Besides methodological explanations (whole-brain vs. ROI a-priori analysis), these different findings may also be related to subject age, as it has been shown that APO-E genotype influences changes in brain function induced by ageing [48–50]. Except for one study [10], the subjects of the present report were nearly 10 years younger than those included into most previous studies (54 % of subjects were below the age of 40 years), while also including subjects over the age of 47 years. The only study in very young APO-E4 carriers with, unlike the present study, a narrow age range (20 – 39 years) showed hypometabolism in the parietal, cingulate and temporal regions, which might also have been related to a different whole-brain voxel-based methodology using 3D-SSP [10, 51], and not SPM. Finally, it is likely that the distinct findings in these FDG PET studies may have been a result of differences in the proportions of healthy subjects with preclinical AD among healthy APO-E4 carriers. Like many studies in the field, almost all APO-E4 carriers included in the study by Reiman et al. [10] had a family history of dementia and a very high level of education, which may have led to the inclusion of a high proportion of APO-E4 carriers with early-stage AD but normal cognition through compensatory mechanisms, while none of the subjects in the present study had a family history of dementia. For future FDG PET studies in APO-E4 carriers, it will therefore be crucial to assess markers of AD using CSF biomarkers or amyloid PET imaging to assess the likelihood of intracerebral amyloid or tau in APO-E4 carriers.
Another issue is the finding of hypometabolism in the left MTL only. Among the plausible explanations to account for this asymmetry is that it may be related to differences in synaptic organization between the left and the right hemisphere (e.g. in the hippocampus of mice [52]). A further possibility is that this asymmetry could reflect, at the preclinical stage, predominantly left hemisphere structural and metabolic changes previously reported in AD [53–55].
Relationship between metabolic changes and cognitive function
At the cognitive level, the positive correlation between the metabolism in the anterior MTL and performance on an object-based visual recognition memory task found in the present study is in line with evidence that the perirhinal cortex plays a crucial role in familiarity-based visual recognition memory [56, 57] and context-free memory [58]. The present findings therefore extend the results obtained in experimental animals [56] and in patients with focal brain lesions [33] concerning the relationship between the perirhinal cortex and visual recognition memory. At the network level, the present findings are also concordant with those of a resting-state fMRI study that suggested a functional relationship between object-based visual recognition memory and an anterior MTL network composed of the perirhinal and entorhinal cortices, the anterior hippocampus and the anterior temporal lobe [38, 59].
Using an extensive neuropsychological assessment, no difference in memory performance between carriers and noncarriers was found, a finding that has been reported previously in younger individuals [10, 20, 48, 50], while studies in older subjects have identified APO-E4 as a factor accounting for cognitive decline in normal ageing [60–62], with the largest effect in late life [63, 64]. However, because of the functional relationship between metabolism and performance on an object-based visual recognition memory task, it remains to be established if a more challenging task assessing object-based visual recognition memory would be likely to differentiate healthy APO-E4 carriers from noncarriers.
Early AD in healthy APO-E4 carriers?
In the most frequent form of AD, the MTL is where neurofibrillary tangles (NFT), related to Tau protein pathology and associated with clinical deficits [66, 67], initially develop. These neuropathological changes first appear in the subhippocampal region, the medial portion of the perirhinal cortex – the transentorhinal cortex (TERC, or BA35) – and then progress to the entorhinal cortex [43]. NFTs within the MLT have recently been described in young individuals, even those under the age of 30 years [68]. In AD, lesions are thought to appear years before the development of overt cognitive changes that can be revealed using standardized cognitive tasks, and it is currently unknown whether this pathological change is associated with more subtle cognitive dysfunction. The present findings of perirhinal hypometabolism in APO-E4 carriers, correlated with performance on a memory task assessing context-free memory, also raise the question as to whether these subjects are at a preclinical stage of AD. However, more challenging neuropsychological tasks are more likely to reveal deficits and should ideally assess the function of the perirhinal cortex, such as familiarity-based recognition memory tasks that are thought to contribute to the preclinical diagnosis of AD [69, 70] and tasks assessing visual short-term memory binding that is altered in asymptomatic mutation carriers in familial AD [71].
Organization of metabolic connectivity in APO-E4 carriers
We here specifically studied the connectivity of an anterior MTL region which was hypometabolic in APO-E4 carriers. The functional connectivity of this region was first explored in healthy subjects by Kahn et al. [72] who identified two neuroanatomically dissociable, large-scale cortical memory networks, referred to as the anterior and posterior MTL networks using resting-state fMRI. Changes in connectivity of the MTL were recently reported in subjects at risk of AD, such as those with subjective memory impairment and mild cognitive impairment [59, 73]. In the present study, the metabolic connectivity of the left anterior MTL cluster in APO-E4 carriers was stronger with the left middle and superior frontal gyri, with the left inferior parietal lobule, and with the bilateral medial frontal/cingulate cortex. Correlation coefficients revealed that correlations between these regions were only significant in APO-E4 carriers, favouring distinct organization of metabolic connectivities in APO-E4 carriers and noncarriers. MTL connectivity differences could thus be interpreted as reduced MTL function in the left hemisphere being compensated for through recruitment of additional regions belonging to a frontoparietal network, as previously demonstrated using memory paradigms with functional MRI in healthy APO-E4 carriers [74–77]. These results are also in line with those of studies showing increased prefrontal activation in memory-related functional MRI studies in subjects with MCI [78] and patients with mild AD [79]. Finally, evidence for compensatory neural networks involving the right dorsolateral prefrontal cortex in highly educated patients with prodromal AD, thought to be related to cognitive reserve, has also been found in a study using FDG PET [15].
Limitations
The main limitation of the present study was the small number of APO-E4 carriers. The present findings need to be replicated in a larger population of APO-E4 carriers, if possible combined with markers of AD using CSF biomarkers or amyloid PET imaging. Also, particular features of this study population, for example their relatively young age, their wide age range and the fact that they included only heterozygote APO-E4 carriers, may have affected the findings. Finally, no physical correction was performed for the partial volume effect and we therefore cannot exclude the possibility that the findings reflect the combined effects of atrophy and hypometabolism, and not exclusively hypometabolism.
Conclusion
This PET study showed reduced metabolism in healthy APO-E4 carriers in a region of the left anterior MTL when compared with APO-E4 noncarriers, and at the individual level especially in younger subjects. Moreover, this hypometabolism correlated with performance on the DMS48, a visual recognition memory task, corroborating the findings of previous studies in experimental animals and in patients with focal brain lesions, and suggesting that future studies in healthy APO-E4 carriers should use more sensitive cognitive tasks to assess the function of the perirhinal region. Finally, a voxel-wise IRCA showed that the hypometabolic MTL cluster was more correlated with neocortical frontoparietal regions in carriers than in noncarriers, in favour of distinct organization of metabolic connectivity, and suggesting compensatory networks.
References
Strittmatter WJ, Roses AD. Apolipoprotein E and Alzheimer disease. Proc Natl Acad Sci U S A. 1995;92(11):4725–7.
Corder EH, Saunders AM, Strittmatter WJ, Schmechel DE, Gaskell PC, Small GW, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer's disease in late onset families. Science. 1993;261:921–3.
Shaw P, Lerch JP, Pruessner JC, Taylor KN, Rose AB, Greenstein D, et al. Cortical morphology in children and adolescents with different apolipoprotein E gene polymorphisms: an observational study. Lancet Neurol. 2007;6(6):494–500.
Burggren AC, Zeineh MM, Ekstrom AD, Braskie MN, Thompson PM, Small GW, et al. Reduced cortical thickness in hippocampal subregions among cognitively normal apolipoprotein E e4 carriers. Neuroimage. 2008;41(4):1177–83.
Donix M, Burggren AC, Suthana NA, Siddarth P, Ekstrom AD, Krupa AK, et al. Longitudinal changes in medial temporal cortical thickness in normal subjects with the APOE-4 polymorphism. Neuroimage. 2010;53(1):37–43.
Magistretti PJ, Pellerin L. Cellular mechanisms of brain energy metabolism and their relevance to functional brain imaging. Philos Trans R Soc Lond B Biol Sci. 1999;354:1155–63.
Samuraki M, Matsunari I, Chen WP, Shima K, Yanase D, Takeda N, et al. Glucose metabolism and gray-matter concentration in apolipoprotein E ε4 positive normal subjects. Neurobiol Aging. 2012;33(10):2321–3.
Reiman EM, Caselli RJ, Yun LS, Chen K, Bandy D, Minoshima S, et al. Preclinical evidence of Alzheimer's disease in persons homozygous for the epsilon 4 allele for apolipoprotein E. N Engl J Med. 1996;334(12):752–8.
Reiman EM, Caselli RJ, Chen K, Alexander GE, Bandy D, Frost J. Declining brain activity in cognitively normal apolipoprotein E epsilon 4 heterozygotes: a foundation for using positron emission tomography to efficiently test treatments to prevent Alzheimer's disease. Proc Natl Acad Sci U S A. 2001;98(6):3334–9.
Reiman EM, Chen K, Alexander GE, Caselli RJ, Bandy D, Osborne D, et al. Functional brain abnormalities in young adults at genetic risk for late-onset Alzheimer's dementia. Proc Natl Acad Sci U S A. 2004;101(1):284–9.
Reiman EM, Chen K, Alexander GE, Caselli RJ, Bandy D, Osborne D, et al. Correlations between apolipoprotein E epsilon4 gene dose and brain-imaging measurements of regional hypometabolism. Proc Natl Acad Sci U S A. 2005;102:8299–302.
Langbaum JB, Chen K, Caselli RJ, Lee W, Reschke C, Bandy D, et al. Hypometabolism in Alzheimer-affected brain regions in cognitively healthy Latino individuals carrying the apolipoprotein E epsilon4 allele. Arch Neurol. 2010;67(4):462–8.
Knopman DS, Jack Jr CR, Wiste HJ, Lundt ES, Weigand SD, Vemuri P, et al. 18F-fluorodeoxyglucose positron emission tomography, aging, and apolipoprotein E genotype in cognitively normal persons. Neurobiol Aging. 2014;35(9):2096–106.
Protas HD, Chen K, Langbaum JB, Fleisher AS, Alexander GE, Lee W, et al. Posterior cingulate glucose metabolism, hippocampal glucose metabolism, and hippocampal volume in cognitively normal, late-middle-aged persons at 3 levels of genetic risk for Alzheimer disease. JAMA Neurol. 2013;70(3):320–5.
Morbelli S, Perneczky R, Drzezga A, Frisoni GB, Caroli A, van Berckel B, et al. Metabolic networks underlying cognitive reserve in prodromal Alzheimer disease: a European Alzheimer disease consortium project. J Nucl Med. 2013;54(6):894–902.
Wilson RS, Bienias JL, Berry-Kravis E, Evans DA, Bennett DA. The apolipoprotein E epsilon 2 allele and decline in episodic memory. J Neurol Neurosurg Psychiatry. 2002;73:672–7.
Caselli RJ, Reiman EM, Osborne D, Hentz JG, Baxter LC, Hernandez JL, et al. Longitudinal changes in cognition and behavior in asymptomatic carriers of the APOE e4 allele. Neurology. 2004;62:1990–95.
Caselli RJ, Reiman EM, Locke DE, Hutton ML, Hentz JG, Hoffman-Snyder C, et al. Cognitive domain decline in healthy apolipoprotein E epsilon4 homozygotes before the diagnosis of mild cognitive impairment. Arch Neurol. 2007;64:1306–11.
Nilsson LG, Adolfcson R, Backman L, Cruts M, Nyberg L, Small BJ, et al. The influence of APOE status on episodic and semantic memory: data from a population-based study. Neuropsychology. 2006;20:645–57.
Ihle A, Bunce D, Kliegel M. APOE epsilon4 and cognitive function in early life: a meta-analysis. Neuropsychology. 2012;26:267–77.
Westlye ET, Hodneland E, Haász J, Espeseth T, Lundervold A, Lundervold AJ. Episodic memory of APOE ε4 carriers is correlated with fractional anisotropy, but not cortical thickness, in the medial temporal lobe. Neuroimage. 2012;63(1):507–16.
Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;2(3):189–98.
Mattis S. Mental status examination for organic mental syndrome in the elderly patients. In: Bellak L, Karasu T, editors. Geriatrics psychiatry: a handbook for psychiatrists and primary care physicians. New York: Grune & Stratton; 1976. p. 77–121.
Reitan RM. Validity of the Trail Making test as an indicator of organic brain damage. Percept Mot Skills. 1958;8:271–6.
Allain P, Nicoleau S, Pinon K, Etcharry-Bouyx F, Barré J, Berrut G, et al. Executive functioning in normal aging: a study of action planning using the Zoo Map Test. Brain Cogn. 2005;57(1):4–7.
Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. 1935;18(6):643–62.
Cardebat D, Doyon B, Puel M, Goulet P, Joanette Y. Formal and semantic lexical evocation in normal subjects. Performance and dynamics of production as a function of sex, age and educational level. Acta Neurol Belg. 1990;90:207–17.
Dubois B, Slachevsky A, Litvan I, Pillon B. The FAB: a frontal assessment battery at bedside. Neurology. 2000;55:1621–26.
Wechsler D. Echelle clinique de mémoire de Wechsler MEM-III (WMS-III). Paris: Les éditions du Centre de Psychologie appliquée; 2001.
Grober E, Buschke H, Crystal H, Bang S, Dresner R. Screening for dementia by memory testing. Neurology. 1988;38(6):900–3.
Ergis A-M, Van der Linden M, Deweer B. Investigation of memory performance with a cued recall test in Alzheimer's disease. Rev Neuropsychol. 1994;4:47–68.
Rey A. L’examen psychologique dans les cas d’encéphalopathie traumatique. Arch Psychol. 1941;28:286–340.
Barbeau E, Didic M, Tramoni E, Felician O, Sontheimer A, Joubert S, et al. Evaluation of visual recognition memory in MCI patients. Neurology. 2004;62:1317–22.
Thomas-Antérion C. La mémoire collective, mémoire des événements publics et des célébrités. Les batteries EVE 30 et TOP 30. Marseille: Solal; 2006.
Deloche G, Hannequin D. Test de dénomination orale d'images DO80. Paris: Les Editions du Centre de Psychologie appliquée; 1997.
Benton AL, Sirvan AB, Hamsher D, Varney NR, Spreen O. Facial recognition: stimulus and multiple choice pictures. Contributions to neuropsychological assessment. New York: Oxford University Press; 1983.
Benton AL, Hamsher K, Varney NR, Spreen O. Benton's Judgement of Line Orientation Test. Contributions to neuropsychological assessment. New York: Oxford University Press; 1983.
Gour N, Ranjeva JP, Ceccaldi M, Confort-Gouny S, Barbeau E, Soulier E, et al. Basal functional connectivity within the anterior temporal network is associated with performance on declarative memory tasks. Neuroimage. 2011;58(2):687–97.
Hixson JE, Vernier DT. Restriction isotyping of human apolipoprotein E by gene amplification and cleavage with Hha1. J Lipid Res. 1990;31(3):545–8.
Lieberman MD, Cunningham WA. Type I and Type II error concerns in fMRI research: re-balancing the scale. Soc Cogn Affect Neurosci. 2009;4(4):423–8.
Worsley KJ, Marrett S, Neelin P, Vandal AC, Friston KJ, Evans AC. A unified statistical approach for determining significant signals in images of cerebral activation. Hum Brain Mapp. 1996;4:58–73.
Lee DS, Kang H, Kim H, Park H, Oh JS, Lee JS, et al. Metabolic connectivity by interregional correlation analysis using statistical parametric mapping (SPM) and FDG brain PET; methodological development and patterns of metabolic connectivity in adults. Eur J Nucl Med Mol Imaging. 2008;35(9):1681–91.
Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 1991;82(4):239–59.
van der Flier WM, Schoonenboom SNM, Pijnenburg YAL, Fox NC, Scheltens P. The effect of APOE genotype on clinical phenotype in Alzheimer disease. Neurology. 2006;67:526–7.
Lee KU, Lee JS, Kim KW, Jhoo JH, Lee DY, Yoon JC, et al. Influence of the apolipoprotein E type 4 allele on cerebral glucose metabolism in Alzheimer's disease patients. J Neuropsychiatry Clin Neurosci. 2003;15(1):78–83.
Mosconi L, Nacmias B, Sorbi S, De Cristofaro J, Fayazz M, Tedde A, et al. Brain metabolic decreases related to the dose of the ApoE e4 allele in Alzheimer's disease. J Neurol Neurosurg Psychiatry. 2004;75(3):370–6.
Mosconi L, Herholz K, Prohovnik I, Nacmias B, De Cristofaro MTR, Fayyaz M, et al. Metabolic interaction between ApoE genotype and onset age in Alzheimer's disease: implications for brain reserve. J Neurol Neurosurg Psychiatry. 2005;76(1):15–23.
Wisdom NM, Callahan JL, Hawkins KA. The effects of apolipoprotein E on non-impaired cognitive functioning: a meta-analysis. Neurobiol Aging. 2011;32:63–74.
Alexander DM, Williams LM, Gatt JM, Dobson-Stone C, Kuan SA, Todd EG, et al. The contribution of apolipoprotein E alleles on cognitive performance and dynamic neural activity over six decades. Biol Psychol. 2007;75:229–38.
Small BJ, Rosnick CB, Fratiglioni L, Bäckman L. Apolipoprotein E and cognitive performance: a meta-analysis. Psychol Aging. 2004;19:592–600.
Minoshima S, Frey KA, Koeppe RA, Foster NL, Kuhl DE. A diagnostic approach in Alzheimer's disease using three-dimensional stereotactic surface projections of fluorine-18-FDG PET. J Nucl Med. 1995;36(7):1238–48.
Shinohara Y, Hirase H, Watanabe M, Itakura M, Takahashi M, Shigemoto R. Left-right asymmetry of the hippocampal synapses with differential subunit allocation of glutamate receptors. Proc Natl Acad Sci U S A. 2008;105(49):19498–503.
Loewenstein DA, Barker WW, Chang JY, Apicella A, Yoshii F, Kothari P, et al. Predominant left hemisphere metabolic dysfunction in dementia. Arch Neurol. 1989;46:146–52.
Johnson KA, Jones K, Holman BL, Becker JA, Spiers PA, Satlin A, et al. Preclinical prediction of Alzheimer’s disease using SPECT. Neurology. 1998;50:1563–71.
Thompson PM, Hayashi KM, de Zubicaray G, Janke AL, Rose SE, Semple J, et al. Dynamics of gray matter loss in Alzheimer's disease. J Neurosci. 2003;23(3):994–1005.
Meunier M, Bachevalier J, Mishkin M, Murray EA. Effects on visual recognition of combined and separate ablations of the entorhinal and perirhinal cortex in rhesus monkeys. J Neurosci. 1993;13:5418–32.
Aggleton JP, Vann SD, Denby C, Dix S, Mayes AR, Roberts N, et al. Sparing of the familiarity component of recognition memory in a patient with hippocampal pathology. Neuropsychologia. 2005;43(12):1810–23.
Mishkin M, Suzuki WA, Gadian DG, Vargha-Khadem F. Hierarchical organization of cognitive memory. Philos Trans R Soc Lond B Biol Sci. 1997;352(1360):1461–7.
Caselli RJ, Graff-Radford NR, Reiman EM, Weaver A, Osborne D, Lucas J, et al. Preclinical memory decline in cognitively normal apolipoprotein E-epsilon4 homozygotes. Neurology. 1999;53:201–7.
Gour N, Felician O, Didic M, Koric L, Gueriot C, Chanoine V, et al. Functional connectivity changes differ in early and late-onset Alzheimer's disease. Hum Brain Mapp. 2014;35(7):2978–94.
Deary IJ, Whiteman MC, Pattie A, Starr JM, Hayward C, Wright AF, et al. Cognitive change and the APOE epsilon 4 allele. Nature. 2002;418(6901):932.
Wilson RS, Schneider JA, Barnes LL, Beckett LA, Aggarwal NT, Cochran EJ, et al. The apolipoprotein E epsilon 4 allele and decline in different cognitive systems during a 6-year period. Arch Neurol. 2002;59:1154–60.
Caselli RJ. Age-related memory decline and apolipoprotein E e4. Discov Med. 2009;8(41):47–50.
Schiepers OJ, Harris SE, Gow AJ, Pattie A, Brett CE, Starr JM, et al. APOE E4 status predicts age-related cognitive decline in the ninth decade: longitudinal follow-up of the Lothian Birth Cohort 1921. Mol Psychiatry. 2012;17(3):315–24.
Arriagada PV, Growdon JH, Hedley-Whyte ET, Hyman BT. Neurofibrillary tangles but not senile plaques parallel duration and severity of Alzheimer's disease. Neurology. 1992;42:631–9.
Gomez-Isla T, Hollister R, West H, Mui S, Growdon JH, Petersen RC, et al. Neuronal loss correlates with but exceeds neurofibrillary tangles in AD. Ann Neurol. 1997;41(6):809–13.
Braak H, Del Tredici K. The pathological process underlying Alzheimer's disease in individuals under thirty. Acta Neuropathol. 2011;121(2):171–81.
Didic M, Barbeau EJ, Felician O, Tramoni E, Guedj E, Poncet M, et al. Which memory system is impaired first in Alzheimer's disease? J Alzheimers Dis. 2011;27(1):11–22.
Wolk DA, Manning K, Kliot D, Arnold SE. Recognition memory in amnestic-mild cognitive impairment: insights from event-related potentials. Front Aging Neurosci. 2013;5:89. doi:10.3389/fnagi.2013.00089.
Parra MA, Abrahams S, Logie RH, Mendez LG, Lopera F, Della SS. Visual short-term memory binding deficits in familial Alzheimer’s disease. Brain. 2010;133:2702–13.
Kahn I, Andrews-Hanna JR, Vincent JL, Snyder AZ, Buckner RL. Distinct cortical anatomy linked to subregions of the medial temporal lobe revealed by intrinsic functional connectivity. J Neurophysiol. 2008;100:129–39.
Das SR, Pluta J, Mancuso L, Kliot D, Orozco S, Dickerson BC, et al. Increased functional connectivity within medial temporal lobe in mild cognitive impairment. Hippocampus. 2012;23:1–6.
Bookheimer SY, Strojwas MH, Cohen MS, Saunders AM, Pericak-Vance MA, Mazziotta JC, et al. Patterns of brain activation in people at risk for Alzheimer’s disease. N Engl J Med. 2000;343:450–56.
Fleisher AS, Houston WS, Eyler LT, Frye S, Jenkins C, et al. Identification of Alzheimer disease risk by functional magnetic resonance imaging. Arch Neurol. 2005;62:1881–88.
Bondi MW, Houston WS, Eyler LT, Brown GG. fMRI evidence of compensatory mechanisms in older adults at genetic risk for Alzheimer disease. Neurology. 2005;64:501–8.
Han SD, Houston WS, Eyler LT, Salmon DP, Fleisher AS, Bondi MW. Verbal paired-associate learning by APOE genotype in nondemented older adults: fMRI evidence of a right hemispheric compensatory response. Neurobiol Aging. 2006;28:238–47.
Heun R, Freymann K, Erb M, Leube DT, Jessen F, Kircher TT, et al. Mild cognitive impairment (MCI) and actual retrieval performance affect cerebral activation in the elderly. Neurobiol Aging. 2007;28:404–13.
Garrido GE, Furuie SS, Buchpiguel CA, Bottino CM, Almeida OP, Cid CG, et al. Relation between medial temporal atrophy and functional brain activity during memory processing in Alzheimer’s disease: a combined MRI and SPECT study. J Neurol Neurosurg Psychiatry. 2002;73:508–16.
Compliance with ethical standards
None.
Conflicts of interest
None.
Funding
This study was funded by AP-HM (PHRC 2007/09) and supported by INSERM (Centre d’Investigation Clinique, CIC, Hôpital de la Conception, Marseille), as well as the association “Déchaîne ton cœur”. M. Didic received a Marie Curie grant from the European Commission (BMH4CT965032).
Research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. A committee on human experimentation of the institution and the local institutional committee approved this study (registration number NCT00484523).
Informed consent
Informed consent was obtained from all participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Didic, M., Felician, O., Gour, N. et al. Rhinal hypometabolism on FDG PET in healthy APO-E4 carriers: impact on memory function and metabolic networks. Eur J Nucl Med Mol Imaging 42, 1512–1521 (2015). https://doi.org/10.1007/s00259-015-3057-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-015-3057-y