
Abstract
Purpose
The purpose of this pilot study was to assess whether outcome in metastatic or recurrent breast cancer patients is related to metabolic response to endocrine therapy determined by 18F-FDG PET/CT.
Methods
The study group comprised 22 patients with breast cancer (age 58 ± 11 years, mean ± SD) who were scheduled to receive endocrine therapy. They were systematically assessed by PET/CT at baseline and after a mean of 10 ± 4 weeks for evaluation of response after induction. All patients demonstrated FDG-avid lesions on the baseline PET/CT scan. The metabolic response was assessed according to EORTC criteria and based on the mean difference in SUVmax between the two PET/CT scans, and the patients were classified into four groups: complete or partial metabolic response, or stable or progressive metabolic disease (CMR, PMR, SMD and PMD, respectively). All patients were followed in our institution.
Results
Metastatic sites were localized in bone (n = 15), lymph nodes (n = 11), chest wall (n = 3), breast (n = 5), lung (n = 3), soft tissue (n = 1) and liver (n = 1). PMR was observed in 11 patients (50%), SMD in 5 (23%) and PMD in 6 (27%). The median progression-free survival (PFS) times were 20, 27 and 6 months in the PMR, SMD and PMD groups, respectively. PFS in the SMD group differed from that in the PMR and SMD groups (p < 0.0001).
Conclusion
Metabolic response assessed by FDG PET/CT imaging in patients with metastatic breast cancer treated with endocrine therapy is predictive of the patients’ PFS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nearly 70% of all breast cancers express oestrogen receptors (ER), and this expression is recognized to be a favourable prognostic factor. A large proportion of patients, particularly postmenopausal women, would therefore benefit from endocrine therapy, which has moderate side effects, at many stages of the disease, especially in the presence of progressive disease in a local/regional and/or metastatic setting [1]. Endocrine sensitivity is linked to certain clinical benefits in 30–77% of patients at the initial stage, decreasing to 7–21% of patients with recurrent disease [2]. Endocrine therapy in the advanced disease setting constitutes a relatively low-toxicity treatment option for disease control and should be proposed as first-line treatment in most women with endocrine-sensitive metastatic breast cancer, i.e. with a long disease-free interval, no (or limited) visceral involvement, slow disease progression, limited metastatic sites and no disease-related symptoms [1]. Knowledge of endocrine receptor expression, usually determined at the time of primary diagnosis by immunohistochemistry, is essential to select the most appropriate therapy. However, ER determinations may be limited by sampling errors, heterogeneity of receptor content in the primary tumour, absence of endocrine receptor expression in metastatic and/or recurrent sites leading to discordance with the endocrine status of the primary breast tumour, and nonfunctionality of receptors. These limitations may explain why only 30–40% of patients with ER-positive breast cancer respond objectively to endocrine therapy. Except for the uncommon clinical flare reaction that occurs 7–10 days after induction of endocrine therapy, tumour response to endocrine therapy, as assessed by clinical, laboratory and imaging examinations, is generally delayed by several months after induction, compared to neoadjuvant chemotherapy [3].
Diagnostic imaging tools able to assess response to endocrine therapy are currently lacking, particularly those for evaluation of the impact of treatment on bone and lymph node metastases. During the past decade, the usefulness of 18F-FDG PET imaging has been demonstrated in patients with breast cancer, particularly for the assessment of tumour response to therapy. Most published studies have assessed tumour response to chemotherapy, especially in the neoadjuvant setting [4–10], and have demonstrated a high correlation with pathological response or predicted outcome in patients with metastatic disease [11–13]. Whole-body PET/CT imaging can be highly effective for assessing response to therapy in diffuse metastatic disease, especially in the skeleton, where morphological imaging modalities mostly fail. Several studies have shown that the metabolic flare reaction, corresponding to an increase in tumour FDG uptake 7–10 days after initiating endocrine therapy, is predictive of response [14, 15], but data are lacking on the delayed effect of endocrine therapy on tumour metabolism.
The purpose of this pilot study was to assess whether the outcome evaluated in terms of overall survival (OS) and progression-free survival (PFS) in patients with metastatic breast cancer receiving endocrine therapy is related to the metabolic response established by FDG PET/CT imaging.
Materials and methods
Study design
Inclusion and protocol
Patients with metastatic breast cancer who were scheduled to receive endocrine therapy were prospectively included from January 2003 to October 2006. According to National Comprehensive Cancer Network guidelines and consensus on medical treatment in metastatic breast cancer, all patients had hormone receptor-positive HER2-negative disease, no disease-related symptoms, no visceral involvement (with the exception of one small liver metastasis in a patient who refused chemotherapy), and a long disease-free interval. The endocrine receptor status was assessed for the primary tumour in all patients and for metastatic sites in three patients. Inclusion criteria included FDG-avid lesions on the baseline PET/CT scan (PET1), performed less than 7 days before induction of endocrine therapy. A second PET/CT scan (PET2) was performed for evaluation of response during the first weeks of therapy, and up to 4 months after induction of endocrine therapy. The optimal interval between the two PET/CT scans was determined as 8 ± 2 weeks (Fig. 1). Lesions seen on PET/CT in both the PET1 and PET2 scans were compared with morphological imaging, including CT, MRI, ultrasonography, standard radiography and bone scintigraphy. Serum CA 15-3 levels were consistently measured before each PET/CT scan. The study was approved by our institutional review board/local ethics committee, and all patients gave their informed consent.

Study timeline
Immunohistochemistry staining
Endocrine receptor expression was assessed using the antioestrogen receptor antibody Dako-ER 1D5 (Dako, Trappes, France) at a dilution of 1:30 and the antiprogesterone receptor antibody PR 1A6 (Novocastra Laboratories, Newcastle, UK) at a dilution of 1:30. C-erb-B-2 oncoprotein expression was detected using a polyclonal antibody (Dako) at a dilution of 1:300. Tumours were scored as positive for ER and progesterone receptors when nuclear staining was identified in at least 10% of cells and for c-erb-B-2 when definite membrane staining was identified in at least 10% of cells. Staining for these markers was classified as positive or negative (two-group classification).
Patient follow-up
All patients were followed in our institution for at least 4 years. Treatment decisions were based on clinical, laboratory or imaging data, including the PET/CT results, discussed during multidisciplinary ward rounds. PFS and OS were calculated, as all patients were followed, even after progression.
FDG PET/CT acquisition
PET/CT scans were performed with a Discovery LS (GE Healthcare, Waukesha, WI) with attenuation-corrected images and coregistered PET/CT images. Patients fasted for at least 6 h before the examination and blood glucose had to be less than 9 mmol/l before injection of FDG. FDG (5 MBq/kg) was injected intravenously using the arm opposite the breast cancer or into a dorsal vein of the foot. PET data were acquired 60 min after injection from skull to mid-thigh in 2-D mode, with 4 min per bed position. Patients were allowed to breathe freely and CT images were acquired without contrast enhancement.
PET/CT analysis
PET/CT scans were reviewed by two nuclear medicine physicians trained in PET imaging on an Advantage Windows workstation (GE Healthcare). FDG-avid target lesions were identified in each patient on PET1 and were followed on PET2. All target lesions on PET1 were confirmed to be metastatic by morphological imaging. Semiquantitative analyses were performed using the maximum standardized uptake value (SUVmax) calculated for each target on a 3-D volume of interest, according to the following formula:
The changes in SUVmax between the PET1 and PET2 scans were recorded for the seven highest SUVmax targets. The mean change in SUVmax of these targets (mΔSUVmax, in percent) was then calculated for each patient, allowing classification of patients according to EORTC criteria [16] into the following groups:
-
Complete metabolic response (CMR): complete resolution of 18F-FDG uptake in the tumour volume (indistinguishable from surrounding normal tissue).
-
Partial metabolic response (PMR): at least 25% reduction in tumour uptake.
-
Stable metabolic disease (SMD): less than 25% increase or less than 25% decrease in tumour 18F-FDG SUV and no visible increase in extent of tumour uptake.
-
Progressive metabolic disease (PMD): greater than 25% increase in 18F-FDG tumour SUV within the tumour region defined on the baseline scan, visible increase in the extent of 18F-FDG tumour uptake (>20% in the longest dimension) or appearance of new 18F-FDG uptake in metastatic lesions.
Statistical analysis
Survival curves were constructed using the Kaplan-Meier method [17] and compared with the log-rank test. Statistical analyses were performed using R 2.0.1 software.
Results
Population
Table 1 summarizes the patient characteristics.
The study group comprised 22 women aged 58 ± 11 years (mean ± SD; range 40–82 years, median 61 years). Primary tumours were invasive ductal carcinoma in 17 patients (77%), invasive lobular carcinoma in 2 patients and unknown in 3 patients. All tumours had biopsy-proven ER-positive status and 86% had progesterone receptor-positive status. Immunohistochemistry was performed on the primary tumour in all patients, and on metastases in three patients. Of the 22 patients, 15 (68%) had received at least one line of chemotherapy prior to this study, while only three patients had not received any adjuvant therapy, 16 (73%) had been previously treated with local/regional adjuvant radiotherapy, and 15 (68%) had received endocrine therapy. The time since the last dose of previous endocrine therapy and the start of new endocrine therapy was 17.8 ± 29.5 months (median 19.5 months, range 1–84 months). Four patients (18%) had metastatic disease at diagnosis and 18 (82%) relapsed (interval between initial diagnosis and metastasis: 9.5 ± 11 years). Metastatic disease was confirmed by additional morphological imaging or histopathology (available in three patients). Disease extension was multiorgan in 12 patients and confined to a single organ in 7 patients, and 3 patients had a single metastatic lesion (bone in two patients and lymph node in the third patient). Metastases were localized in bone 15 patients (68%), lymph nodes in 11 (50%), chest wall in 3 (14%), lung in 3 (14%), soft tissue in 1 (5%) and liver in 1 (5%). Five patients (23%) had an additional contralateral breast lesion. Exclusive endocrine therapy initiated in these patients consisted of aromatase inhibitors in 16 patients (73%), antioestrogens in 5 (23%) and progestogen in 1. In addition, 6 patients (27%) had combined therapy with LHRH agonist (Table 2). The duration of follow-up was 55.4 ± 19.4 months (median 54 months, range 16–96 months).
PET/CT analysis
A median of 3.2 PET/CT scans were performed per patient (mean 3.2 ± 1, range 2–5), corresponding to a total of 71 PET/CT scans. The median interval between the PET1 and PET2 scans was 9 weeks (mean 10 ± 4, range 5–18 weeks). The median SUVmax at baseline was 5.8 (mean 6.2 ± 2.6). According to EORTC criteria, using the mean change in SUVmax (mΔSUVmax) between the PET1 and PET2 scans (cut-off 25%), patients were classified as follows: 11 PMR (50%), 5 SMD (23%), 6 PMD (27%) and 0 CMR (Table 3).
The median decrease in mΔSUVmax was 45% (mean 50 ± 17%, range −31.6 to −82.6%) in the PMR group and 19% (mean 11 ± 15%, range −22.9 to +12.8%) in the SMD group (Fig. 2). In the six patients with PMD, four (67%) showed a new hypermetabolic metastatic lesion on the PET2 scan, localized in bone in two, in lymph nodes in one and in the contralateral breast in one. One patient had a marked increase in mΔSUVmax (+241%), and the only patient with a dissociated response was also classified as PMD (Fig. 3). This patient showed metastatic lesions in bone (T8 vertebra and iliac bone) and liver (right lobe) on the PET1 scan. The PET2 scan demonstrated an increased SUVmax in the liver lesion (∆SUVmax +48%), stability in the T8 lesion (ΔSUVmax +5%) and decreased uptake in the iliac bone lesion (ΔSUVmax −51%). No other new hypermetabolic lesions were detected. Due to the increased uptake in the liver lesion, this patient was classified as PMD. A contrast-enhanced CT scan and MRI performed 1 week after the PET2 scan confirmed progression of liver metastases, and the patient showed further signs of progression during the 6 months after induction of endocrine therapy. No difference in terms of organ sites was observed between the PMD and PMR groups, with a mean number of targets of 1.6 and 2, respectively.

Partial metabolic response. Axillary lymph node disease (arrows) is seen on the PET1 scan. Decreased uptake is apparent on the PET2 scan (60% decrease in SUVmax). Data were confirmed by MRI. The PFS was 76 months in this patient

Progressive metabolic disease. Bone (T8 vertebra) and liver metastases (arrows) are seen on the PET1 scan. Increased uptake in the liver lesion is apparent on the PET2 scan (48% increase in SUVmax), and liver progression was confirmed on an enhanced CT scan. The PFS was 7 months in this patient
Prognostic parameters
Progression-free survival
The median PFS for the overall population was 16 months (mean 21.6 ± 18.5, range 4–65 months). The median PFS was 20, 27 and 6 months in the PMR, SMD and PMD groups, respectively (Fig. 4). All patients in the PMD group showed documented progression within 7 months. Of note, three patients still had no signs of progression at the time of this analysis (one patient in the SMD group and two in the PMR group) after 53, 50 and 55 months of follow-up, respectively. The PFS in patients in the PMD group was significantly different from that in patients in the PMR group and SMD group (p < 0.0001, log-rank test). No significant difference was observed between the PFS in patients in the PMR group and SMD group (p = 0.603, log-rank test); these two groups were therefore combined. The difference in PFS was still highly significant between patients in the PMD group and those in the merged PMR and SMD groups (p < 0.0001, log-rank test; Fig. 5).

PFS in the PMR, SMD and PMD groups

PFS in the merged PMR and SMD in comparison with the PMD group
Overall survival
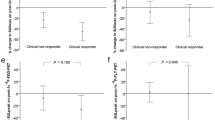
At the time of this analysis, 13 of the 22 patients (59%) were still alive. The median OS was 55, 71 and 52 months in the PMR, SMD and PMD groups, respectively (Fig. 6). No statistically significant differences was observed among the three groups (p = 0.338, log-rank test).

Overall survival in the PMR, SMD and PMD groups
Morphological imaging and CA 15-3 analysis
All lesions seen on the PET/CT scans were confirmed by morphological imaging including MRI (n = 14), contrast-enhanced CT (n = 9), bone scintigraphy (n = 7), standard radiography (n = 4), mammography (n = 2) and abdominal and pelvic ultrasonography (n = 1), or by fine-needle aspiration (n = 3). Morphological changes in bone lesions were assessed on the low-dose CT component of PET/CT in 13 of the 15 patients with bone metastases for whom CT data were available. The results were as follows:
-
Four patients in the PMR group and one patient in the SMD group showed osteolytic lesions that became osteoblastic.
-
Four patients in the PMD group showed osteolytic lesions that remained osteolytic.
-
Three patients in the PMR group showed osteoblastic lesions on the two PET/CT scans.
-
One patient in the SMD group showed mixed-pattern lesions.
Serum CA 15-3 levels (upper limit of normal values in healthy individuals 30 IU/ml) were measured before each PET/CT scan. Baseline serum CA 15-3 levels were less than 30 IU/ml in six patients. The CA 15-3 false-negative rate in this metastatic population was therefore 26%. No association between changes in CA 15-3 values and metabolic response was observed, but only limited variations in CA 15-3 values were observed in most patients (Table 1).
Discussion
In human breast cancer, assessment of tumour response to therapy is critical in order to avoid unnecessary side effects and ineffective treatment in nonresponders, and to allow a rapid change in treatment to ensure greater efficacy. This assessment is routinely based on clinical examination and morphological imaging, which both present certain limitations. The main limitation is that tumour response assessment is based on changes in the size of lesions, as illustrated by the use of the RECIST criteria (Response Evaluation Criteria in Solid Tumors), which do not reflect tumour cell viability. Moreover, these measurements are subject to interobserver variability, lack accuracy and are not suitable for assessment of tumour response to targeted therapies, particularly those with cytostatic effects. Molecular imaging allows noninvasive visualization of regional functional and molecular characteristics, and provides quantitative parameters. This is particularly true in bone-dominant disease, in which morphological modalities fail to assess tumour response [18] and in which endocrine therapy plays a major role. Tumour FDG uptake can therefore be used as a surrogate marker to monitor early response to therapy. This issue has been addressed in two studies focusing on morphological and metabolic changes in bone metastases in response to treatment [19, 20]. According to Du et al., progression of FDG uptake reflects the immediate tumour activity of bone metastases. [19]. Progression of osteoblastic changes during treatment, which can be explained by bone formation, is correlated with decreases in SUV and these two factors are predictive of response duration according to Tateishi et al. [20].
In previous studies assessing early tumour response to neoadjuvant chemotherapy by PET imaging, the most widely used criterion to differentiate responders from nonresponders was a cut-off for the percentage SUVmax change (∆SUVmax) between baseline and evaluation PET scans [4–10]. However, the use of this criterion has several limitations. First, SUVmax measurements have a number of shortcomings. SUVmax must be analysed with caution in the presence of elevated blood glucose and/or insulin levels; however, all patients in the present study were fasting and had a blood glucose level within the normal range. The reproducibility of SUVmax depends on the time between injection and acquisition, which must be similar between PET examinations in the same patient to allow valid comparison. It has recently been demonstrated that ∆SUVmax is influenced by the drug regimen [21], and the time between serial PET scans. Finally, an overlap of values in responders and nonresponders is not uncommon, and it is difficult to recommend a reference value for the ∆SUVmax cut-off value, since parameters were different between the various studies (chemotherapy regimens and number of cycles between the baseline and evaluation PET scans).
Only one study has focused on the assessment of response to neoadjuvant endocrine therapy by FDG PET/CT and discriminated responders from nonresponders using a decrease in SUVmax of 40% as the cut-off. The results were correlated with the Ki-67 labelling index, a proliferation biomarker, assessed 2 weeks after initiation of therapy [22]. A positive correlation between the percent Ki-67 labelling index and SUV uptake in primary tumours has been found in several studies [23–25]. This observation may explain why SUVmax decreased in the PMR group in our series with endocrine therapy, which was shown to reduce the Ki-67 labelling index in the affiliated IMPACT randomized trial [26]. Decreases in Ki-67 labelling index assessed 2 and 12 weeks after initiation of endocrine therapy [27] are significantly correlated with relapse-free survival in patients after surgery [28].
In the present study, determination of a cut-off in a selected group of metastatic patients did not appear to be relevant, and the criteria defined by the EORTC PET study group [16], validated in several solid tumour models and based on the SUVmax change on serial FDG-PET studies, were therefore used to classify tumour response. However, these criteria are based on cut-off values that are still open to debate, because they do not take into account the type of therapy and are not sufficiently accurate in borderline situations. We decided to use a reduction in mΔSUVmax of 25% as a cut-off value to define PMR, considering that the tumour response to endocrine therapy is slower than to chemotherapy, and according to the EORTC criteria which proposed a greater than 25% reduction in tumour SUV after more than one treatment cycle, although the minimum reduction in tumour SUV was 15 ± 25% after one cycle of chemotherapy [16]. The relevance of a cut-off of +25% to discriminate SMD from PMD or −25% to discriminate SMD from PMR might be questioned: four patients were in this situation in the present study with a mΔSUVmax between 21% and 33% (patients 7, 8, 11 and 18). The impact of this difficulty in classifying patients would appear to have been limited in the present study because patients in the PMR and SMD groups could be combined for statistical analysis, and most patients in the PMD group showed obvious new hypermetabolic lesions. Moreover, the mΔSUVmax is an approximate assessment for defined targets, limited to seven, and assessment of patients with several lesions remains more delicate. A dissociated response in the metastatic setting is not unusual: it was observed in 48% of a series of 46 metastatic breast cancer patients and has been shown to be associated with a poor prognosis, as assessed by a short time to progression [29].
To our knowledge, this is the first study to investigate the predictive value of metabolic response in breast cancer metastatic disease obtained after induction of endocrine therapy, and which demonstrates that PFS, one of the most widely used parameters to reflect outcome in oncology, is related to metabolic response. The main objective of endocrine therapy, which remains a palliative option in this population, is to obtain at least disease stabilization and at best a response. PET/CT seems to be a valuable tool to identify the subgroup of patients likely to benefit from continuation of therapy, as shown in our series. The PFS in patients in the PMD group was significantly different from the PFS in patients in the PMR and SMD groups (p < 0.0001), whereas the OS of patients in these various groups were not different (p = 0.338). This last observation could be explained by several factors: first, the high rate of patients still alive (13/22) after completion of the present study makes any conclusions based on OS analysis uncertain; second, it must be stressed that OS benefits from endocrine therapy are rarely observed in patients with metastatic disease. Moreover, increases or decreases in serum CA 15-3 levels were in agreement with the PET imaging results in only 66% of patients. This observation confirms that serum CA 15-3 assay, used as the sole criterion for assessment of response to therapy in metastatic breast cancer patients during active therapy, cannot be recommended and must be associated with diagnostic imaging [30], history and physical examination [31]. Moreover, the sensitivity of serum CA 15-3 levels for the detection of tumour recurrence was fairly low in the present series with a false-negative rate of 26%.
This pilot study has several limitations, as patients may have received different endocrine therapies, although the majority of patients (73%) were treated with aromatase inhibitors. This diversity in treatment modalities could be related to the previously administered adjuvant therapies. Moreover, this prospective population included a limited number of patients with heterogeneous situations including patients with metastatic disease at either initial diagnosis or relapse. ER positivity was not systematically confirmed by pathological analysis of the metastasis, but this is a very common in patients with metastatic breast cancer, provided that imaging is positive, and endocrine therapy is decided only on the ER positivity of the primary tumour. Nevertheless, patients with positive Her2 expression were not included since these patients usually do not respond to endocrine therapy, particularly tamoxifen [32]. The optimal interval between the two PET scans was defined as 8 ± 2 weeks, allowing the two PET scans to be performed during the 12-week interval between the two oncologist visits, but a variation of this time interval was observed (mean ± SD of 10 ± 4 weeks) due to patient convenience and/or oncologist planning. Finally, the PET/CT scan results were known by the oncologists, which may have influenced their decision-making, and the PFS value.
Very few PET studies assessing endocrine therapy are available. The main parameter evaluated is the flare reaction induced after oestradiol challenge. Based on the clinical observation of a flare reaction characterized by bone and soft-tissue pain and cutaneous erythema generally occurring within 7–10 days after induction of endocrine therapy in 5–20% of patients, the metabolic flare reaction, reflected by increased tumour FDG uptake, was studied by the Mallinckrodt Institute of Radiology in St Louis, Missouri. This group showed that this reaction is predictive of the response to endocrine therapy [14, 15]. This group has also developed ER in vivo FES PET imaging using 16α-[18F]fluoroestradiol-17β [33] to characterize the in vivo functional status of ER. FES uptake in metastases on a baseline PET scan and its intensity assessed by SUV were higher in responders than in nonresponders [14, 34, 35]. The decreased FES uptake observed after induction of antioestrogen therapy, due to selective competition and binding of antioestrogen, was greater in responders than in non-responders among 11 metastatic patients [14].
More recently, Dehdashti et al, have demonstrated that FES uptake on baseline PET scan and the flare reaction with FDG after oestradiol challenge may both be predictive of response [36]. The proposed explanation for the increased tumour FDG uptake after oestradiol challenge is an increase in cell growth. A recent study has shed new light on the biofactors that influence cancer cell glucose metabolism [37]. The authors showed that 17β-oestradiol is able to increase 18F-FDG uptake by stimulating glycolysis and hexokinase in oestrogen-responsive breast cancer cells, but this action is not mediated by nuclear ER but via the membrane-initiated rapid PI3K-Akt activation pathway. This observation might illustrate why non-nuclear ER could constitute a target for oestrogen action, with effects on glucose metabolism. The underlying question raised by Linden and Mankoff [35] is, among the currently available biomarkers, which one is the more relevant to predict response to endocrine therapy by molecular imaging: glycolysis (FDG) or proliferation (FLT)? Other radiolabelled agents including 11C-methionine or FLT [38–40] have also been studied to evaluate early response to therapy in advanced breast cancer, but no conclusion can yet be drawn from these preliminary studies.
Conclusion
In this pilot study in a small group of patients with metastatic breast cancer at either initial diagnosis or relapse, FDG PET/CT appeared to be predictive of response to endocrine therapy and reflected patient outcome as assessed in terms of PFS. These findings need to be confirmed in further prospective studies based on a larger number of patients. PET imaging combining FES and FDG is very promising. FES PET performed at baseline could be useful in evaluating whether ERs are present and functional in primary or metastatic lesions, while FDG appears to be predictive of response to endocrine therapy.
References
Beslija S, Bonneterre J, Burstein H, Cocquyt V, Gnant M, Heinemann V, et al.; Central European Cooperative Oncology Group (CECOG). Third consensus on medical treatment of metastatic breast cancer. Ann Oncol. 2009;20:1771–85.
Kuukasjärvi T, Kononen J, Helin H, Holli K, Isola J. Loss of estrogen receptor in recurrent breast cancer is associated with poor response to endocrine therapy. J Clin Oncol. 1996;14:2584–9.
Kaufmann M, von Minckwitz G, Bear H, Buzdar A, McGale P, Bonnefoi H, et al. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: new perspectives 2006. Ann Oncol. 2007;18:1927–34.
Schelling M, Avril N, Nahrig J, Kuhn W, Romer W, Sattler D. Positron emission tomography using [(18)F]fluorodeoxyglucose for monitoring primary chemotherapy in breast cancer. J Clin Oncol. 2000;18:1689–95.
Smith I, Welch A, Hutcheon A, Miller I, Payne S, Chilcott F. Positron emission tomography using [(18)]-(fluorine-18)-fluorodeoxy-D-glucose to predict the pathologic response of breast cancer to primary chemotherapy. J Clin Oncol. 2000;18:1676–88.
Rousseau C, Devillers A, Sagan C, Ferrer L, Bridji B, Campion L, et al. Monitoring of early response to neoadjuvant chemotherapy in stage II and III breast cancer by [18F]fluorodeoxyglucose positron emission tomography. J Clin Oncol. 2006;24:5366–72.
Berriolo-Riedinger A, Touzery C, Riedinger JM, Toubeau M, Coudert B, Arnould L, et al. [18F]FDG-PET predicts complete pathological response of breast cancer to neoadjuvant chemotherapy. Eur J Nucl Med Mol Imaging. 2007;34:1915–24.
McDermott G, Welch A, Staff R, Gilbert F, Schweiger L, Semple S, et al. Monitoring primary breast cancer throughout chemotherapy using FDG-PET. Breast Cancer Res Treat. 2007;102(1):75–84.
Schwarz-Dose J, Untch M, Tiling R, Sassen S, Mahner S, Kahlert S, et al. Monitoring primary systemic therapy of large and locally advanced breast cancer by using sequential positron emission tomography imaging with [18F]fluorodeoxyglucose. J Clin Oncol. 2009;27:535–41.
Duch J, Fuster D, Munoz M, Fernandez PL, Paredes P, Fontanillas M, et al. 18F-FDG PET/CT for early prediction of response to neoadjuvant chemotherapy in breast cancer. Eur J Nucl Med Mol Imaging. 2009;36:1551–7.
Dose Schwarz J, Bader M, Jenicke L, Hemminger G, Jänicke F, Avril N. Early prediction of response to chemotherapy in metastatic breast cancer using sequential 18F-FDG PET. J Nucl Med. 2005;46:1144–50.
Couturier O, Jerusalem G, N’Guyen J, Hustinx R. Sequential positron emission tomography using [18F]fluorodeoxyglucose for monitoring response to chemotherapy in metastatic breast cancer. Clin Cancer Res. 2006;12:6437–43.
Specht J, Tam S, Kurland B, Gralow J, Livingston R, Linden H, et al. Serial 2-[18F] fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) to monitor treatment of bone-dominant metastatic breast cancer predicts time to progression (TTP). Breast Cancer Res Treat. 2007;105:87–94.
Dehdashti F, Flanagan F, Mortimer J, Katzenellenbogen J, Welch M, Siegel B. Positron emission tomographic assessment of “metabolic flare” to predict response of metastatic breast cancer to antiestrogen therapy. Eur J Nucl Med. 1999;26:51–6.
Mortimer J, Dehdashti F, Siegel B, Trinkaus K, Katzenellenbogen J, Welch M. Metabolic flare: indicator of hormone responsiveness in advanced breast cancer. J Clin Oncol. 2001;19:2797–803.
Young H, Baum R, Cremerius U, Herholz K, Hoekstra O, Lammertsma A, et al. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur J Cancer. 1999;35:1773–82.
Kaplan E, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–81.
Hamaoka T, Madewell J, Podoloff D, Hortobagyi G, Ueno N. Bone imaging in metastatic breast cancer. J Clin Oncol. 2004;22:2942–53.
Du Y, Cullum I, Illidge T, Ell P. Fusion of metabolic function and morphology: sequential [18F]fluorodeoxyglucose positron-emission tomography/computed tomography studies yield new insights into the natural history of bone metastases in breast cancer. J Clin Oncol. 2007;25:3440–7.
Tateishi U, Gamez C, Dawood S, Yeung H, Cristofanilli M, Macapinlac H. Bone metastases in patients with metastatic breast cancer: morphologic and metabolic monitoring of systemic therapy with integrated PET/CT. Radiology. 2008;247:189–96.
Schneider-Kolsky M, Hart S, Fox J, Midolo P, Stuckey J, Hofman M, et al. The role of chemotherapeutic drugs in the evaluation of breast tumour response to chemotherapy using serial FDG-PET. Breast Cancer Res. 2010;12:R37.
Ueda S, Tsuda H, Saeki T, Omata J, Osaki A, Shigekawa T, et al. Early metabolic response to neoadjuvant letrozole, measured by FDG PET/CT, is correlated with a decrease in the Ki67 labeling index in patients with hormone receptor-positive primary breast cancer: a pilot study. Breast Cancer. 2010;16:660–2.
Bos R, van Der Hoeven J, van Der Wall E, van Der Groep P, van Diest P, Comans E, et al. Biologic correlates of (18)fluorodeoxyglucose uptake in human breast cancer measured by positron emission tomography. J Clin Oncol. 2002;15:379–87.
Buck A, Schirrmeister H, Kuhn T, Shen C, Kalker T, Kotzerke J, et al. FDG uptake in breast cancer: correlation with biological and clinical prognostic parameters. Eur J Nucl Med Mol Imaging. 2002;29:1317–23.
Shimoda W, Hayashi M, Murakami K, Oyama T, Sunagawa M. The relationship between FDG uptake in PET scans and biological behavior in breast cancer. Breast Cancer. 2007;14:260–8.
Smith I, Dowsett M, Ebbs S, Dixon J, Skene A, Blohmer J, et al. Neoadjuvant treatment of postmenopausal breast cancer with anastrozole, tamoxifen, or both in combination: the Immediate Preoperative Anastrozole, Tamoxifen, or Combined with Tamoxifen (IMPACT) multicenter double-blind randomized trial. J Clin Oncol. 2005;23:5108–16.
Dowsett M, Smith I, Ebbs S, Dixon J, Skene A, Griffith C, et al. Proliferation and apoptosis as markers of benefit in neoadjuvant endocrine therapy of breast cancer. Clin Cancer Res. 2006;12:1024s–30s.
Dowsett M, Smith I, Ebbs S, Dixon J, Skene A, A’Hern R, et al. Prognostic value of Ki67 expression after short-term presurgical endocrine therapy for primary breast cancer. J Natl Cancer Inst. 2007;99:167–70.
Huyge V, Garcia C, Alexiou J, Ameye L, Vanderlinden B, Lemort M, et al. Heterogeneity of metabolic response to systemic therapy in metastatic breast cancer patients. Clin Oncol (R Coll Radiol). 2010;22:818–27.
Champion L, Brain E, Giraudet A, Le Stanc E, Wartski M, Edeline V, et al. Breast cancer recurrence diagnosis suspected on tumor marker rising: value of whole-body 18FDG-PET/CT imaging and impact on patient management. Cancer. 2011;117:1621–9.
Harris L, Fritsche H, Mennel R, Norton L, Ravdin P, Taube S, et al; American Society of Clinical Oncology. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J Clin Oncol. 2007;25:5287–312.
Ellis M, Coop A, Singh B, Mauriac L, Llombert-Cussac A, Jänicke F, et al. Letrozole is more effective neoadjuvant endocrine therapy than tamoxifen for ErbB-1- and/or ErbB-2-positive, estrogen receptor-positive primary breast cancer: evidence from a phase III randomized trial. J Clin Oncol. 2001;19:3808–16.
Mintun M, Welch M, Siegel B, Mathias C, Brodack J, McGuire A, et al. Breast cancer: PET imaging of estrogen receptors. Radiology. 1988;169:45–8.
McGuire A, Dehdashti F, Siegel B, Lyss A, Brodack J, Mathias C, et al. Positron tomographic assessment of 16a-[18F]fluoro-17b-estradiol uptake in metastatic breast carcinoma. J Nucl Med. 1991;32:1526–31.
Linden H, Stekhova S, Link J, Gralow J, Livingston R, Ellis G, et al. Quantitative fluoroestradiol positron emission tomography imaging predicts response to endocrine treatment in breast cancer. J Clin Oncol. 2006;24:2793–9.
Dehdashti F, Mortimer J, Trinkaus K, Naughton M, Ellis M, Katzenellenbogen J, et al. PET-based estradiol challenge as a predictive biomarker of response to endocrine therapy in women with estrogen-receptor-positive breast cancer. Breast Cancer Res Treat. 2009;113:509–17.
Ko B, Paik J, Jung K, Lee K. 17b-Estradiol augments 18F-FDG uptake and glycolysis of T47D breast cancer cells via membrane-initiated rapid PI3K-Akt activation. J Nucl Med. 2010;51:1740–7.
Pio BS, Park CK, Pietras R, Hsueh WA, Satyamurthy N, Pegram MD, et al. Usefulness of 3′-[F-18]fluoro-3′-deoxythymidine with positron emission tomography in predicting breast cancer response to therapy. Mol Imaging Biol. 2006;8:36–42.
Kenny L, Coombes RC, Vigushin DM, Al-Nahhas A, Shousha S, Aboagye EO. Imaging early changes in proliferation at 1 week post chemotherapy: a pilot study in breast cancer patients with 3′-deoxy-3′-[(18)F]fluorothymidine positron emission tomography. Eur J Nucl Med Mol Imaging. 2007;34:1339–47.
Lindholm P, Lapela M, Någren K, Lehikoinen P, Minn H, Jyrkkiö S. Preliminary study of carbon-11 methionine PET in the evaluation of early response to therapy in advanced breast cancer. Nucl Med Commun. 2009;30:30–6.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
A related editorial commentary can be found at doi:10.1007/s00259-011-2018-3.
Rights and permissions
About this article
Cite this article
Mortazavi-Jehanno, N., Giraudet, AL., Champion, L. et al. Assessment of response to endocrine therapy using FDG PET/CT in metastatic breast cancer: a pilot study. Eur J Nucl Med Mol Imaging 39, 450–460 (2012). https://doi.org/10.1007/s00259-011-1981-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-011-1981-z