
Abstract
Purpose
In clinical myocardial single photon emission computed tomography (SPECT), attenuation artefacts may cause a loss of specificity in the identification of diseased vessels that can be corrected by means of gated SPECT (GSPECT) acquisition or CT attenuation correction (AC). The purpose of this multicentre study was to assess the impact of GSPECT and AC on the diagnostic performance of myocardial scintigraphy, according to patient’s sex, body mass index (BMI) and site of coronary artery disease (CAD).
Methods
We studied a group of 104 patients who underwent coronary angiography within 1 month before or after the SPECT study. Patients with a BMI > 27 were considered “overweight”. Attenuation-corrected and standard GSPECT early images were randomly interpreted by three readers blinded to the clinical data.
Results
In the whole group, GSPECT and AC showed a diagnostic accuracy of 86.5% (sensitivity 82%, specificity 93%) and 77% (sensitivity 75.4%, specificity 81.4%), respectively (p < 0.05). In women, when anterior ischaemia was matched with CAD, AC failed to show any increase in specificity (AC 63.6% vs GSPECT 63.6%) with evident loss of sensitivity (AC 72.7% vs GSPECT 90.9%). AC significantly improved SPECT specificity in the identification of right CAD in overweight men (AC 100% vs GSPECT 66.7%, p <0.05).
Conclusion
AC improved specificity in the evaluation of right CAD in overweight men. In the other evaluable subgroups specificity was not significantly affected while sensitivity was frequently reduced.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Myocardial perfusion imaging is a fundamental tool for the diagnosis of coronary artery disease (CAD), risk stratification and management decisions for patients with known or suspected CAD and its usefulness is supported by adequate evidence in the literature [1–4].
However, despite considerable technical advances achieved in order to obtain motion and scatter correction, generation of attenuation artefacts leads to a reduction of specificity of conventional single photon emission computed tomography (SPECT) imaging. This limitation has been partially overcome by the application of gated SPECT (GSPECT) that allows the simultaneous evaluation of the perfusion/contraction match, permitting the correct clinical interpretation of fixed (stress/rest) perfusion defects [5].
Alternatively, hardware and software devices have been developed to correct for nonuniform attenuation artefacts [6, 7]. Today the most widely used attenuation correction (AC) instrumentation utilizes single-slice computed X-ray tomography (CT) for acquisition of transmission maps [8]. Several reports on the use of AC in myocardial SPECT imaging showed discordant results and its utility in routine clinical practice is still debated [9–12]. Therefore, the aim of the present study was to evaluate the effect of CT-based AC and of gated acquisition on the interpretation of myocardial SPECT in a multicentre investigation involving patients with known coronary anatomy.
Materials and methods
Population
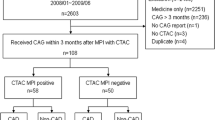
The study population included 104 patients [82 men and 22 women; mean age 64 ± 10; range 38–82; mean body mass index (BMI) 27 ± 4 kg×m−2] referred to 5 Italian nuclear medicine departments from March 2007 to April 2009 for stress/rest GSPECT. All patients had a known coronary anatomy at the time of the study or underwent coronary angiography within 1 month; in particular in patients with known CAD the time elapsed before SPECT was 23 ± 6 days, while in patients with suspected CAD the time to angiography was 20 ± 7 days.
The clinical characteristics and coronary anatomy of the study group are summarized in Table 1.
Given the mean age and the mean BMI of the population we decided to use age-adjusted levels of BMI and to consider as “overweight” all patients with a BMI greater than 27, as previously recommended [13].
Scintigraphic protocol
Each patient underwent stress/rest 99mTc-tetrofosmin GSPECT with CT-based AC according to a single- or double-day early imaging protocol, depending on the needs of the participating units, as previously described [14, 15]; in particular 65 patients (62%) performed a single-day protocol, whereas 39 patients (38%) performed a double-day protocol. Seventy-five patients (72%) underwent an exercise stress test, whereas 29 patients (28%) had a dipyridamole infusion (0.56 mg/kg in 4 min) pharmacologic stress test.
All patients were studied after an overnight fasting period and invited to avoid tea, coffee, chocolate and other foods containing phyllinic derivates at least for 48 h before the stress. Beta-blockers, nitrates and calcium channel blockers were discontinued at least 5 plasma half-lives before the SPECT study while other drugs (such as angiotensin-converting enzyme inhibitors) were maintained.
In cases of previous myocardial infarction, 99mTc-tetrofosmin at rest was injected after nitrate administration (sublingual isosorbide mononitrate, 5 or 10 mg according to body weight).
In the single-day protocol, 99mTc-tetrofosmin (296–370 MBq) was administered intravenously at peak stress. Immediately after the end of the stress, the patient ate a fatty meal to accelerate hepatobiliary clearance of the tracer. Within 15 min, GSPECT with CT-based AC was performed using a hybrid dual-head gamma camera (Infinia Hawkeye; GE) equipped with high-resolution collimators. The protocol included a 64 × 64 matrix, 32 projections, 30-s projection and 16 frames per cycle used in association with a 15% window centred on the 140 keV photopeak of 99mTc. Immediately after completion of the stress study, 740–830 MBq of 99mTc-tetrofosmin was administered under resting conditions and a scan was obtained as for the stress imaging. At the end of each acquisition a low-dose CT scan (140 KV; 2.5 mA) of the chest was performed in order to obtain attenuation maps automatically applied by the processing software to correct the emission data. Reconstructions of stress and rest gated images were performed using filtered backprojection (FBP) using a Butterworth low-pass filter with a critical frequency of 0.46 Nyquist with an order of 5 and with a critical frequency of 0.32 Nyquist with an order of 5, respectively. For application of AC, SPECT emission image data were processed using ordered subsets expectation maximization (OSEM) reconstruction software with 2 iterations and 10 subsets.
Quality controls of alignment both of stress/rest slices and of emission-transmission data were performed for each perfusion study. In all studies GSPECT and AC SPECT sets of images were obtained in the two conditions of acquisition.
In the double-day protocol, 370–600 MBq of 99mTc-tetrofosmin was injected and the stress and rest scans were obtained on separate days.
Analysis of scintigraphic data
Each centre sent raw GSPECT emission data, corrected for nonuniformity, and CT attenuation coefficient maps to the core laboratory (Fondazione G. Monasterio – Pisa) on digital media. Qualitative and semiquantitative analysis of scintigraphic data was performed at the core laboratory using a commercially available GE Xeleris nuclear medicine workstation (GE Medical Systems, Haifa, Israel).
Processed SPECT images were randomly analysed by three experienced readers blinded to the patient’s clinical information, body habitus, type of stress and results of coronary angiography. Patient gender was only revealed on request. Images were displayed on a computer screen in the standard format for display of tomographic cardiac images [16]. The total set of 208 SPECT (104 GSPECT and 104 AC SPECT) was displayed in random order.
Three independent observers visually analysed the image quality using a 4-point scale (from 0 = “poor” to 3 = “optimal”). Since the unavailability of a standard database for AC images did not allow the use of automatic analysis softwares, the presence and extent of perfusion defects and their reversibility were visually evaluated using a 5-point scale (from 0 = “no perfusion defect” to 4 = “total perfusion defect”) according to a 20-segment myocardial model [17] both for GSPECT and for AC SPECT. The readers were aware of the type of image reconstruction (GSPECT or AC SPECT).
Visual summed stress score (SSS), visual summed rest score (SRS) and visual summed difference score (SDS) were then obtained. Functional parameters (motion and thickening) were used to obtain a better differentiation between scarred and attenuated viable segments visualized as fixed perfusion defects in GSPECT.
Coronary angiography
Selective conventional coronary angiography was performed using invasive techniques available in each centre. Standard multiple projections were recorded for the left and right coronary arteries. Coronary angiograms were quantified with offline computer software with an automatic edge contour detection algorithm. In all patients CAD was defined as ≥70% diameter stenosis in the three major coronary arteries and ≥50% for the left main coronary artery.
Statistical analysis
Continuous variables are presented as mean ± SD. Where indicated, differences were assessed by Student’s t test for paired or unpaired data. The significance of the relationship between both GSPECT and AC perfusion data was assessed by linear regression analysis. Analysis of agreement was also performed by means of the Bland-Altman method [18]. Accuracy in coronary stenosis detection was estimated by analysis of receiver-operating characteristic (ROC) curves using MedCalc software (v. 8.0.0.0). As previously described, ROC curves were created by shifting the diagnostic criterion level for positives and negatives over the entire range of score [19]. Sensitivity and 1-specificity for each diagnostic criterion level were plotted against each other. Kappa values <0.4, between 0.4 and 0.75, and > 0.75 were taken to represent poor, fair to good and excellent agreement, respectively [20]. Statistical significance for analysis was assessed at a p value of less than 0.05.
Results
Clinical results
Of the 104 patients, 23 had a BMI greater than 27 (15 men); 56 had a clinical history of previous myocardial infarction; 25 had been previously revascularized with a coronary artery bypass graft; 29 had single-, 25 double- and 9 triple-vessel disease while 41 did not have significant coronary artery stenosis.
Scintigraphic results
Image quality
The quality of stress/rest images was rated as optimal in 22 patients for GSPECT versus 26 for AC SPECT, good in 61 patients for both techniques, fair in 16 patients for GSPECT versus 13 for AC SPECT and poor in 5 patients for GSPECT versus 4 for AC SPECT (p = NS for all values). Artefacts caused by AC, such as truncation [21] or misregistration [22], were not observed in our patients while overcorrection, which may reduce accuracy mostly in the evaluation of septal and anterior walls, was observed in 8.5% of male patients.
Semiquantitative analysis: overall results
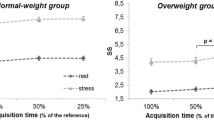
The mean SSS and SRS for GSPECT were significantly higher than the respective values obtained with AC SPECT (SSS 13.12 ± 11.91 vs 11.04 ± 11.52, p < 0.001; SRS 6.97 ± 10.21 vs 5.48 ± 8.67, p < 0.001). These data were confirmed by male subgroup analysis (SSS 14.47 ± 12.47 vs 12.20 ± 12.16, p = 0.001; SRS 7.95 ± 10.82 vs 6.04 ± 9.18, p < 0.001). When only female patients were considered, the differences between the mean values of SSS and SRS were not significant (SSS 8.09 ± 7.88 vs 6.72 ± 7.45, p = NS; SRS 3.31 ± 6.52 vs 3.36 ± 6.18, p = NS).
The mean SDS for GSPECT was slightly but not significantly higher than the mean SDS for AC SPECT (6.15 ± 7.60 vs 5.57 ± 7.22, p = NS). Linear regression analysis showed a fair relationship between GSPECT and AC SPECT SDS (y = 1.249 + 0.702x; r = 0.546; SEE = 0.06; p < 0.001). The Bland-Altman analysis showed a shift in the mean value of the difference (AC SPECT – GSPECT SDS) of −0.6 ± 10.5 [lower limit: −11.1 (95% confidence interval = −12.9 to −9.32); upper limit: +9.9 (95% confidence interval = 8.14 to 11.7)], with 94% of the results enclosed inside the limits (mean ± 1.96 SD) (Fig. 1).

The linear regression analysis showed fair relationship between GSPECT and AC SPECT visual SDS (V-SDS) (a). Bland-Altman analysis showed fair agreement between GSPECT and AC SPECT V-SDS (b)
ROC curve analysis identified cutoffs of 3 for SDS both in GSPECT images and AC SPECT images as the best value for separating patients with from those without CAD. Using these thresholds, GSPECT predicted CAD in 52 of 63 patients (82% sensitivity) and excluded it in 38 of 41 patients (93% specificity), while AC SPECT predicted CAD in 47 of 63 patients with CAD (75.4% sensitivity) and excluded it in 33 of 41 patients without coronary lesions (81.4% specificity). The area under the ROC curve was significantly higher for GSPECT than for AC SPECT (0.94 vs 0.84, p = 0.01) (Fig. 2). The k-statistic showed a poor agreement between the two imaging results (k = 0.4; SE = 0.09).

ROC curve analysis. a Overall analysis. b LAD territory in women. c RCA territory in overweight men
Subanalysis by coronary territory, gender and body habitus
Left anterior descending coronary artery (LAD) territory
In the evaluation of LAD territory GSPECT showed a significantly higher diagnostic accuracy than AC SPECT (area under ROC curves: 0.90 vs 0.76, p < 0.01).
Although anterior artefacts should be more common in women because of breast attenuation, no significant differences between GSPECT and AC SPECT were found when male and female patients were evaluated separately.
In our female population GSPECT and AC SPECT showed similar diagnostic accuracy (area under ROC curves: 0.79 vs 0.72, p = NS) (Fig. 2), while in male patients diagnostic accuracy was significantly higher for GSPECT than for AC SPECT (area under ROC curves: 0.92 vs 0.78, p < 0.01).
In seven men (8.5%) the use of AC generated “overcorrection” artefacts on the anterior wall visualized as perfusion defects more evident in rest than in stress images.
Therefore AC SPECT demonstrated a reduced diagnostic accuracy in the evaluation of LAD territory of male patients.
In overweight men (BMI > 27), GSPECT showed a not significantly higher diagnostic accuracy than AC SPECT (area under ROC curves: 0.85 vs 0.72, p = NS).
Right coronary artery (RCA) territory
In the evaluation of RCA territory GSPECT predicted RCA disease in 31 of 39 patients (79.5% sensitivity) and excluded it in 46 of 65 patients (70.8% specificity), while AC SPECT predicted RCA disease in 28 of 39 patients (71.8% sensitivity) and excluded it in 64 of 65 patients (98.5% specificity). The area under the ROC curve was higher for AC SPECT than for GSPECT, but not significantly (0.87 vs 0.76, p = 0.08). The k-statistic showed a poor agreement between the two imaging results (k = 0.3; SE = 0.09).
In our male population, ROC curves analysis identified cutoffs of 2 for SDS in GSPECT images and 4 for SDS in AC SPECT images as the best for identifying patients with a diseased vessel. With these thresholds, GSPECT and AC SPECT sensitivities were 80.6 vs 75.0% while specificities were 67.4 vs 97.8%. The area under the ROC curve was higher for AC SPECT than for GSPECT, but not significantly (0.87 vs 0.76, p = 0.08). The k-statistic showed a poor agreement between the two imaging results (k = 0.3; SE = 0.11).
In overweight men, GSPECT predicted RCA disease in 12 of 15 patients (80.0% sensitivity) and excluded it in 10 of 15 patients (66.7% specificity), while AC SPECT predicted RCA disease in 12 of 15 patients (80.0% sensitivity) and excluded it in 15 of 15 patients (100% specificity). The area under the ROC curve was significantly higher for AC SPECT than for GSPECT (0.90 vs 0.72, p < 0.05) (Fig. 2). The k-statistic showed a poor agreement between the two imaging results (k = 0.4; SE = 0.17). No significant differences were found for the evaluation of RCA territory between GSPECT and AC SPECT images in female patients.
Left circumflex coronary artery (LCX) territory
In the evaluation of LCX territory GSPECT showed a significantly higher diagnostic accuracy than AC SPECT (area under ROC curves: 0.86 vs 0.73, p < 0.05).
No significant differences were found for the evaluation of LCX territory between GSPECT and AC SPECT images both for normal and overweight patients (p = NS).
Detailed diagnostic accuracies for GSPECT and AC SPECT according to coronary territory, gender and body habitus are summarized in Table 2.
Discussion
Myocardial perfusion imaging is a widely accepted technique for the assessment of CAD as well as for the prediction of patient outcomes, but its accuracy may be suboptimal for a relatively low specificity. Although several studies started from a low SPECT specificity, clinical evidence indicated that AC may increase specificity in normal subjects and in patients with CAD [23–28]. In particular, AC proved to be more useful in patients with a large body surface area or BMI in whom the photonic attenuation, especially in the inferior wall, may reduce SPECT accuracy. Thompson and colleagues [9] examined the value of AC SPECT in normal subjects as well as in obese patients according to a BMI greater or lower than 30. AC proved to be of value for both groups of patients, with nonsignificant changes in sensitivity, but with an enhanced specificity. In particular, in patients with a BMI < 30 specificity increased by 14%, while for patients with a BMI > 30 specificity increased with AC by 33%. On the contrary, Wolak and colleagues [10] recently evaluated the performance of AC in women by using automated quantitative analysis of SPECT images. The authors reported no significant differences both in sensitivity and in specificity neither in SSS values in low-likelihood patients between non-corrected and AC images.
On the other side, gated acquisition provided additional functional information able to differentiate soft tissue attenuation from true perfusion defects, as necrotic myocardium is not expected to move or thicken normally [5, 29]. Taillefer and colleagues [30] demonstrated the enhanced specificity of GSPECT in detecting CAD in women and Doğruca and colleagues [31] demonstrated the increased specificity of inferior wall ischaemia detection of 99mTc-sestamibi GSPECT analysis.
Moreover, as previously described by Links and colleagues [32] AC SPECT and GSPECT can be combined leading to the best option in analysis, even if the use of standard software does not allow gated images to be obtained by iterative reconstruction which is essential for the implementation of AC.
Thus, clinically speaking, it is not clear whether AC SPECT should be preferred to GSPECT and the difference in utilization is based mostly on laboratories’ experience, availability of hybrid cameras and local accuracies, when evaluated. Despite the solid data concerning the usefulness of GSPECT and the increasing evidence on the gain in specificity due to the use of AC, a comparison of accuracies between the two modalities performed in the same patients with known coronary anatomy and differentiated by gender, body habitus and coronary territory is still missing.
This multicentre study demonstrated that using coronary lesions as the standard of reference for ischaemia the use of AC frequently led to a decrease in overall accuracy due to an almost constant lowering of sensitivity and to a frequent reduction in specificity and that only a limited subgroup of patients showed a significant gain in specificity with the use of AC, while in most cases accuracy of AC was similar or worse than that of GSPECT. In agreement with previous evidence [10], AC did not improve specificity for anterior wall evaluation in women while in men it significantly increased accuracy only for the evaluation of the inferior wall, especially in the overweight subgroup (Fig. 3).

Perfusion bullseyes obtained with GSPECT (left column) and AC SPECT (right column), motion bullseye (bottom, left) and selected angiogram (bottom, right). Territories of interest are marked with black arrows. a A 67-year-old woman, BMI 26. No significant differences between GSPECT and AC SPECT; normal motion in LAD territory, no LAD lesions. b A 57-year-old man, BMI 35. Apparent ischaemia in RCA territory at GSPECT analysis, normal inferior wall motion, normal perfusion at AC SPECT, no RCA lesions
In this paper the impact of artefacts generated by AC, such as truncation and misregistration, did not significantly affects our results, and this is probably due to the uniformity of the instrumentation and to the use of the core lab for analysis.
Dosimetric considerations
The effective radiation dose range due to a stress/rest perfusion SPECT study is between 7.2 and 8.1 mSv [14], the effective dose range for a single CT scan (140 KV; 2.5 mA) is between 0.25 mSv and 0.45 mSv (0.017 mSv/cm for the chest region) [33], and thus the total effective dose due to CT scan for a stress/rest AC SPECT is about 0.5 ~ 0.9 mSv (from 6 to 12% of the total amount). Thus, although around 1 mSv for a complete study, the identification of the subgroup that benefits more from AC could allow a targeted dose reduction in SPECT. Progress in cardiac software could also allow the use of a single CT scan reducing by 50% the radiation exposure due to CT.
Study limitations
Although current guidelines recommend an interval of 30–60 min between injection and image acquisition, we decided to follow the fast imaging protocol described by Giorgetti et al. [15] that was already in use in all centres involved in the study.
Results obtained in women are biased by the narrowness of the sample, and specifically by the fact that only few overweight women were present in our population.
In this multicentre study only a visual analysis of myocardial perfusion images was performed, but this limitation could not be avoided due to the lack of a normal database for AC studies. Quantitative perfusion SPECT software results for AC studies are not clinically available and further investigations are needed to obtain an AC database.
Conclusion
According to our results, CT-based nonuniform AC of 99mTc-tetrofosmin GSPECT fast imaging consistently improved specificity without affecting sensitivity only in the evaluation of the inferior wall in overweight men. In the other evaluable subgroups of patients specificity was not significantly affected while sensitivity was frequently reduced. Since the number of overweight women was too small to perform a significative statistic analysis, conclusions on this specific subgroup could not be obtained. The routine application of AC brings in extra radiation exposure to patients; although these dose values are relatively low, this does not justify the extensive use of AC, especially in patients that will not benefit from it. Our results suggest that in clinical practice the use of AC should be limited to patients with a BMI higher than 27; this was statistically demonstrated in the subgroup of men, whereas in overweight women this difference was not assessable because of the limited sample. In the other subgroups of patients standard GSPECT should be preferred. Furthermore “dosimetry-adapted” softwares are needed to avoid unnecessary CT scans in order to further reduce the total effective dose to patients.
References
Maddahi J, Kiat H, Van Train KF, Prigent F, Friedman J, Garcia EV, et al. Myocardial perfusion imaging with technetium-99m sestamibi SPECT in the evaluation of coronary artery disease. Am J Cardiol 1990;66:55E–62.
Palmas W, Bingham S, Diamond GA, Denton TA, Kiat H, Friedman JD, et al. Incremental prognostic value of exercise thallium-201 myocardial single-photon emission computed tomography late after coronary artery bypass surgery. J Am Coll Cardiol 1995;25:403–9.
Nallamothu N, Johnson JH, Bagheri B, Heo J, Iskandrian AE. Utility of stress single-photon emission computed tomography (SPECT) perfusion imaging in predicting outcome after coronary artery bypass grafting. Am J Cardiol 1997;80:1517–21.
Kósa I, Blasini R, Schneider-Eicke J, Neumann FJ, Matsunari I, Neverve J, et al. Myocardial perfusion scintigraphy to evaluate patients after coronary stent implantation. J Nucl Med 1998;39:1307–11.
Fleishmann S, Koepfli P, Namdar M, Wyss CA, Jenni R, Kaufmann PA. Gated (99m)Tc-tetrofosmin SPECT for discriminating infarct from artifact in fixed myocardial perfusion defects. J Nucl Med 2004;45:754–9.
He ZX, Scarlett MD, Mahmarian JJ, Verani MS. Enhanced accuracy of defect detection by myocardial single-photon emission computed tomography with attenuation correction with gadolinium 153 line sources: evaluation with a cardiac phantom. J Nucl Cardiol 1997;4:202–10.
Kluge R, Sattler B, Seese A, Knapp WH. Attenuation correction by simultaneous emission-transmission myocardial single-photon emission tomography using a technetium-99m-labelled radiotracer: impact on diagnostic accuracy. Eur J Nucl Med 1997;24:1107–14.
Patton JA, Townsend DW, Hutton BF. Hybrid imaging technology: from dreams and vision to clinical devices. Semin Nucl Med 2009;39(4):247–63.
Thompson RC, Heller GV, Johnson LL, Case JA, Cullom SJ, Garcia EV, et al. Value of attenuation correction on ECG-gated SPECT myocardial perfusion imaging related to body mass index. J Nucl Cardiol 2005;12:195–202.
Wolak A, Slomka PJ, Fish MB, Lorenzo S, Berman DS, Germano G. Quantitative diagnostic performance of myocardial perfusion SPECT with attenuation correction in women. J Nucl Med 2008;49:915–22.
Banzo I, Pena FJ, Allende RH, Quirce R, Carril JM. Prospective clinical comparison of non-corrected and attenuation- and scatter-corrected myocardial perfusion SPECT in patients with suspicion of coronary artery disease. Nucl Med Commun 2003;24:995–1002.
Garcia EV. SPECT attenuation correction: an essential tool to realize nuclear cardiology’s manifest destiny. J Nucl Cardiol 2007;14:16–24.
Bray GA. Overweight is risking fate. Definition, classification, prevalence, and risks. Ann N Y Acad Sci 1987;499:14–28.
Hesse B, Tägil K, Cuocolo A, Anagnostopoulos C, Bardiés M, Bax J, et al. EANM/ESC procedural guidelines for myocardial perfusion imaging in nuclear cardiology. Eur J Nucl Med Mol Imaging 2005;32:855–97.
Giorgetti A, Rossi M, Stanislao M, Valle G, Bertolaccini P, Maneschi A, et al. Feasibility and diagnostic accuracy of gated SPECT early-imaging protocol: a multicenter study of the Myoview Imaging Optimization Group. J Nucl Med 2007;48:1670–5.
Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. J Nucl Cardiol 2002;9:240–5.
Germano G, Kavanagh PB, Waechter P, Areeda J, Van Kriekinge S, Sharir T, et al. A new algorithm for the quantitation of myocardial perfusion SPECT. I: technical principles and reproducibility. J Nucl Med 2000;41:712–9.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical assessment. Lancet 1986;1:307–10.
Metz CE. Basic principles of ROC analysis. Semin Nucl Med 1978;8:283–98.
Fleiss J. Statistical methods for rates and proportions. 2nd ed. New York: Wiley & Sons; 1981.
Gregoriou GK, Tsui BM, Gullberg GT. Effect of truncated projections on defect detection in attenuation-compensated fanbeam cardiac SPECT. J Nucl Med 1998;39:166–75.
Takahashi Y, Murase K, Higashino H, Mochizuki T, Motomura N. Attenuation correction of myocardial SPECT images with X-ray CT: effects of registration errors between X-ray CT and SPECT. Ann Nucl Med 2002;16:431–5.
Ficaro EP, Fessler JA, Ackermann RJ, Rogers WL, Corbett JR, Schwaiger M. Simultaneous transmission-emission thallium-201 cardiac SPECT: effect of attenuation correction on myocardial tracer distribution. J Nucl Med 1995;36:921–31.
Prvulovich EM, Lonn AHR, Bomanji JB, Jarritt PH, Ell PJ. Effect of attenuation correction on myocardial thallium-201 distribution in patients with a low likelihood of coronary artery disease. Eur J Nucl Med 1997;24:266–75.
Gallowitsch HJ, Syokora J, Mikosch P, Kresnik E, Unterweger O, Molnar M, et al. Attenuation-corrected thallium-201 single-photon emission tomography using a gadolinium-153 moving line source: clinical value and the impact of attenuation correction on the extent and severity of perfusion abnormalities. Eur J Nucl Med 1998;25:220–8.
Hendel RC, Berman DS, Cullom SJ, Follansbee W, Heller GV, Kiat H, et al. Multicenter clinical trial to evaluate the efficacy of correction for photon attenuation and scatter in SPECT myocardial perfusion imaging. Circulation 1999;99:2742–9.
Taneja S, Mohan HK, Blake GM, Livieratos L, Clarke SE. Synergistic impact of attenuation correction and gating in routine myocardial SPECT reporting: 2 year follow-up study. Nucl Med Commun 2008;29:390–7.
Masood Y, Liu YH, Depuey G, Taillefer R, Arujo LI, Allen S, et al. Clinical validation of SPECT attenuation correction using x-ray computed tomography–derived attenuation maps: multicenter clinical trial with angiographic correlation. J Nucl Cardiol 2005;12:676–86.
DePuey EG, Rozanski A. Using gated technetium-99m-sestamibi SPECT to characterize fixed myocardial defects as infarct or artifact. J Nucl Med 1995;36:952–5.
Taillefer R, DePuey EG, Udelson JE, Beller GA, Latour Y, Reeves F. Comparative diagnostic accuracy of Tl-201 and Tc-99m sestamibi SPECT imaging (perfusion and ECG-gated SPECT) in detecting coronary artery disease in women. J Am Coll Cardiol 1997;29:69–77.
Doğruca Z, Kabasakal L, Yapar F, Nisil C, Vural VA, Onsel Q. A comparison of Tl-201 stress-reinjection-prone SPECT and Tc-99m-sestamibi gated SPECT in the differentiation of inferior wall defects from artifacts. Nucl Med Commun 2000;21:719–27.
Links JM, DePuey EG, Taillefer R, Becker LC. Attenuation correction and gating synergistically improve the diagnostic accuracy of myocardial perfusion SPECT. J Nucl Cardiol 2002;9:183–7.
Jessen KA, Shrimpton PC, Geleijns J, Panzer W, Tosi G. Dosimetry for optimisation of patient protection in computed tomography. Appl Radiat Isot 1999;50:165–72.
Acknowledgments
We gratefully acknowledge all the SPAG study investigators from the five Italian centres (Nuclear Medicine of: A.O.V. Cervello – Palermo, Spedali Civili – Brescia, Ospedale Maggiore – Bologna, Ospedale SS Giacomo e Cristoforo – Massa and Fondazione CNR –Regione Toscana “G. Monasterio” – Pisa) who contributed to the recruitment of a valid study population. We also acknowledge the support we have received from Ilaria Citti.
This study was an investigator-initiated study. No sponsor had any role in the analysis and interpretation of data or in the preparation of the manuscript. None of the authors had a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Genovesi, D., Giorgetti, A., Gimelli, A. et al. Impact of attenuation correction and gated acquisition in SPECT myocardial perfusion imaging: results of the multicentre SPAG (SPECT Attenuation Correction vs Gated) study. Eur J Nucl Med Mol Imaging 38, 1890–1898 (2011). https://doi.org/10.1007/s00259-011-1855-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-011-1855-4