
Abstract
Purpose
Apart from binding to the dopamine transporter (DAT), [123I]FP-CIT shows moderate affinity for the serotonin transporter (SERT), allowing imaging of both monoamine transporters in a single imaging session in different brain areas. The aim of this study was to systematically evaluate extrastriatal binding (predominantly due to SERT) and its age and gender dependencies in a large cohort of healthy controls.
Methods
SPECT data from 103 healthy controls with well-defined criteria of normality acquired at 13 different imaging centres were analysed for extrastriatal binding using volumes of interest analysis for the thalamus and the pons. Data were examined for gender and age effects as well as for potential influence of striatal DAT radiotracer binding.
Results
Thalamic binding was significantly higher than pons binding. Partial correlations showed an influence of putaminal DAT binding on measured binding in the thalamus but not on the pons. Data showed high interindividual variation in extrastriatal binding. Significant gender effects with 31 % higher binding in women than in men were observed in the thalamus, but not in the pons. An age dependency with a decline per decade (±standard error) of 8.2 ± 1.3 % for the thalamus and 6.8 ± 2.9 % for the pons was shown.
Conclusion
The potential to evaluate extrastriatal predominant SERT binding in addition to the striatal DAT in a single imaging session was shown using a large database of [123I]FP-CIT scans in healthy controls. For both the thalamus and the pons, an age-related decline in radiotracer binding was observed. Gender effects were demonstrated for binding in the thalamus only. As a potential clinical application, the data could be used as a reference to estimate SERT occupancy in addition to nigrostriatal integrity when using [123I]FP-CIT for DAT imaging in patients treated with selective serotonin reuptake inhibitors.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Imaging of the dopaminergic system provides a valuable tool for discriminating neurodegenerative Parkinsonian syndromes with an associated presynaptic dopaminergic deficit from diseases without presynaptic neurodegeneration (e.g. essential tremor) [1–3]. The use of dopamine transporter (DAT) SPECT has recently been extended to the discrimination between patients with suspected dementia with Lewy bodies (DLB) and those with Alzheimer’s disease [4].
[123I]N-ω-Fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane ([123I]FP-CIT) is the most widely used radiotracer for DAT imaging. It is commercially available and approved for use in patients with Parkinsonian syndromes (Europe and the US) and suspected DLB (Europe). [123I]FP-CIT shows high affinity for DAT but also moderate affinity for the serotonin transporter (SERT) [5]. Binding of radiolabelled tropane derivatives in most extrastriatal regions (ESTR) has been primarily attributed to SERT binding. The thalamus has about 20 times more SERT than DAT binding sites [6–8]. In an autoradiography study of the human brain [9], the selective serotonin reuptake inhibitor (SSRI) citalopram almost entirely displaced [125I]RTI-55 ([125I]2β-carbomethoxy-3β-(4-iodophenyl)tropane, [125I]β-CIT) in the midbrain, thalamus and hypothalamus, indicating that radiotracer uptake in these regions is almost exclusively associated with SERT and not with DAT. With a preference for DAT sites (3.5 nM) over SERT sites (10 nM) [5], approximately 70 % of [123I]FP-CIT uptake in the thalamus should result from SERT binding. Consistently, applied to SPECT imaging, Ziebell et al. [10] observed a loss of thalamic binding potential of the nondisplaceable radioligand by 63 % when blocking SERT with citalopram. For semiquantitative evaluation using a ratio method in transient equilibrium (as generally applied in clinical routine), even 86 – 90 % of thalamus signal could be attributed to SERT binding [10, 11]. The first successful attempts to establish [123I]FP-CIT for SERT imaging studied the central serotonergic system in 6 [12] and 19 [13] healthy volunteers. Initial applications in patients indicated potential clinical usefulness showing reduced extrastriatal SERT availability in patients with Parkinson’s disease and particularly in those with DLB [14, 15].
In comparison to other cocaine analogues suitable for SPECT imaging, [123I]FP-CIT allows the combined evaluation of both DAT and SERT in a single scan. The ideal time window for imaging the extrastriatal SERT is between 2 and 3 h after injection [13]. For DAT imaging with [123I]FP-CIT, the pseudoequilibrium is reached 3 h after injection [16], resulting in ideal imaging conditions for both monoamine transporters 3 h after injection. This, in addition to its widespread availability, makes [123I]FP-CIT attractive for imaging not only the striatal DAT but also the extrastriatal SERT in the diagnostic work-up of patients. As a potential clinical application, SERT occupancy could be estimated in patients treated with SSRIs undergoing DAT SPECT to measure nigrostriatal integrity. Depression is a common nonmotor symptom in Parkinson’s disease and its treatment is challenging [17]. Higher pretreatment SERT availability, higher SSRI-induced occupancy of SERT [18] and SERT interplay between the median raphe nucleus and projection areas [19] have been associated with treatment response. Knowledge of SERT availability could allow individualization of treatment strategies (for example by optimized selection of the most suitable antidepressant with a serotonergic, noradrenergic, dopaminergic or monoamine oxidase inhibiting mechanism).
For accurate interpretation of [123I]FP-CIT binding to SERT, knowledge of potential influencing factors such as age or gender dependencies is essential. An age-related decline in SERT binding has been described using other radioligands [20–27]. However, post-mortem studies have not confirmed effects of aging on SERT mRNA availability [28–32].
The aim of this study was to explore age and gender influences on extrastriatal binding of [123I]FP-CIT to SERT in healthy volunteers using the data from a well-defined cohort of a large multicentre trial.
Methods
Subjects
Included in this prospective study were 103 healthy individuals free of neurological and psychiatric diseases (46 women, 57 men; age range 21 – 83 years, mean 51.8 ± 17.8 years). The study population is part of the ENC-DAT (European Normal Control Database of DaTSCAN) database established as an initiative of the Neuroimaging Committee of the European Association of Nuclear Medicine and includes data from 13 different imaging centres. All subjects had to fulfil predefined criteria of normality without any significant clinical abnormalities in medical history, blood chemistry, neurological examination (including the Unified Parkinson’s Disease Rating Scale score) and psychiatric evaluation including the Symptom Checklist-90 revised (score <63) [33] and the Beck Depression Inventory (score <9) self-assessment scales [34]. Cognitive deficits as assessed by the Mini-Mental State Examination (score ≥28) were ruled out. Furthermore, a history of Parkinsonian syndromes in first-degree relatives was an exclusion criterion. The study population had a balanced gender and age distribution. The average ages were comparable between the women (51.3 ± 17.7 years) and the men (52.1 ± 18.1 years).
Each subject underwent MRI examination according to the protocols of the respective imaging centre to detect potential structural pathologies. Pregnancy was ruled out in the women by urinary pregnancy testing. In addition, all subjects underwent urine drug testing. Approval of the ethics committee and the local authorities was obtained and all subjects signed written informed consent. Further details have been reported previously [35].
SPECT imaging
Stringent quality control protocols were applied at each of the 13 imaging sites [36]. Uniformity and centre of rotation were continuously maintained. In addition, 123I SPECT images of an anthropomorphic striatal phantom (Radiology Support Devices Inc., Long Beach, CA) were acquired in each of the participating centres according to a protocol published elsewhere [37] to calibrate the gamma camera systems on 17 imaging systems: four Siemens ECAM, three GE Infinia, three Philips IRIX, two Siemens SYMBIA, two Trionix Triad XLT 20, one GE Millennium VG, one Siemens MultiSPECT, and one Mediso x-Ring/4HR.
[123I]FP-CIT (180 ± 16 MBq) was injected intravenously as a bolus. SPECT images were acquired 3.0 ± 0.3 h after tracer injection. Acquisition parameters were: fixed rotational radius between 13 and 15 cm, matrix 128 × 128, angular sampling ≤3° (360° rotation), and hardware zoom of 1.23 to 2.00 to achieve a pixel size of 2 – 3 mm. The photopeak was set to 159 keV ±10 %. The acquisition time was chosen to obtain at least 2 million counts per study. Further information on SPECT system configuration and the scanning procedure has been reported previously [35].
In the subset of the ENC-DAT database reported here, scans were reconstructed using HERMES hybrid reconstruction (Hermes Medical Solutions, Stockholm, Sweden) using ordered subsets expectation maximization (OSEM) with 16 iterations and four or five subsets depending on the number of projections. To obtain a high level of standardization of scans with different camera systems and to reduce partial volume effects when evaluating small structures such as the pons, all scans were corrected for
-
1.
Attenuation: Chang method [38] with automatically generated ellipses, and an attenuation coefficient μ of 0.146 has been used, the high value for μ corresponding to the “narrow beam attenuation coefficient” that is recommended when scatter correction is applied [39].
-
2.
Scatter: A Monte-Carlo based scatter correction was applied using the HERMES Monte Carlo simulator [40]. Basically this method uses reconstruction-based scatter compensation with Monte Carlo modelling of scatter. It includes the simulation of the pathways of a large number of photons accelerated by a coarse grid and intermittent scatter modelling without simulation of septal penetration.
-
3.
Resolution recovery: Correction for depth-dependent detector response was done separately for each camera model using calculated point-spread functions based on the exact geometry of the respective collimator as well as the scanning geometry of the detector orbit [41].
Three-dimensional gaussian postfiltering was applied using a kernel with full-width at half-maximum (FWHM) of 7 mm, resulting in an estimated image FWHM of approximately 8 – 10 mm (more details are provided by Dickson et al. [36]).
Automated semiquantitative evaluation method
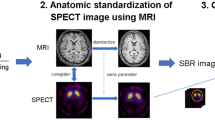
Semiquantitative evaluation of the SPECT data was performed using the brain analysis software (BRASS, version 3.6; Hermes Medical Solutions, Stockholm, Sweden). The software automatically performs spatial coregistration of individual patient images to a [123I]FP-CIT healthy control template using a registration algorithm based on mutual information and optimized for [123I]FP-CIT images. The accuracy of the coregistration of scans to the template was confirmed in all subjects. The template itself was derived using the 103 normal control scans, which were spatially normalized to the Montreal Neurological Institute standard MRI template (MNI; McGill University, Montreal QC, Canada) [42]. Next, a standard set of 3-D VOIs defining the thalamus and the putamen based on the Automated Anatomical Labelling (AAL) atlas [43] as well as a spherical VOI for the pons was created. An occipital cortex (OC) VOI served as the reference region. The respective VOIs are shown in Fig. 1. All VOIs were applied to the SPECT data, and manually adjusted (drag and drop) when necessary to ensure positional accuracy. The pons VOI was positioned to cover the uptake in the area of the raphe nuclei. Mean counts per voxel were calculated for each VOI. Specific binding (SB) ratios in the predefined ESTR in relation to the OC were calculated according to the formula:

VOIs used for semiquantitative analysis and corresponding SPECT template (left column colour scale thresholds adjusted to depict the respective structures)
Statistics
Descriptive statistics are given as means and standard deviation. Comparisons between and within groups were tested with independent group or paired Student's t tests, respectively. The relationship between age and SERT binding was analysed using linear regression and described by Pearson correlation coefficients. To verify differences in the slopes of the linear regression curves between male and female subjects and therefore different gender profiles of age effects, the effect of gender on the slopes of the regression lines was tested by analysis of covariance investigating the significance of the interaction between the classification effect (gender) and the covariate (measured SB). Analyses of covariance was used to determine the influence of gender, age and striatal binding on extrastriatal binding. To control for confounding factors, partial correlations were calculated. All statistical analyses were performed using SPSS software version 13.0 (SPSS Inc, Chicago, IL).
Results
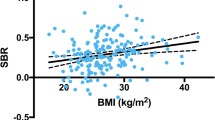
The age distributions of the men and women were balanced (p = 0.814). Measured specific SERT binding ratios in both the thalamus and pons showed considerable variability across the full age range (Fig. 2) with thalamic binding ratios in general being significantly higher than pons binding ratios (0.35 ± 0.17 vs. 0.26 ± 0.21, p = 0.001).

Correlations between age and [123I]FP-CIT binding ratios in (a) the thalamus and (b) the pons
Mean SB ratios in the thalamus were significantly higher in women than in men (0.40 ± 0.15 vs. 0.31 ± 0.17, p = 0.003). Mean SB ratios in the pons were slightly higher in men than in women (0.29 ± 0.19 vs. 0.22 ± 0.23), but this difference did not reach the level of significance (p = 0.077). A linear fit showed an age-related decline in [123I]FP-CIT binding ratios in both the thalamus and the pons (Fig. 2). The corresponding regression parameters, Pearson correlation coefficients and p values are given in Table 1 (for comparison these values are also given for the putamen). Correlation coefficients were stronger for the thalamus than for the pons. Correlations were significant for the entire cohort as well as for men and women, with only one exception: the correlation between age and SB ratios in the pons in women failed to reach the level of significance. Extrastriatal binding ratios showed a reduction with normal aging with average (±standard error) declines per decade of 8.2 ± 1.3 % in the thalamus and 6.8 ± 2.9 % in the pons.
The declines in binding ratios per decade in the thalamus and in the pons were not different between men (thalamus 9.0 ± 1.9 %, pons 7.9 ± 2.7 %) and women (thalamus 7.1 ± 1.6 %, analysis of covariance p = 0.61; pons 4.3 ± 7.0 %, p = 0.10). Specific thalamic binding ratios were also correlated with putaminal binding ratios (Pearson’s correlation coefficient 0.35, p < 0.001), whereas no correlation was found between pons and putaminal binding ratios (correlation coefficient 0.11, p = 0.29; Fig. 3). Controlling for putaminal binding ratios with partial correlations, age effects remained stable in both the thalamus (p < 0.001) and pons (p = 0.043).

Correlations between putaminal [123I]FP-CIT binding ratios and (a) thalamic binding ratios and (b) pons binding ratios
Discussion
To our knowledge this is the largest study to systematically evaluate extrastriatal binding of the commercially available DAT tracer [123I]FP-CIT in a cohort of healthy controls with a wide age range and with well-defined criteria of normality. The study population had balanced age distribution across the whole age range as well as an even gender distribution. The measured specific thalamic [123I]FP-CIT binding ratios were similar to those recently reported by Borgers et al. [12] and Koopman et al. [13]. As expected, SB ratios in SERT-rich ESTR were considerably lower than in the DAT-rich striatum, owing to the lower affinity of [123I]FP-CIT for SERT than for DAT [5, 44] and the overall lower expression of SERT in the brainstem and thalamus in comparison to the striatal DAT expression [45, 46].
There was high variability (high standard deviation compared to the average) of extrastriatal radiotracer binding across the entire age range. A drug-induced reduction due to potential blocking effects of SSRIs [10, 11] or other psychotropic drugs were excluded as all subjects were drug-naive and urine drug screening revealed no abnormalities. Also psychiatric disorders as potential confounding factors were ruled out. In line with our results, similar high interindividual variations in extrastriatal binding have also been found using other SPECT and PET tracers [10, 13, 47–50]. Ziebell et al. [10] discussed potential reasons for this variability. It could be attributed to variation in SERT density, the relatively low [123I]FP-CIT binding affinity to SERT with consequently relatively low binding ratios, or relative DAT versus SERT density ratios in the analysed regions.
We observed a significant correlation between thalamic (but not pons) radiotracer binding and putaminal binding. A similar finding was reported by Ryding et al. [26] for the thalamus using ([123I]β-CIT). Visual image analysis revealed potential spill-in of striatal counts into the thalamic VOI. Despite applying resolution modelling and scatter correction, spill-in of counts cannot be entirely eliminated [51] and might have led to a stronger observed correlation than could be attributed to direct thalamic DAT radiotracer binding, since DAT density in the thalamus is known to be relatively low [52]. Potential spill-in might limit the specific analysis of SERT in the thalamus and (apart from potential biological binding differences, partial volume effects and VOI sizes) could also contribute to the higher radiotracer uptake observed in the thalamus than in the pons. Eventually this might also account for the significantly higher thalamic uptake in women than in men, due to the well-documented gender dependency of DAT binding [53, 54]. Borgers et al. [12] analysed binding of [123I]FP-CIT in the hypothalamus in healthy controls, patients with pituitary insufficiency and patients with hypothalamic impairment, but found no differences in binding ratios in the hypothalamus among these groups, although SERT appears to play a key role in the hypothalamus [55]. The assumed spill-in of counts from striatal DAT binding in combination with the overall low specific [123I]FP-CIT binding ratios in the thalamus may have eventually masked the expected group differences. In our subjects, the pons region did not appear to be influenced by striatal binding. Although higher radiotracer binding in women than in men has been reported in this region for other radiotracers [53, 56], and despite preclinical evidence of protective effects of oestrogens on SERT [57], we were not able to show significant gender effects on [123I]FP-CIT binding. We found a significant age dependency of [123I]FP-CIT binding in both the thalamus and the pons. These age effects remained significant after controlling for potential spill-in from the putamen using partial correlation analyses.
Post-mortem studies with [3H]imipramine [29–31] and [3H]paroxetine [28, 32] did not reveal any age-dependent decline in SERT expression in the thalamus or brainstem. The inability of these studies to demonstrate age-dependency could potentially be explained by their limited sample size, low age range of the subjects and limited selectivity of the ligands used. Most neuroimaging studies have confirmed effects of healthy aging on SERT. Using [123I]β-CIT, several studies have shown a decline in thalamus binding per decade in the range 3.2 % to 7.2 % and in midbrain binding in the range 4.2 % to 8.3 % [22, 25, 27]. We obtained higher values (8.6 % in the thalamus and 7.1 % in the pons) which lie in a similar range to those reported for DAT [58–61]. Binding loss with healthy aging seems to vary depending on which radiotracer is used (possibly attributable to different levels of specific to nonspecific binding as well as the contribution of SERT to the reference region used). Using the more SERT-selective tracer 2-((2-((dimethylamino)methyl)phenyl)thio)-5-[123I]iodophenylamine ([123I]ADAM), a low decline of only 3.0 % per decade in the midbrain was reported by Newberg et al. [24] and using [123I]2β-carbomethoxy-3β-(4-iodophenyl)nortropane ([123I]Nor-β-CIT) a decline of 2.0 % per decade was reported by Kuikka et al. [23]. In young subjects up to 35 years of age, Buchert et al. found no relevant influence of aging on SERT [56] using [11C]McN5652 and PET. Aging effects in young subjects appear not to be relevant. On the other hand, the finding could also indicate a nonlinear relationship between age and SERT binding that cannot be entirely ruled out based on our data. Nonlinear fits did not provide usable results in our study population due to the observed high variation of extrastriatal binding.
There are some limitations to consider when interpreting our results. First, [123I]FP-CIT has higher affinity to DAT than to SERT [5, 44]. There is evidence of the presence of some DAT expression in the midbrain [62], potentially also resulting in a small influence on the pons binding observed. We controlled for this statistically using partial correlations. Age effects remained stable when controlling for DAT binding ratios measured in the putamen. For [123I]β-CIT, attempts have been made to separate DAT and SERT binding based on the different uptake kinetics and on SERT blocking with selective SSRI [26]. Using this method, Ryding et al. observed no age dependency of SERT binding, but the sample size (23 healthy controls) is considerably lower than in our study. More accurate separation could be achieved using more selective SERT ligands such as [123I]ADAM [63]. Second, our results were based on a variety of different imaging equipment, potentially explaining some of the interindividual variation observed. Phantom calibration [37] was validated for striatal DAT binding only, and not for extrastriatal SERT-rich regions. However, extensive efforts for standardization of acquisition protocols and camera-specific resolution modelling in the reconstruction process were made, and all scans were processed and evaluated in a single centre. Third, apart from resolution modelling in the reconstruction process, no additional MRI-based recovery correction was performed to reduce potential pons atrophy effects with aging. Previous studies examining age-related volumetric decline in the brainstem, however, have shown no overall volume loss in this area [64, 65].
Fourth, we did not correct for other potential confounding factors such as seasonal variability in SERT availability [56]. Also polymorphism in the SERT promoter gene has been reported, that can potentially regulate SERT expression [66] possibly modulated by a family history of axis-I disorders. A family history of axis-I disorders was an exclusion criterion. Fifth, in line with most other groups, we used the OC as the reference region for both SERT and DAT analysis which contains a low (but presumably not relevant) concentration of SERT [45, 67]. Age effects could be underestimated if age-related decline in the occipital reference region occurs in a similar proportion as in the thalamus or pons. We did not use the cerebellum as the reference region, since attenuation correction in this area is problematic and would have introduced additional variability. In addition, in clinical routine imaging, the cerebellum is often not covered entirely, limiting the use of a cerebellar reference region.
Conclusion
Imaging with the radioligand [123I]FP-CIT, that is commercially widely available and approved for specific applications, may allow the evaluation of DAT and SERT in a single imaging session. [123I]FP-CIT binding in the thalamus as well as in the pons showed high interindividual variation most likely hampering accurate interpretation of SERT expression on an individual basis. The additional information on SERT binding, however, may provide new insights into neurological and psychiatric diseases such as shown for Parkinson’s disease and DLB [14, 15] in research trials in which [123I]FP-CIT and SPECT are used. The data could also be used as a reference to estimate SERT occupancy in addition to nigrostriatal integrity when using [123I]FP-CIT for DAT imaging in patients treated with selective SSRIs to individualize treatment of depression, a common nonmotor symptom in Parkinson’s disease.
References
Booij J, Speelman JD, Horstink MW, Wolters EC. The clinical benefit of imaging striatal dopamine transporters with [123I]FP-CIT SPET in differentiating patients with presynaptic parkinsonism from those with other forms of parkinsonism. Eur J Nucl Med. 2001;28:266–72.
Benamer TS, Patterson J, Grosset DG, Booij J, de Bruin K, van Royen E, et al. Accurate differentiation of parkinsonism and essential tremor using visual assessment of [123I]-FP-CIT SPECT imaging: the [123I]-FP-CIT study group. Mov Disord. 2000;15:503–10.
Darcourt J, Booij J, Tatsch K, Varrone A, Vander Borght T, Kapucu OL, et al. EANM procedure guidelines for brain neurotransmission SPECT using (123)I-labelled dopamine transporter ligands, version 2. Eur J Nucl Med Mol Imaging. 2010;37:443–50. doi:10.1007/s00259-009-1267-x.
Walker Z, Cummings JL. [123I]N-omega-fluoropropyl-2beta-carbomethoxy-3beta-(4-iodophenyl)nortropane single-photon emission computed tomography brain imaging in the diagnosis of dementia with Lewy bodies. Alzheimers Dement. 2012;8:74–83. doi:10.1016/j.jalz.2011.08.003.
Abi-Dargham A, Gandelman MS, DeErausquin GA, Zea-Ponce Y, Zoghbi SS, Baldwin RM, et al. SPECT imaging of dopamine transporters in human brain with iodine-123-fluoroalkyl analogs of beta-CIT. J Nucl Med. 1996;37:1129–33.
Hall H, Halldin C, Guilloteau D, Chalon S, Emond P, Besnard J, et al. Visualization of the dopamine transporter in the human brain postmortem with the new selective ligand [125I]PE2I. Neuroimage. 1999;9:108–16.
Madras BK, Gracz LM, Fahey MA, Elmaleh D, Meltzer PC, Liang AY, et al. Altropane, a SPECT or PET imaging probe for dopamine neurons: III. Human dopamine transporter in postmortem normal and Parkinson's diseased brain. Synapse. 1998;29:116–27. doi:10.1002/(SICI)1098-2396(199806)29:2<116::AID-SYN3>3.0.CO;2-A.
Varnas K, Halldin C, Hall H. Autoradiographic distribution of serotonin transporters and receptor subtypes in human brain. Hum Brain Mapp. 2004;22:246–60. doi:10.1002/hbm.20035.
Staley JK, Basile M, Flynn DD, Mash DC. Visualizing dopamine and serotonin transporters in the human brain with the potent cocaine analogue [125I]RTI-55: in vitro binding and autoradiographic characterization. J Neurochem. 1994;62:549–56.
Ziebell M, Holm-Hansen S, Thomsen G, Wagner A, Jensen P, Pinborg LH, et al. Serotonin transporters in dopamine transporter imaging: a head-to-head comparison of dopamine transporter SPECT radioligands 123I-FP-CIT and 123I-PE2I. J Nucl Med. 2010;51:1885–91. doi:10.2967/jnumed.110.078337.
Booij J, de Jong J, de Bruin K, Knol R, de Win MM, van Eck-Smit BL. Quantification of striatal dopamine transporters with 123I-FP-CIT SPECT is influenced by the selective serotonin reuptake inhibitor paroxetine: a double-blind, placebo-controlled, crossover study in healthy control subjects. J Nucl Med. 2007;48:359–66.
Borgers AJ, Alkemade A, Van de Giessen EM, Drent ML, Booij J, Bisschop PH, et al. Imaging of serotonin transporters with [123I]FP-CIT SPECT in the human hypothalamus. EJNMMI Res. 2013;3:34. doi:10.1186/2191-219X-3-34.
Koopman KE, la Fleur SE, Fliers E, Serlie MJ, Booij J. Assessing the optimal time point for the measurement of extrastriatal serotonin transporter binding with 123I-FP-CIT SPECT in healthy, male subjects. J Nucl Med. 2012;53:1087–90. doi:10.2967/jnumed.111.102277.
Hesse S, Meyer PM, Strecker K, Barthel H, Wegner F, Oehlwein C, et al. Monoamine transporter availability in Parkinson's disease patients with or without depression. Eur J Nucl Med Mol Imaging. 2009;36:428–35. doi:10.1007/s00259-008-0979-7.
Roselli F, Pisciotta NM, Pennelli M, Aniello MS, Gigante A, De Caro MF, et al. Midbrain SERT in degenerative parkinsonisms: a 123I-FP-CIT SPECT study. Mov Disord. 2010;25:1853–9. doi:10.1002/mds.23179.
Booij J, Hemelaar TG, Speelman JD, de Bruin K, Janssen AG, van Royen EA. One-day protocol for imaging of the nigrostriatal dopaminergic pathway in Parkinson's disease by [123I]FPCIT SPECT. J Nucl Med. 1999;40:753–61.
Rocha FL, Murad MG, Stumpf BP, Hara C, Fuzikawa C. Antidepressants for depression in Parkinson's disease: systematic review and meta-analysis. J Psychopharmacol. 2013;27:417–23. doi:10.1177/0269881113478282.
Kugaya A, Sanacora G, Staley JK, Malison RT, Bozkurt A, Khan S, et al. Brain serotonin transporter availability predicts treatment response to selective serotonin reuptake inhibitors. Biol Psychiatry. 2004;56:497–502. doi:10.1016/j.biopsych.2004.07.001.
Lanzenberger R, Kranz GS, Haeusler D, Akimova E, Savli M, Hahn A, et al. Prediction of SSRI treatment response in major depression based on serotonin transporter interplay between median raphe nucleus and projection areas. Neuroimage. 2012;63:874–81. doi:10.1016/j.neuroimage.2012.07.023.
Dahlstrom M, Ahonen A, Ebeling H, Torniainen P, Heikkila J, Moilanen I. Elevated hypothalamic/midbrain serotonin (monoamine) transporter availability in depressive drug-naive children and adolescents. Mol Psychiatry. 2000;5:514–22.
Heinz A, Ragan P, Jones DW, Hommer D, Williams W, Knable MB, et al. Reduced central serotonin transporters in alcoholism. Am J Psychiatry. 1998;155:1544–9.
Hesse S, Barthel H, Murai T, Muller U, Muller D, Seese A, et al. Is correction for age necessary in neuroimaging studies of the central serotonin transporter? Eur J Nucl Med Mol Imaging. 2003;30:427–30. doi:10.1007/s00259-002-1044-6.
Kuikka JT, Tammela L, Bergstrom KA, Karhunen L, Uusitupa M, Tiihonen J. Effects of ageing on serotonin transporters in healthy females. Eur J Nucl Med. 2001;28:911–3.
Newberg AB, Amsterdam JD, Wintering N, Ploessl K, Swanson RL, Shults J, et al. 123I-ADAM binding to serotonin transporters in patients with major depression and healthy controls: a preliminary study. J Nucl Med. 2005;46:973–7.
Pirker W, Asenbaum S, Hauk M, Kandlhofer S, Tauscher J, Willeit M, et al. Imaging serotonin and dopamine transporters with 123I-beta-CIT SPECT: binding kinetics and effects of normal aging. J Nucl Med. 2000;41:36–44.
Ryding E, Lindstrom M, Bradvik B, Grabowski M, Bosson P, Traskman-Bendz L, et al. A new model for separation between brain dopamine and serotonin transporters in 123I-beta-CIT SPECT measurements: normal values and sex and age dependence. Eur J Nucl Med Mol Imaging. 2004;31:1114–8. doi:10.1007/s00259-004-1489-x.
van Dyck CH, Malison RT, Seibyl JP, Laruelle M, Klumpp H, Zoghbi SS, et al. Age-related decline in central serotonin transporter availability with [(123)I]beta-CIT SPECT. Neurobiol Aging. 2000;21:497–501.
Arranz B, Eriksson A, Mellerup E, Plenge P, Marcusson J. Effect of aging in human cortical pre- and postsynaptic serotonin binding sites. Brain Res. 1993;620:163–6.
Allen SJ, Benton JS, Goodhardt MJ, Haan EA, Sims NR, Smith CC, et al. Biochemical evidence of selective nerve cell changes in the normal ageing human and rat brain. J Neurochem. 1983;41:256–65.
Severson JA, Marcusson JO, Osterburg HH, Finch CE, Winblad B. Elevated density of [3H]imipramine binding in aged human brain. J Neurochem. 1985;45:1382–9.
Marcusson JO, Alafuzoff I, Backstrom IT, Ericson E, Gottfries CG, Winblad B. 5-Hydroxytryptamine-sensitive [3H]imipramine binding of protein nature in the human brain. II. Effect of normal aging and dementia disorders. Brain Res. 1987;425:137–45.
Andersson A, Sundman I, Marcusson J. Age stability of human brain 5-HT terminals studied with [3H]paroxetine binding. Gerontology. 1992;38:127–32.
Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatric rating scale – preliminary report. Pychopharmacol Bull. 1973;1:13–28.
Beck AT, Steer RA. Beck depression inventory–manual. San Antonio: The Psychological Association; 1987.
Varrone A, Dickson JC, Tossici-Bolt L, Sera T, Asenbaum S, Booij J, et al. European multicentre database of healthy controls for [123I]FP-CIT SPECT (ENC-DAT): age-related effects, gender differences and evaluation of different methods of analysis. Eur J Nucl Med Mol Imaging. 2013;40:213–27. doi:10.1007/s00259-012-2276-8.
Dickson JC, Tossici-Bolt L, Sera T, de Nijs R, Booij J, Bagnara MC, et al. Proposal for the standardisation of multi-centre trials in nuclear medicine imaging: prerequisites for a European 123I-FP-CIT SPECT database. Eur J Nucl Med Mol Imaging. 2012;39:188–97. doi:10.1007/s00259-011-1884-z.
Tossici-Bolt L, Dickson JC, Sera T, de Nijs R, Bagnara MC, Jonsson C, et al. Calibration of gamma camera systems for a multicentre European 123I-FP-CIT SPECT normal database. Eur J Nucl Med Mol Imaging. 2011;38:1529–40. doi:10.1007/s00259-011-1801-5.
Chang L. A method for attenuation correction in radionuclide computed tomography. IEEE Trans Nucl Sci. 1978;21:638–43.
Willowson K, Bailey D, Schembri G, Baldock C. CT-based quantitative SPECT for the radionuclide 201Tl: experimental validation and a standardized uptake value for brain tumour patients. Cancer Imaging. 2012;12:31–40.
Sohlberg A, Watabe H, Iida H. Acceleration of Monte Carlo-based scatter compensation for cardiac SPECT. Phys Med Biol. 2008;53:N277–85. doi:10.1088/0031-9155/53/14/N02.
Sohlberg A, Watabe H, Iida H. Optimal collimator design for cardiac SPECT when resolution recovery is applied in statistical reconstruction. J Nucl Med. 2007;48 Suppl 2:721P.
Collins DL, Neelin P, Peters TM, Evans AC. Automatic 3D intersubject registration of MR volumetric data in standardized Talairach space. J Comput Assist Tomogr. 1994;18:192–205.
Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage. 2002;15:273–89. doi:10.1006/nimg.2001.0978.
Laruelle M, Slifstein M, Huang Y. Relationships between radiotracer properties and image quality in molecular imaging of the brain with positron emission tomography. Mol Imaging Biol. 2003;5:363–75.
Backstrom I, Bergstrom M, Marcusson J. High affinity [3H]paroxetine binding to serotonin uptake sites in human brain tissue. Brain Res. 1989;486:261–8.
De Keyser J, De Backer JP, Ebinger G, Vauquelin G. [3H]GBR 12935 binding to dopamine uptake sites in the human brain. J Neurochem. 1989;53:1400–4.
Kupers R, Frokjaer VG, Erritzoe D, Naert A, Budtz-Joergensen E, Nielsen FA, et al. Serotonin transporter binding in the hypothalamus correlates negatively with tonic heat pain ratings in healthy subjects: a [11C]DASB PET study. Neuroimage. 2011;54:1336–43. doi:10.1016/j.neuroimage.2010.09.010.
Chou YH, Yang BH, Chung MY, Chen SP, Su TP, Chen CC, et al. Imaging the serotonin transporter using (123)I-ADAM in the human brain. Psychiatry Res. 2009;172:38–43. doi:10.1016/j.pscychresns.2008.12.006.
van de Giessen E, Booij J. The SPECT tracer [123I]ADAM binds selectively to serotonin transporters: a double-blind, placebo-controlled study in healthy young men. Eur J Nucl Med Mol Imaging. 2010;37:1507–11. doi:10.1007/s00259-010-1424-2.
Koch W, Schaaff N, Popperl G, Mulert C, Juckel G, Reicherzer M, et al. [I-123]ADAM and SPECT in patients with borderline personality disorder and healthy control subjects. J Psychiatry Neurosci. 2007;32:234–40.
Du Y, Tsui BM, Frey EC. Model-based compensation for quantitative 123I brain SPECT imaging. Phys Med Biol. 2006;51:1269–82. doi:10.1088/0031-9155/51/5/016.
Sun J, Xu J, Cairns NJ, Perlmutter JS, Mach RH. Dopamine D1, D2, D3 receptors, vesicular monoamine transporter type-2 (VMAT2) and dopamine transporter (DAT) densities in aged human brain. PLoS One. 2012;7:e49483. doi:10.1371/journal.pone.0049483.
Staley JK, Krishnan-Sarin S, Zoghbi S, Tamagnan G, Fujita M, Seibyl JP, et al. Sex differences in [123I]beta-CIT SPECT measures of dopamine and serotonin transporter availability in healthy smokers and nonsmokers. Synapse. 2001;41:275–84. doi:10.1002/syn.1084.
Lavalaye J, Booij J, Reneman L, Habraken JB, van Royen EA. Effect of age and gender on dopamine transporter imaging with [123I]FP-CIT SPET in healthy volunteers. Eur J Nucl Med. 2000;27:867–9.
Amir S, Robinson B, Ratovitski T, Rea MA, Stewart J, Simantov R. A role for serotonin in the circadian system revealed by the distribution of serotonin transporter and light-induced Fos immunoreactivity in the suprachiasmatic nucleus and intergeniculate leaflet. Neuroscience. 1998;84:1059–73.
Buchert R, Schulze O, Wilke F, Berding G, Thomasius R, Petersen K, et al. Is correction for age necessary in SPECT or PET of the central serotonin transporter in young, healthy adults? J Nucl Med. 2006;47:38–42.
Sanchez MG, Morissette M, Di Paolo T. Oestradiol modulation of serotonin reuptake transporter and serotonin metabolism in the brain of monkeys. J Neuroendocrinol. 2013;25:560–9. doi:10.1111/jne.12034.
Volkow ND, Fowler JS, Wang GJ, Logan J, Schlyer D, MacGregor R, et al. Decreased dopamine transporters with age in healthy human subjects. Ann Neurol. 1994;36:237–9.
De Keyser J, Ebinger G, Vauquelin G. Age-related changes in the human nigrostriatal dopaminergic system. Ann Neurol. 1990;27:157–61.
Mozley PD, Acton PD, Barraclough ED, Plossl K, Gur RC, Alavi A, et al. Effects of age on dopamine transporters in healthy humans. J Nucl Med. 1999;40:1812–7.
Schwarz J, Storch A, Koch W, Pogarell O, Radau PE, Tatsch K. Loss of dopamine transporter binding in Parkinson's disease follows a single exponential rather than linear decline. J Nucl Med. 2004;45:1694–7.
Bannon MJ, Whitty CJ. Age-related and regional differences in dopamine transporter mRNA expression in human midbrain. Neurology. 1997;48:969–77.
Booij J, de Win MM. Brain kinetics of the new selective serotonin transporter tracer [123I]ADAM in healthy young adults. Nucl Med Biol. 2006;33:185–91. doi:10.1016/j.nucmedbio.2005.10.005.
Lee NJ, Park IS, Koh I, Jung TW, Rhyu IJ. No volume difference of medulla oblongata between young and old Korean people. Brain Res. 2009;1276:77–82. doi:10.1016/j.brainres.2009.04.027.
Raz N, Gunning-Dixon F, Head D, Williamson A, Acker JD. Age and sex differences in the cerebellum and the ventral pons: a prospective MR study of healthy adults. AJNR Am J Neuroradiol. 2001;22:1161–7.
Shioe K, Ichimiya T, Suhara T, Takano A, Sudo Y, Yasuno F, et al. No association between genotype of the promoter region of serotonin transporter gene and serotonin transporter binding in human brain measured by PET. Synapse. 2003;48:184–8. doi:10.1002/syn.10204.
Laruelle M, Vanisberg MA, Maloteaux JM. Regional and subcellular localization in human brain of [3H]paroxetine binding, a marker of serotonin uptake sites. Biol Psychiatry. 1988;24:299–309.
Acknowledgments
The participating centres thank GE Healthcare and the German Parkinson Association for their financial contribution to this study, ABX-CRO for managing the network activities and the Executive Committee of the EANM for establishing EANM Research Ltd. (EARL) as an administrative framework for this project.
The authors also thank the personnel of each Nuclear Medicine Centre responsible for the quality controls and acquisition of the SPECT data.
Disclosure
Prof. Jan Booij and Koen Van Laere have acted as neuroimaging consultants for GE Healthcare in the context of [123I]FP-CIT scans.
Author information
Authors and Affiliations
Corresponding author
Additional information
Walter Koch and Marcus Unterrainer share first authorship.
Rights and permissions
About this article

Cite this article
Koch, W., Unterrainer, M., Xiong, G. et al. Extrastriatal binding of [123I]FP-CIT in the thalamus and pons: gender and age dependencies assessed in a European multicentre database of healthy controls. Eur J Nucl Med Mol Imaging 41, 1938–1946 (2014). https://doi.org/10.1007/s00259-014-2785-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-014-2785-8