
Abstract
Purpose
Subtle cognitive impairment is recognized in the first stages of Parkinson’s disease (PD), including executive, memory and visuospatial dysfunction, but its pathophysiological basis is still debated.
Methods
Twenty-six consecutive, drug-naïve, de novo PD patients underwent an extended neuropsychological battery, dopamine transporter (DAT) and brain perfusion single photon emission computed tomography (SPECT). We previously reported that nigrocaudate impairment correlates with executive functions, and nigroputaminal impairment with visuospatial abilities. Here perfusion SPECT was first compared between the PD group and age-matched controls (CTR). Then, perfusion SPECT was correlated with both DAT SPECT and four neuropsychological factors by means of voxel-based analysis (SPM8) with a height threshold of p < 0.005 at peak level and p < 0.05 false discovery rate-corrected at cluster level. Both perfusion and DAT SPECT images were flipped in order to have the more affected hemisphere (MAH), defined clinically, on the same side.
Results
Significant hypoperfusion was found in an occipital area of the MAH in PD patients as compared to CTR. Executive functions directly correlated with brain perfusion in bilateral posterior cingulate cortex and precuneus in the less affected hemisphere (LAH), while verbal memory directly correlated with perfusion in the precuneus, inferior parietal lobule and superior temporal gyrus in the LAH. Furthermore, positive correlation was highlighted between nigrocaudate and nigroputaminal impairment and brain perfusion in the precuneus, posterior cingulate and parahippocampal gyri of the LAH.
Conclusion
These data support the evidence showing an early involvement of the cholinergic system in the early cognitive dysfunction and point to a more relevant role of parietal lobes and posterior cingulate in executive functions in PD.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Cognitive impairment, mainly in the form of executive, visuospatial and memory deficit, has been increasingly recognized in patients with Parkinson’s disease (PD) since the first stages. A mild cognitive impairment has been reported in 20–57% of cases 3–5 years after the diagnosis, which has been suggested as a powerful predictor of the progression of cognitive dysfunction to dementia [1].
However, the neurochemical and pathophysiological basis of these deficits is still not fully elucidated and could be heterogeneous [1]. The early dysexecutive syndrome is similar to that seen in patients with frontal lobe lesions, which has contributed to the concept of PD as a frontostriatal syndrome, mainly based on dopamine deficit at the striatal level and on dorsal striatum-frontal connection impairment. Previous studies have shown a direct correlation between nigrostriatal (mainly nigrocaudate) dopaminergic activity and scores on tests assessing executive functions [2–4], but the relationships among nigrostriatal impairment, cognition and cortical function are not well elucidated and further research is underway.
By means of [18F]fluorodeoxyglucose positron emission tomography (FDG PET), a PD-related cognitive pattern (PDCP) has been identified, directly co-varying with cognitive measures of executive, memory and visuospatial functions [5, 6]. The cortical areas involved in PDCP are mainly located in the frontal and parietal association cortex, with the precuneus and superior frontal gyrus reaching the highest statistical significance [7, 8]. While relevant in the modelling of PD pathophysiology, the PDCP may be less useful to unveil the cortical correlates of specific cognitive domains, because it correlates with a variety of tests.
Also, it is still uncertain to what extent the severity of dopaminergic striatal denervation is associated with impaired cortical perfusion/metabolism. A PD motor-related metabolic pattern (PDRP) has been described, mostly independent of PDCP, in which increased metabolic levels in pallidothalamic, pontocerebellar and motor cortical/supplementary motor area metabolic activity, associated with reductions in the lateral premotor and posterior parietal areas, correlate with dopamine transporter (DAT) binding. Instead, DAT binding is not correlated with the cortical areas contributing to the PDCP [9]. However, not all of the studies support this model. In a single photon emission computed tomography (SPECT) study, while DAT binding in the left putamen was correlated with perfusion in the left premotor cortex and supplementary motor area, thus confirming the PDRP-DAT relationships, DAT binding in the left caudate was correlated with perfusion in the left dorsolateral prefrontal cortex, which is actually part of the PDCP, not of the PDRP [10]. Similar results were obtained in a study in drug-naïve PD patients, in whom nigroputaminal dopaminergic activity was correlated with glucose metabolism in premotor as well as in multiple areas of the frontal association cortex [11]. In another study the findings seemed to be even more discordant, since the dopaminergic impairment in the basal ganglia was associated with decreased FDG uptake in the cerebellum and thalamus, and with increased FDG uptake in the motor cortex. In the same study, the univariate voxel-based correlation analysis between 18F-dopa PET and 18F-FDG PET failed to show significant results [12].
The aim of this study was to investigate the relationships among nigrostriatal denervation, cognitive performances and cortical function in a group of de novo, drug-naïve PD patients, by means of an extended battery of neuropsychological tests and both brain perfusion and DAT SPECT.
Materials and methods
Patients
Thirty consecutive patients with de novo PD, never treated with dopaminergic stimulation (drug-naïve), were enrolled. The diagnosis of PD followed current criteria [13]. The patients underwent brain magnetic resonance imaging (MRI), or computed tomography (CT) if MRI was unfeasible, to rule out other brain diseases. Patients with brain infarcts on MRI/CT or with a history of stroke or transient ischaemic attacks were excluded, whereas the presence of small white matter hyperintensities on MRI was not an exclusion criterion. Dementia was excluded by means of clinical interview and questionnaires for activities of daily living (ADL)[14] and instrumental ADL [15]. The Clinical Dementia Rating (CDR) Scale was 0 in all patients. The Mini-Mental State Examination (MMSE) was used as a measure of global cognitive function. The 15-item Geriatric Depression Scale was administered to assess depression. Motor severity of disease was assessed by the Unified Parkinson’s Disease Rating Scale (UPDRS) (Motor section).
Patients underwent a neuropsychological test battery, including: (1) 6-trial selective reminding test (SRT) for verbal episodic memory (immediate and delayed recall); (2) categorical and phonological verbal fluency; (3) figure copying of the mental deterioration battery (simple copy and copy with guiding landmarks) to assess visuoconstructional abilities; (4) Raven’s PM47 matrices, investigating logical reasoning and visuospatial functions; (5) visual search test to study sustained attention and ideomotor speed; (6) trail making test (A and B, with computation of B-A score) to explore visuomotor abilities, divided attention and attention shifting; (7) Stroop colour-word test for cognitive flexibility and executive functions; (8) symbol digit test to assess executive functions and working memory; (9) Corsi’s block design to investigate spatial memory; (10) digit span (forward) assessing auditory memory span; and (11) clock completion test as a mixed measure of executive functions, visuospatial abilities and memory. References for tests and normative values are listed in a previous paper [4].
White matter hyperintensities (WMH) were scored on T2-weighted images using the Age-Related White Matter Changes (ARWMC) Scale [16], which assigns a rating on a 4-point scale (0, no lesions; 1, focal lesions; 2, increasing confluence; 3, diffuse involvement) in each of five regions in both hemispheres separately (frontal, parieto-occipital, temporal, infratentorial and basal ganglia). The MRI of 21 patients and 17 controls were blindly assessed by one of us (D.A.). In five patients and four controls CT was assessed since MRI was not available.
The 30 patients underwent brain DAT SPECT, while in 4 of them brain perfusion SPECT was not feasible because of logistic reasons. Therefore, the final study group included 26 of the original 30 patients. The main clinical and demographic characteristics are listed in Table 1.
Controls
A group of 21 normal subjects in the same age span as patients served as controls for brain perfusion SPECT comparison with PD patients. Control subjects were healthy volunteers, recruited during Open University programmes for the elderly. Their healthy condition was carefully checked by reviewing their general medical history and clinical examination. MMSE was performed and only subjects with a score ≥ 28 were considered. Moreover, only subjects with a CDR of 0 were included. Control subjects also underwent brain MRI (all but 4 who underwent CT because of metallic devices, n = 2, or claustrophobia, n = 2).
The study protocol met the approval of the local Ethics Committee and an informed consent form was signed by all participants, in compliance with the Helsinki Declaration of 1975.
Brain [123I]FP-CIT SPECT and [99mTc]bicisate (ECD) SPECT
DAT SPECT was acquired after i.v. administration of about 185 MBq of [123I]FP-CIT (DaTSCAN, GE Healthcare, Little Chalfont, Buckinghamshire, UK). Patients also underwent brain perfusion SPECT after i.v. administration of about 740 MBq of [99mTc]bicisate (ECD) (Neurolite, Bristol-Myers Squibb, Moreton, UK) within 1 month. Both procedures were performed according to the European Association of Nuclear Medicine (EANM) guidelines [17, 18].
SPECT was performed using a dual-head Millennium VG camera (GE Healthcare) equipped with low-energy, high-resolution, parallel-beam collimators. Acquisition started between 180 and 240 min after injection of [123I]FP-CIT and lasted 40 min, while it started after 30–60 min after injection of [99mTc]bicisate (ECD) and lasted 30 min. A “step-and-shoot” protocol was applied with a radius of rotation <15 cm, and 120 projections evenly spaced over 360° were generated. Total counts ranged between 2.5 and 3 million ([123I]FP-CIT) or were higher than 5 million ([99mTc]bicisate). The pixel size of the acquisition matrix was 2.4 mm, thanks to an electronic zoom (zoom factor = 1.8) applied in the data collection phase. In the reconstruction phase also a digital zoom was used and the resulting images were sampled by cubic voxels with 2.33-mm sides. Projections were processed by means of the ordered subsets expectation maximization (OSEM) algorithm (8 iterations, 10 subsets) [19] followed by post-filtering (3-D Gaussian filter with full-width at half-maximum 5 8 mm). The OSEM algorithm included a proback pair accounting for collimator blur and photon attenuation. No compensation for scatter was performed. The 2-D + 1 approximation [20] was applied in the simulation of the space-variant collimator blur, whereas photon attenuation was modelled with the approximation of a linear coefficient uniform inside the skull and equal to 0.11 cm−1.
The reconstructed [123I]FP-CIT images were exported in analyse format and processed by the automatic BasGan algorithm [21] based on a high-definition, three-dimensional (3-D) striatal template, derived from Talairach’s atlas. An optimization protocol automatically performs fine adjustments in the positioning of blurred templates to best match the radioactive counts and locates occipital regions of interest for background evaluation. Partial volume effect (PVE) correction is included in the process of uptake computation of the caudate, putamen and background. Background uptake was subtracted by putamen and caudate uptake as follows [(caudate or putamen uptake−background uptake)/background uptake].
The reconstructed [99mTc]ECD images were exported in analyse format and processed by the Statistical Parametric Mapping (SPM) 8 software.
In order to highlight correlation in the more and in the less affected hemispheres, respectively, the more affected hemisphere (MAH) was defined as the contralateral one to the side of the body with prevalence of motor symptoms, such as tremor, rigidity or motor impairment, by the referring clinician. A UPDRS asymmetry index was computed following the procedure described in Yogev et al. [22] (Table 1). In 16 patients the MAH was the left one, while in the remaining 10 patients it was the right one. Thus, both DAT and perfusion SPECT were flipped in these ten patients so as to have the MAH on the left side and the less affected hemisphere (LAH) in the right side, following the procedure adopted in previous works [4, 12]. In this way we favoured highlighting findings caused by the disease process while missing the information of left/right hemisphere peculiarities.
As for putamen uptake, correspondence between clinical and DAT SPECT MAH was found in 19 of 26 patients, while in 4 of 26 patients the uptake was the same in the two sides and just in 3 of 26 was the asymmetry reversed in comparison to the clinical side (mean reversed putamen asymmetry: 10.3%). Bilateral uptake reduction was present in the four patients with symmetric putamen uptake as well as in the three patients with reversed asymmetry. As for caudate uptake, correspondence between clinical and DAT SPECT MAH was found in 18 of 26 patients, while in 1 of 26 patients the uptake was the same in the two sides and in 7 of 26 the asymmetry was reversed in comparison to the clinical side (mean reversed putamen asymmetry: 8.1%). The presence of both reversed putamen and reversed caudate asymmetries was never found in an individual patient, so that each patient had at least one of the two nuclei uptake asymmetry concordant with the clinical asymmetry. The UPDRS asymmetry index was positively correlated (r = 0.41; p < 0.05) with DAT putamen asymmetries but not with DAT caudate asymmetries (computed as LAH−MAH/mean of LAH + MAH).
Statistics
Because of the problem of multicollinearity among the 16 neuropsychological variables, preliminary analyses were performed on the original variables to minimize multicollinearity and to reduce the number of variables for further statistical analysis. As a first step, factor analysis with varimax rotation was applied to the 16 native neuropsychological measures at baseline to identify those scores expressing a similar part of total variance. Factor analysis identified four cognitive factors, as detailed in a previous paper [4], including a dysexecutive (NPS-EX), a visuospatial (NPS-VS), a verbal memory (NPS-VM) and a ‘mixed’ (NPS-MIX) factor. A conventional threshold of 0.4 was applied to factor loadings (expressing the factor-variable correlation) to individuate the group of variables mainly represented by each factor.
Using SPM8 (Wellcome Department of Cognitive Neurology, London, UK) implemented in MATLAB 6.5 (MathWorks, Natick, MA, USA), perfusion SPECT data were subjected to affine and nonlinear spatial normalization into the MNI space, using a 99mTc-bicisate customized template [23]. The spatially normalized set of images were then smoothed with a 12-mm isotropic Gaussian filter to blur individual variations in gyral anatomy and to increase the signal to noise ratio. The resulting statistical parametric maps, SPM{t}, were transformed into normal distribution (SPM{z}) unit.
Correction of SPM coordinates to match the Talairach coordinates was achieved by the subroutine implemented by Matthew Brett (http://www.mrc-cbu.cam.ac.uk/Imaging). SPM t-maps were thresholded using a p < 0.005 at voxel level, uncorrected for multiple comparisons. This threshold is accepted as a reasonable choice as it takes into account the need to balance between type I and type II errors and considers the relatively low sensitivity of SPECT in the lack of repeated measures [24, 25]. The significance of identified regions was established at a p < 0.05, corrected for multiple comparisons with the false discovery rate (FDR) option at the cluster level. Only clusters containing more than 50 voxels were considered to be significant.
The following analyses were assessed using SPM8, taking into account age, gender and education as ‘nuisance’ variables:
-
1.
Comparison
-
Controls minus PD patients
-
-
2.
Correlations
-
Brain perfusion and each of the four neuropsychological factors
-
Brain perfusion and FP-CIT uptake at the caudate and putamen level in the MAH as well as in the LAH
-
Results
Comparison: controls minus PD patients
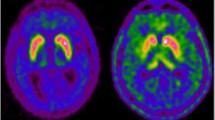
A cluster of significant hypoperfusion was found in the occipital lobe of the MAH, including the middle occipital gyrus (Brodmann areas, BA, 18 and 19) and the lingual gyrus (Table 2, Fig. 1).

Statistical parametric maps superimposed to magnetic resonance rendering showing the regions of significant decrease in brain perfusion in PD patients compared with controls, obtained by SPM8 analysis. Details of regions and coordinates in Table 2
Correlations: brain perfusion and neuropsychological factors
A positive correlation between brain perfusion and NPS-EX was found in a large cluster in the parieto-occipital areas of both hemispheres, with peaks in the posterior cingulate cortex (PCC; BA30) of both hemispheres and parietal precuneus (BA7) of the LAH (Table 2, Fig. 2). The correlation in the posterior cingulate gyrus of the LAH survived the p < 0.001 threshold at peak level. A cluster of positive correlation was also found between brain perfusion and NPS-VM in the temporoparietal region of the LAH, involving the superior temporal gyrus (BA13), the inferior parietal lobule (BA40) and the parietal precuneus (BA7). The correlation in BA13 and BA40 survived the p < 0.001 threshold at peak level. No significant correlation was found between perfusion and either NPS-VS or NPS-MIX.

Statistical parametric maps superimposed to magnetic resonance rendering showing the regions of significant correlation between brain perfusion and NPS-EX (neuropsychological executive factor) in PD patients, obtained by SPM8 analysis. Details of regions and coordinates in Table 2
Correlations: brain perfusion and FP-CIT uptake
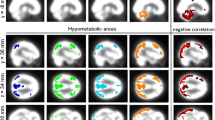
A positive correlation was found between brain perfusion in the PCC (BA30), parahippocampal gyrus (BA30) and middle temporal gyrus (BA39) of the LAH and FP-CIT uptake in the caudate of the LAH (Table 2, Fig. 3). A positive correlation was also found between brain perfusion in the PCC (BA30), parietal precuneus (BA7) and occipital cuneus (BA18) of the LAH and putamen uptake in the MAH.

Statistical parametric maps superimposed to magnetic resonance rendering showing the regions of significant correlation between brain perfusion and FP-CIT caudate uptake in the less affected hemisphere in PD patients, obtained by SPM8 analysis. Details of regions and coordinates in Table 2
Discussion
This study shows that executive functions are directly correlated with cortical function, as assessed by means of perfusion SPECT, in the posterior association and limbic cortex with peaks in the PCC and parietal precuneus. These areas are included in the PDCP that is correlated with measures of executive function indeed, but also includes association areas of the frontal lobe. The latter may have been expected to show a higher correlation with executive functions than the parietal-posterior limbic areas. However, the classic notion of executive dysfunction as a consequence of frontal-subcortical disconnection, mainly derived from patients with cerebrovascular disease, has not received further validation by more recent neuroimaging studies. In a large series of non-demented elderly individuals, WMH in all but occipital lobes were correlated with executive dysfunction; thus, not just those located in the frontal lobes [26]. In another larger sample of subjects with mild cognitive impairment (MCI), WMH in the parietal lobe, but not in the frontal lobe, were necessary to cause executive dysfunction [27]. A similar scenario may characterize executive dysfunction of PD. A SPECT study highlighted hypoperfusion in the inferior parietal lobule and supramarginal gyrus, rather than in the frontal lobes, in PD patients with dysexecutive impairment, assessed with the Frontal Assessment Battery [28]. Furthermore, there was significant fractional anisotropy reduction in the left parietal—not frontal—white matter in non-demented PD patients with a low score on the Wisconsin Card Sorting Test as compared to those with a higher score [29]. These findings in patients with cerebrovascular disease and in PD patients parallel those obtained in healthy individuals [30] and suggest that executive functions are more distributed across several cortical regions, including the parietal association cortex.
Verbal memory disclosed a significant correlation with cortical function in an association temporoparietal region of the LAH, including again the precuneus, the inferior parietal lobule and the superior temporal gyrus. This is in agreement with previous correlative studies in other neurodegenerative disorders, such as Alzheimer’s disease (AD), in which correlation between a word list learning and brain perfusion in bilateral temporal lobes and left precuneus was found [31]. These findings point to the involvement of the wider memory network component of verbal memory function. In a correlative analysis in mild AD patients, the score on a verbal memory test was found to correlate with glucose metabolism in bilateral PCC and precuneus, middle occipital and inferior parietal gyri in the right hemisphere [32]. The key role of the precuneus in the memorization of imageable words has been confirmed by activation studies in normal subjects during the recall of episodic information [33] or during mental imagery processes [34, 35]. In PD patients with amnestic MCI, we previously reported significant hypoperfusion in bilateral parieto-occipital cortex, also including the PCC, in comparison with controls but even in comparison with patients with the common form of amnestic MCI [36].
Thus, both executive and verbal memory function correlated with brain perfusion in posterior association cortical areas, with some topographical overlap (precuneus) and some differences. These findings do not fit with the concept of PD as a frontostriatal syndrome, mainly based on dorsal striatum-frontal connection impairment. Rather, they point to the impairment of posterior brain areas, where dopamine endings are much less present. Increasing evidence with N-[11C]methyl-4-piperidyl acetate (MP4A) PET shows a reduction of cholinergic function mainly in posterior brain regions, including the PCC and posterior temporo-parieto-occipital association cortex, in PD patients without dementia [37] but even in de novo or early PD patients [38]. There is an intriguing topographic correspondence in posterior association areas between cortical dysfunction, as shown by means of FDG PET [39–41] or perfusion SPECT [8, 36], and cholinergic denervation in PD. It has been shown that the cholinergic deficit in posterior association areas is even more severe in PD patients without dementia than in patients with AD [42]. According to this view, the early cholinergic deficit in PD might account for executive dysfunction more than previously thought, as supported by early studies showing that in PD patients anticholinergic drugs produce a frontal-like executive dysfunction after acute administration [43] and by the findings that performance on tests of attention and executive function correlated with loss of cortical cholinesterase activity in PD dementia [44].
We found a positive correlation between nigrostriatal denervation and cortical perfusion in posterior temporo-parieto-occipital areas of the LAH, most of which are included in the PDRP as shown by both FDG PET [11] and [99mTc]ECD SPECT studies [45]. Our results seem in keeping with the finding of a positive correlation trend between [18F]fluorodopa uptake in the basal ganglia and glucose metabolism in the temporal and insular cortex of the LAH by univariate analysis [12]. Substantial evidence links the components of PDRP to the motor symptoms of PD, because it is correlated with measures of motor disability [46] as well as with spontaneous firing rates of pallidal neurons [47]. PDRP expression increases linearly with disease progression and is correlated with concurrent reductions in motor function and DAT binding in the putamen [48]. Although the anatomo-functional bases for the PDRP are not well known, the association of PDRP expression with DAT binding in the striatum [9] and its modulation by levodopa [46] suggests that, functionally, this network may be affected by dopamine. However, although loss of nigrostriatal dopamine cells can be seen as permissive for expression of the PDRP, network activity seems to be more closely related to basal ganglia output, which are not dopaminergic, and in fact includes areas in parietal and occipital lobes where dopamine endings are rare. Moreover, a recent study with functional MRI (fMRI) has extended previous observations on the functional connectivity pattern of the striatum. Besides the frontal association cortex, connectivity of the caudate includes the parahippocampal gyrus, the inferior temporal gyrus and the inferior parietal cortex both in PD patients and controls, while connectivity of the putamen includes the superior temporal gyrus, the inferior parietal cortex, the middle cingulate cortex and the middle occipital gyrus besides the classic connections with motor and premotor areas. Of note, in PD patients there was increased functional connectivity between the anterior putamen and parietal operculum, supramarginal gyrus, insula and inferior temporal gyrus as compared to controls [49].
As a final remark, looking at Table 2 it appears that the region of the PCC-precuneus was almost invariably positively correlated with executive function, verbal memory function and nigrostriatal dopamine impairment. The PCC-precuneus is the main posterior key node of the so-called default mode network, thought to express hyperactivity of interlinked regions during brain at rest. Activity in the dorsal caudate has been shown to correlate with the PCC-precuneus, and it has been suggested that default network activity in these nodes is abnormally modulated in diseases in which the dopamine system is implicated. A relationship between striatal dopamine synthesis and resting state fMRI activity in the PCC-precuneus has been shown that may be facilitated by the closed loop dorsal caudate-pallidal-thalamic-cortical connectivity, including both lateral prefrontal cortex and precuneus [50].
Correlations between brain perfusion in the LAH and nigrostriatal impairment were found at the nigrocaudate level in the LAH and at the nigroputaminal level in the MAH. This side discrepancy may well be the result of chance. However, the PDRP has been recently evaluated in the LAH in the attempt to assess cortical metabolism in a pre-symptomatic hemisphere. The PDRP correlates with nigrostriatal denervation, is already expressed in the LAH at the time of clinical diagnosis, and it has been shown to be detectable at least 2 years before the onset of symptoms in the unaffected side of the body [51].
A limitation of this study is that the mean age at onset of PD (66.6 by looking at age and disease duration in Table 1) was a bit higher than in the general PD population. This bias could be the result of chance, since no criteria other than consecutive enrolment were adopted. Also, living in a very old urban area might have affected recruitment. Although age has been taken into account as a confounding variable in SPM comparison and correlation analyses, which has smoothed the effect of age on results, the present data may not be applicable to the younger general PD population. It could also be argued that WMH have an impact on cognition in PD patients. However, WMH did not significantly differ between the PD group and controls (Table 1). Moreover, whereas the number of WMH has been shown to be higher in PD patients developing dementia [52, 53], they have not been shown to significantly impact cognition in early PD [54, 55].
In conclusion, we have shown that executive and verbal memory function as well as nigrostriatal impairment are correlated with areas of posterior association and limbic cortex in de novo, drug-naïve PD patients. These findings suggest a larger cortical involvement since the time of diagnosis than admitted by the classic striato-frontal hypothesis. Their role in predicting cognitive decline and eventually dementia remains to be verified in longitudinal studies.
References
Kehagia AA, Barker RA, Robbins TW. Neuropsychological and clinical heterogeneity of cognitive impairment and dementia in patients with Parkinson’s disease. Lancet Neurol 2010;9:1200–13.
Rinne JO, Portin R, Ruottinen H, Nurmi E, Bergman J, Haaparanta M, et al. Cognitive impairment and the brain dopaminergic system in Parkinson’s disease: [18F]fluorodopa positron emission tomographic study. Arch Neurol 2000;57:470–5.
Müller U, Wächter T, Barthel H, Reuter M, von Cramon DY. Striatal [123I]beta-CIT SPECT and prefrontal cognitive functions in Parkinson’s disease. J Neural Transm 2000;107:303–19.
Nobili F, Campus C, Arnaldi D, De Carli F, Cabassi G, Brugnolo A, et al. Cognitive-nigrostriatal relationships in de novo, drug-naïve Parkinson’s disease patients: a [I-123]FP-CIT SPECT study. Mov Disord 2010;25:35–43.
Huang C, Mattis P, Tang C, Perrine K, Carbon M, Eidelberg D. Metabolic brain networks associated with cognitive function in Parkinson’s disease. Neuroimage 2007;34:714–23.
Huang C, Mattis P, Perrine K, Brown N, Dhawan V, Eidelberg D. Metabolic abnormalities associated with mild cognitive impairment in Parkinson disease. Neurology 2008;70:1470–7.
Van Laere K, Santens P, Bosman T, De Reuck J, Mortelmans L, Dierckx R. Statistical parametric mapping of (99m)Tc-ECD SPECT in idiopathic Parkinson’s disease and multiple system atrophy with predominant parkinsonian features: correlation with clinical parameters. J Nucl Med 2004;45:933–42.
Firbank MJ, Colloby SJ, Burn DJ, McKeith IG, O’Brien JT. Regional cerebral blood flow in Parkinson’s disease with and without dementia. Neuroimage 2003;20:1309–19.
Huang C, Tang C, Feigin A, Lesser M, Ma Y, Pourfar M, et al. Changes in network activity with the progression of Parkinson’s disease. Brain 2007;130:1834–46.
Paschali A, Messinis L, Kargiotis O, Lakiotis V, Kefalopoulou Z, Constantoyannis C, et al. SPECT neuroimaging and neuropsychological functions in different stages of Parkinson’s disease. Eur J Nucl Med Mol Imaging 2010;37:1128–40.
Berti V, Polito C, Ramat S, Vanzi E, De Cristofaro MT, Pellicanò G, et al. Brain metabolic correlates of dopaminergic degeneration in de novo idiopathic Parkinson’s disease. Eur J Nucl Med Mol Imaging 2010;37:537–44.
Kaasinen V, Maguire RP, Hundemer HP, Leenders KL. Corticostriatal covariance patterns of 6-[18F]fluoro-L-dopa and [18F]fluorodeoxyglucose PET in Parkinson’s disease. J Neurol 2006;253:340–8.
Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol 1999;56:33–9.
Katz S, Downs TD, Cash HR, Grotz RC. Progress in development of the index of ADL. Gerontologist 1970;10:20–30.
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 1969;9:179–86.
Wahlund LO, Barkhof F, Fazekas F, Bronge L, Augustin M, Sjögren M, et al. A new rating scale for age-related white matter changes applicable to MRI and CT. Stroke 2001;32:1318–22.
Tatsch K, Asenbaum S, Bartenstein P, Catafau A, Halldin C, Pilowsky LS, et al. European Association of Nuclear Medicine procedure guidelines for brain neurotransmission SPET using (123)I-labelled dopamine D(2) transporter ligands. Eur J Nucl Med Mol Imaging 2002;29:BP30–5.
Tatsch K, Asenbaum S, Bartenstein P, Catafau A, Halldin C, Pilowsky LS, et al. European Association of Nuclear Medicine procedure guidelines for brain perfusion SPET using (99m)Tc-labelled radiopharmaceuticals. Eur J Nucl Med Mol Imaging 2002;29:BP36–42.
Hudson HM, Larkin RS. Accelerated image reconstruction using ordered subsets of projection data. IEEE Trans Med Imaging 1994;13:601–9.
Boccacci P, Bonetto P, Calvini P, Formiconi AR. A simple model for the efficient correction of collimator blur in 3D SPECT imaging. Inverse Problems 1999;15:907–30.
Calvini P, Rodriguez G, Inguglia F, Mignone A, Guerra UP, Nobili F. The basal ganglia matching tools package for striatal uptake semi-quantification: description and validation. Eur J Nucl Med Mol Imaging 2007;34:1240–53.
Yogev G, Plotnik M, Peretz C, Giladi N, Hausdorff JM. Gait asymmetry in patients with Parkinson’s disease and elderly fallers: when does the bilateral coordination of gait require attention? Exp Brain Res 2007;177:336–46.
Morbelli S, Rodriguez G, Mignone A, Altrinetti V, Brugnolo A, Piccardo A, et al. The need of appropriate brain SPECT templates for SPM comparisons. Q J Nucl Med Mol Imaging 2008;52:89–98.
Oishi N, Udaka F, Kameyama M, Sawamoto N, Hashikawa K, Fukuyama H. Regional cerebral blood flow in Parkinson disease with nonpsychotic visual hallucinations. Neurology 2005;65:1708–15.
Villain N, Desgranges B, Viader F, de la Sayette V, Mézenge F, Landeau B, et al. Relationships between hippocampal atrophy, white matter disruption, and gray matter hypometabolism in Alzheimer’s disease. J Neurosci 2008;28:6174–81.
Murray ME, Senjem ML, Petersen RC, Hollman JH, Preboske GM, Weigand SD, et al. Functional impact of white matter hyperintensities in cognitively normal elderly subjects. Arch Neurol 2010;67:1379–85.
Jacobs HI, Visser PJ, Van Boxtel MPJ, Frisoni GB, Tsolaki M, Papapostolou P, et al. The association between white matter hyperintensities and executive decline in mild cognitive impairment is network dependent. Neurobiol Aging 2010 Aug 23. [Epub ahead of print]. PMID: 20739101.
Matsui H, Udaka F, Miyoshi T, Hara N, Tamura A, Oda M, et al. Frontal assessment battery and brain perfusion image in Parkinson’s disease. J Geriatr Psychiatry Neurol 2006;19:41–5.
Matsui H, Nishinaka K, Oda M, Niikawa H, Komatsu K, Kubori T, et al. Wisconsin Card Sorting Test in Parkinson’s disease: diffusion tensor imaging. Acta Neurol Scand 2007;116:108–12.
Collette F, Van der Linden M, Laureys S, Delfiore G, Degueldre C, Luxen A, et al. Exploring the unity and diversity of the neural substrates of executive functioning. Hum Brain Mapp 2005;25:409–23.
Nobili F, Brugnolo A, Calvini P, Copello F, De Leo C, Girtler N, et al. Resting SPECT-neuropsychology correlation in very mild Alzheimer’s disease. Clin Neurophysiol 2005;116:364–75.
Desgranges B, Baron J-C, de la Sayette V, Petit-Taboué M-C, Benali K, Landeau B, et al. The neural substrates of memory systems impairment in Alzheimer’s disease. A PET study of resting brain glucose utilization. Brain 1998;121:611–31.
Cabeza R, Dolcos F, Prince SE, Rice HJ, Weissman DH, Nyberg L. Attention-related activity during episodic memory retrieval: a cross-function fMRI study. Neuropsychologia 2003;41:390–9.
Platel H, Price C, Baron JC, Wise R, Lambert J, Frackowiak RS, et al. The structural components of music perception. A functional anatomical study. Brain 1997;120:229–43.
Fletcher PC, Frith CD, Baker SC, Shallice T, Frackowiak RS, Dolan RJ. The mind’s eye—precuneus activation in memory-related imagery. Neuroimage 1995;2:195–200.
Nobili F, Abbruzzese G, Morbelli S, Marchese R, Girtler N, Dessi B, et al. Amnestic mild cognitive impairment in Parkinson’s disease: a brain perfusion SPECT study. Mov Disord 2009;24:414–21.
Klein JC, Eggers C, Kalbe E, Weisenbach S, Hohmann C, Vollmar S, et al. Neurotransmitter changes in dementia with Lewy bodies and Parkinson disease dementia in vivo. Neurology 2010;74:885–92.
Shimada H, Hirano S, Shinotoh H, Aotsuka A, Sato K, Tanaka N, et al. Mapping of brain acetylcholinesterase alterations in Lewy body disease by PET. Neurology 2009;73:273–8.
Vander Borght T, Minoshima S, Giordani B, Foster NL, Frey KA, Berent S, et al. Cerebral metabolic differences in Parkinson’s and Alzheimer’s diseases matched for dementia severity. J Nucl Med 1997;38:797–802.
Hu MT, Taylor-Robinson SD, Chaudhuri KR, Bell JD, Labbé C, Cunningham VJ, et al. Cortical dysfunction in non-demented Parkinson’s disease patients: a combined (31)P-MRS and (18)FDG-PET study. Brain 2000;123:340–52.
Liepelt I, Reimold M, Maetzler W, Godau J, Reischl G, Gaenslen A, et al. Cortical hypometabolism assessed by a metabolic ratio in Parkinson’s disease primarily reflects cognitive deterioration—[18F]FDG-PET. Mov Disord 2009;24:1504–11.
Bohnen NI, Kaufer DI, Ivanco LS, Lopresti B, Koeppe RA, Davis JG, et al. Cortical cholinergic function is more severely affected in parkinsonian dementia than in Alzheimer disease: an in vivo positron emission tomographic study. Arch Neurol 2003;60:1745–8.
Dubois B, Pilon B, Lhermitte F, Agid Y. Cholinergic deficiency and frontal dysfunction in Parkinson’s disease. Ann Neurol 1990;28:117–21.
Bohnen NI, Kaufer DI, Hendrickson R, Ivanco LS, Lopresti BJ, Constantine GM, et al. Cognitive correlates of cortical cholinergic denervation in Parkinson’s disease and parkinsonian dementia. J Neurol 2006;253:242–7.
Eckert T, Van Laere K, Tang C, Lewis DE, Edwards C, Santens P, et al. Quantification of Parkinson’s disease-related network expression with ECD SPECT. Eur J Nucl Med Mol Imaging 2007;34:496–501.
Asanuma K, Tang C, Ma Y, Dhawan V, Mattis P, Edwards C, et al. Network modulation in the treatment of Parkinson’s disease. Brain 2006;129:2667–78.
Eckert T, Eidelberg D. Neuroimaging and therapeutics in movement disorders. NeuroRx 2005;2:361–71.
Eckert T, Tang C, Eidelberg D. Assessment of the progression of Parkinson’s disease: a metabolic network approach. Lancet Neurol 2007;6:926–32.
Helmich RC, Derikx LC, Bakker M, Scheeringa R, Bloem BR, Toni I. Spatial remapping of cortico-striatal connectivity in Parkinson’s disease. Cereb Cortex 2010;20:1175–86.
Braskie MN, Landau SM, Wilcox CE, Taylor SD, O’Neil JP, Baker SL, et al. Correlations of striatal dopamine synthesis with default network deactivations during working memory in younger adults. Hum Brain Mapp 2011;32:947–61.
Tang CC, Poston KL, Dhawan V, Eidelberg D. Abnormalities in metabolic network activity precede the onset of motor symptoms in Parkinson’s disease. J Neurosci 2010;30:1049–56.
Lee SJ, Kim JS, Yoo JY, Song IU, Kim BS, Jung SL, et al. Influence of white matter hyperintensities on the cognition of patients with Parkinson disease. Alzheimer Dis Assoc Disord 2010;24:227–33.
Beyer MK, Aarsland D, Greve OJ, Larsen JP. Visual rating of white matter hyperintensities in Parkinson’s disease. Mov Disord 2006;21:223–9.
Dalaker TO, Larsen JP, Bergsland N, Beyer MK, Alves G, Dwyer MG, et al. Brain atrophy and white matter hyperintensities in early Parkinson’s disease. Mov Disord 2009;24:2233–41.
Dalaker TO, Larsen JP, Dwyer MG, Aarsland D, Beyer MK, Alves G, et al. White matter hyperintensities do not impact cognitive function in patients with newly diagnosed Parkinson’s disease. Neuroimage 2009;47:2083–9.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nobili, F., Arnaldi, D., Campus, C. et al. Brain perfusion correlates of cognitive and nigrostriatal functions in de novo Parkinson’s disease. Eur J Nucl Med Mol Imaging 38, 2209–2218 (2011). https://doi.org/10.1007/s00259-011-1874-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-011-1874-1