
Abstract
Purpose
We present a review of radionuclide imaging of tumour vascular physiology as it relates to angiogenesis. We focus on clinical trials in human subjects using PET and SPECT to evaluate tumour physiology, in particular blood flow and hypoxia.
Methods
A systematic review of literature based on MEDLINE searches updated in February 2010 was performed.
Results
Twenty-nine studies were identified for review: 14 dealt with 15O-water PET perfusion imaging, while 8 dealt with 18F-fluoromisonidazole PET hypoxia imaging. Five used SPECT methods. The studies varied widely in technical quality and reporting of methods.
Conclusions
A subset of radionuclide methods offers accurate quantitative scientific observations on tumour vascular physiology of relevance to angiogenesis and its treatment. The relationship between cellular processes of angiogenesis and changing physiological function remains poorly defined. The promise of quantitative functional imaging at high specificity and low administered dose sustains interest in radionuclide methods.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Angiogenesis is the formation of new blood vessels by capillary sprouting. It is recognised as a molecular and cellular hallmark of cancer. Tumour cells release molecular signals that promote growth of new vessels that in turn provide circulatory support for tumour growth. Folkman suggested cancer could be treated by targeting angiogenesis at a molecular level [1].
Over time, concepts of the mode of action of antiangiogenic and vascular treatments have evolved. Initial ideas were of tumour stasis due to reduced growth of new vessels. An important and distinct idea has been that of acute tumour hypoxia and necrosis due to vascular disruptive effects. More recently, actual improvements in tumour circulation are mooted to result from blockade of new vessel growth, and stabilisation and maturation of established vessels [2].
It is axiomatic that tumour neovasculature is not part of the malignant clone. Rather it is part of the stroma or supporting tissues. This is relevant to the mode of action of vascular-targeted treatments, especially as regards resistance. The tumour vascular genome is more stable than that of malignant cells, and less prone to acquire resistance by selection under treatment. It is therefore less relevant to try to overwhelm vascular resistance by maximum tolerated doses in a narrow therapeutic window. There is more incentive for dose-ranging studies of vascular-targeted treatments to search for a biologically optimum dose.
Similarly, vascular treatments are likely to have different clinical effects from cytotoxics. The acute effects of vascular disruptive agents may take place within minutes to hours and be manifest by liquefactive necrosis rather than classic volume response. Conversely, antiangiogenic agents may facilitate tumour stabilisation. When combined with cytotoxics, if drug delivery is improved, this may lead to a higher objective response rate [2].
With good reason, the definition of angiogenesis is made histologically based on density and architecture of tissue microvessels [3, 4]. With the exception of a minority of lesions localised to surface and lining tissues, angiogenesis cannot yet be feasibly imaged by optical or anatomical methods in vivo.
Methods exist to image the molecular basis of angiogenesis, and are covered elsewhere in this Supplement. Although molecular methods offer high specificity for imaging treatment-target interactions, they still do not image density and architecture of tissue microvessels. Therefore it will remain a question with molecular imaging as to whether treatment-target interactions actually translate in vivo into a change in microvessel density and architecture.
Functional imaging is performed by internalisation of a probe compound of specific physicochemistry that interacts with physiology. The probe includes a tracer moiety, which can be detected by an imaging system. The functional image is a map of tracer distribution in space and time. By use of mathematical models, inferences can be made as to the probe’s distribution and the underlying physiology that determines this.
Functional imaging provides data on living tissue physiology in vivo in dimensions of space and time. It is a potential biomarker for angiogenesis, since changes in microvessel density and architecture are predicted to lead to changes in physiological function. Neovascular blood flow is on average reduced, but also chaotic, disrupted and distorted [5]. The new vessels lack covering pericytes and endothelial tight junctions, and so are relatively permeable. Tissue turgor is increased, delivery of oxygen and nutrients is impaired, and cellular waste accumulates [6, 7].
It follows that changes in blood flow and tissue oxygenation are among the physiological final common pathways of tumour angiogenesis. They are implicitly among the things that vascular-targeted treatments seek to modify. Therefore functional imaging of flow and hypoxia has appeal as a marker of effect for vascular-targeted treatments.
As will be seen from the contents of this Supplement, functional imaging takes several forms, classified on the physics of tracer detection. These include imaging with radionuclides, magnetic resonance, X-ray CT and ultrasound. This paper covers radionuclide imaging with positron emission tomography (PET) and single photon emission computed tomography (SPECT).
Literature search
We reviewed published literature on radionuclide functional imaging of angiogenesis, with reference to the methods used, their technical reliability and results. The physicochemical basis of nuclear medicine imaging is extensively discussed elsewhere [8, 9]. We restrict our scope to in vivo studies in humans, since most of our own work has been in this area. We also exclude studies with molecular imaging agents, as these are covered elsewhere in this issue.
We searched PubMed according to the following strategy:
-
“Neoplasms”[Mesh] AND
-
“Radionuclide Imaging”[Mesh] AND
-
“Neovascularization, Pathologic”[Mesh]
applying the filter:
-
Humans
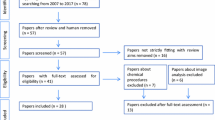
This retrieved 112 reports, of which 53 could be excluded as review articles not presenting primary data. A further 40 could be excluded for various reasons [19 were pre-clinical or laboratory studies, 8 were reports of non-radionuclide methods (CT, MRI, ultrasound), 10 used radionuclide methods to investigate metabolic end-points (principally FDG) and 4 were miscellaneous (physiological model, whole-organ study, SIR-spheres, imaging for surgical localisation)]. There were four reports of human in vivo studies with molecular angiogenesis imaging agents.
The remaining 14 reports described human in vivo radionuclide functional imaging of relevance to angiogenesis. Of these, 12 related to indices of perfusion and the remaining 2 to hypoxic markers [10–23].
We then conducted a more targeted search for literature of potential relevance to vascular functional imaging not indexed under angiogenesis:
-
“Neoplasms”[Mesh] AND
-
“Radionuclide Imaging”[Mesh] AND
-
((“Perfusion”[Mesh] OR “Cell Hypoxia”[Mesh]) NOT “Neovascularization, Pathologic”[Mesh])
applying the filter:
-
Clinical Trials
This retrieved a further 12 reports, comprising 10 studies with hypoxia probes and 2 with perfusion tracers [24–35]. Finally, hand searching of the literature identified 11 further reports concerned with tumour perfusion [36–46].
Review of literature and commentary
Three definitions merit attention, although we have addressed them in more detail in earlier work [8]. Blood flow is the amount of blood moving through a tissue. It has dimensions of quantity (blood)/time/quantity (tissue). Whereas blood is quantified in volume (e.g. ml or dl), tissue may be quantified in volume or weight (e.g. g). Recorded observations typically fall in the range 1–100, provided units are scaled to ml/min per 100 ml. Although authors report results at a range of scales, we have for consistency converted all results to ml/min per 100 ml (or, where mass is used, 100 g).
Perfusion is nutritive blood flow, i.e. flow that actually delivers nutrients to and removes waste from tissues. The contrasting concept is that of a vascular shunt, which carries blood through a tissue without exchange of nutrients or waste.
To estimate perfusion depends on a notion of VT, the volume of distribution for water, also known as exchanging water spaceFootnote 1. VT is an incompletely understood parameter that in this setting represents the proportion of tissue available for perfusion by water. It has dimensions of volume (water)/volume (tissue), quantified respectively in ml and cm3. Examples where VT is predicted to fall below 1 ml/cm3 include tissues that are fatty or necrotic. If VT is overestimated, perfusion will tend to be overestimated, and vice versa. For this reason we prefer to use the term ‘flow’ instead of ‘perfusion’ in settings where a value for VT has been assumed and not measured.
We first review reports concerned with development and validation of methods. In several examples, PET is used as a reference method to validate other imaging modalities (subject to caveats). We then cover reports applying the methods to research and clinical scenarios.
15O-water PET method development and validation
Wilson et al. pioneered application of 15O-water PET to tumours in their study of 20 patients with breast cancer. Later workers have departed little from the basic plan of analysis—a single-compartment model integrating PET image data from tumours and arterial blood. Wilson et al. found mean tumour perfusion (29.8 ± 17 ml/min per 100 ml) was about sixfold higher than normal breast (5.6 ± 1.4 ml/min per 100 ml). Tumour mean VT was 0.56 ± 0.15, whereas VT for normal tissue was 0.14 ± 0.05. The lower VT for normal breast could be attributed to higher fat content.
Interestingly, the ratio of flow/VT was similar for both tumour and normal breast, at 52.8 ± 22.0 and 45.2 ± 20.0, respectively. This raised the possibility that a major difference between tumour and normal tissue might simply be the amount of perfused tissue. Whereas breast would have a large amount of underperfused fat, tumours potentially would have corresponding underperfused hypoxic or necrotic areas. Such heterogeneity in tissue physiology would most likely only resolve at microscopic scales. It could be elucidated only indirectly using radionuclide methods, potentially via spectral or fractal analysis, or other multi-compartmental modelling [48, 49].
Wells et al. studied 37 patients with mainly intra-abdominal tumours using a dynamic 15O-water protocol based on inhaled 15O-carbon dioxide [41]. They found significant between-tumour variability in vascular parameters. Mean perfusion was 46 SD ± 19 ml/min per 100 ml, while mean VT was 0.74 ± 0.15 ml/ml. Test-retest analysis in five patients at an interval of a week found a within-subject coefficient of variation (CV) for perfusion of 11%. This level of repeatability supported 15O-water PET’s use for pharmacodynamic evaluation of vascular-targeted treatmentsFootnote 2.
de Langen et al. assessed repeatability of 15O-water PET across a 7-day interval in nine patients with non-small cell carcinoma of lung [36]. Tumour volumes of interest were defined from sequential 18F-fluorothymidine images. Perfusion and VT were estimated using a single-compartment model including an arterial blood volume component and an image-derived arterial input function. Perfusion estimates were highly repeatable, with an intraclass correlation coefficient (ICC) of 0.95 and standard deviation (SD) of 9%. VT was less repeatable, with ICC of 0.52 and SD of 16%. The variability in VT was thought perhaps to have propagated from the noisy tails of image-derived arterial input functions. Repeatability was independent of absolute values of perfusion and VT across the range studied. The authors concluded that the smallest detectable change for perfusion in this setting would be 18%, and for VT would be 32%.
15O-water PET for validation of other imaging modalities
Eby et al. used 15O-water PET to validate a semi-quantitative dynamic contrast-enhanced (DCE) MRI method in a retrospective analysis of 15 patients with locally advanced carcinoma of breast [11]. The MRI end-points were tumour peak percent enhancement and peak signal enhancement ratio (SER). The authors also had FDG PET data for which they could calculate FDG metabolic rates and tissue transport constant K1. K1 reflects tissue delivery of FDG, and therefore responds most nearly to blood flow. The authors found that SER correlated with 15O-water blood flow (r = 0.73, p = 0.002) and with K1 (r = 0.76, p = 0.001), but not with FDG metabolic rate (r = 0.44, p = 0.101). This supports the idea that perfusion would be an important factor in MRI enhancement, as predicted in physiological models. It also agrees with other reports showing a lack of association between vascular end-points and glucose metabolism of tumours.
It is not surprising that the correlation between 15O-water PET and DCE MRI SER is less than perfect, given that DCE MRI also responds to vascular permeability. To deconvolve the relative contributions of perfusion and permeability to total MRI signal requires more sophisticated data analysis than SER [8]. Improved image coregistration in dedicated PET/MRI machines might also help.
Ng et al. used 15O-water PET to validate perfusion CT (pCT) in 14 patients with solid tumours. The PET analysis was based on a first-pass ‘autoradiographic’ model [10]. The authors found no significant difference between the mean and SD of blood flows measured by CT (25.9 ± 15.4 ml/min per 100 g) and PET (27.8 ± 14.0 ml/min per 100 g). They concluded that pCT would have promise as a measure of blood flow in clinical studies.
Autoradiographic methods (hereafter ‘AM’) have an important limitation in that they must assume a value for the VT of water [51]. Although such assumptions are validated for muscle and the cerebral circulation, this is not so for tumours. Several reports reviewed here found tumour VT of water to be variable. This casts doubt on the validity of 15O-water PET autoradiography as a tool for validation of pCT. Ng et al. note they used a ‘simple blood flow model’ for PET, based on the limitations of the scanner available at the time of the study. Newer scanners permit higher temporal resolution PET and support models capable of estimating both perfusion and VT. One useful task for such devices would be to compare autoradiographic and dynamic PET perfusion models in tumours.
Lüdemann et al. related 15O-water PET (AM) to 4 MRI methods in 12 patients with tumours of brain [12]. The MRI methods included three qualitative analyses of DCE/susceptibility-contrast data (DCE MRI/DSC MRI) and pulsed arterial spin labelling (PASL). They found that all five methods correlated, in both normal brain and tumour. The MRI methods tended however to overestimate tumour perfusion compared to PET, by from 10 to 180%. The authors reported that the T2* method of DSC and PASL “depict[ed] median perfusion most reliably”. The authors justify their focus on the median insofar as 15O-water PET AM had been shown to underestimate perfusion in high flow areas of the human brain.
These observations are a reminder that parametric estimates in functional imaging may be sensitive to a range of interacting factors. These factors may include regional physiology of tissues (e.g. tissue type, absolute values of flow, heterogeneity of blood flow and water distribution), probe characteristics (e.g. molecular weight, electrochemistry), and imaging technology (e.g. spatial and temporal resolution). Analytical models are designed and validated for a particular combination of tissue, probe and imaging technology. The models may need to be scrutinised and revised for use in different settings. In particular, most of the work to validate radionuclide imaging of vascular function was performed for heart and brain. There is still considerable work needed to cross-validate these methods for tumours, and with newer probes, imaging technologies and analytic models.
Nonetheless, 15O-water PET is established as a repeatable method for quantitative measurement of tumour perfusion in vivo in human subjects. It is desirable for workers with 15O-water PET to use methods that do not assume a value for tumour VT, in view of this parameter’s wide reported variability and its influence on estimates of perfusion.
Descriptive and pharmacodynamic studies of tumour vascular physiology
Ponto et al. used 15O-water PET (AM) to study seven women before and during radiotherapy for cancer of the cervix [45]. Mean tumour blood flow at baseline was 41.5 ± 11.9 ml/min per 100 g. In four women who had serial studies, there was a trend towards increasing flow during treatment.
Yamaguchi et al. correlated 15O PET-based measures of flow with 3 grades of angiographic vascularity in liver metastases from 15 patients with colorectal carcinoma [20]. This study cross-validated 15O-carbon dioxide steady-state and 15O-water PET (AM) methods. Using 15O-water PET, they found mean blood flow of 52.9 ml/min per 100 g for angiographic grade A tumours, and 35.7 and 31.7 ml/min per 100 g, respectively, for grades B and C. These values were greater than previously suggested by ultrasound studies. They assumed a value of 1 for VT of water in tumour tissue.
Hoekstra et al. assessed the feasibility of 15O-water PET in locally advanced non-small cell carcinoma of lung in ten patients [19]. They used 18F-FDG PET for tumour localisation and for correlative data on glucose metabolism. They found wide variation in perfusion between tumours, ranging from 15 to 129 ml/min per 100 ml. VT for water ranged from 0.45 to 0.78 ml/ml. Simplified ratio-based analytic methods to study blood flow correlated only poorly with dynamic modelling. They concluded that PET studies of perfusion would need to be done in large populations, so that vascular function could be compared with clinical outcomes.
Gupta et al. used 15O-water PET to study the effect of nicotinamide and carbogen on delivery of 5-fluorouracil (5-FU) in six patients with colorectal cancer metastases [37]. They found that nicotinamide and carbogen increased blood oxygen tension by around 200%, and increased tumour perfusion by 52%, while decreasing perfusion of kidney and liver by 30–40%. This was associated with trends to similar increased tumour and reduced normal tissue 5-FU uptake. Paradoxically however, there was no increase in actual 5-FU retention or tissue exposure, perhaps reflecting increased washout. Tumour perfusion varied in the range 8–88 ml/min per 100 ml, while VT for water ranged from 0.41 to 1.09 ml/ml.
Hentschel et al. used 15O-water PET in a comparative study of tumour and normal breast tissue in ten patients with advanced invasive ductal carcinoma of breast [13]. They found that tumour vascular parameters were about threefold greater than normal tissue (perfusion 59.2 versus 22.1 ml/min per 100 g; VT of water 0.58 versus 0.16 ml/g; VT of water is low in normal breast since it is a fatty tissue). Glucose metabolism was about 30-fold greater for tumours (SUV 7.76 versus 0.33, metabolic rate 5.4 versus 0.18 mg/min per 100 g). Pixel-wise analysis revealed within-lesion heterogeneity in these values.
These studies confirm wide inter-subject variation in tumour perfusion and VT, ranging across two orders of magnitude. Tumours are heterogeneous, within both individuals and populations. Although angiogenesis is a molecular hallmark of cancer, there is a wide range of vascular phenotypes.
Evaluation of response to cytotoxics and antiangiogenic agents with 15O-water PET
Herbst et al. used 15O-water PET (AM) to study 25 patients with various solid tumours in a phase I dose-ranging study of endostatin [18]. They also took FDG PET scans and tumour biopsies. Images were recorded at baseline and every 4 weeks on treatment. Endostatin generally reduced blood flow and glucose metabolism. This was linked to an increase in tumour and endothelial cell apoptosis. In a preliminary report from this group it seemed there might be a simple effect of endostatin to reduce blood flow with increasing doses [44]. That finding was not borne out, since blood flow dose-response followed a V-shaped course, with its nadir at around 180 mg/m2 endostatin. Although the study drug had detectable effects, the complex result with PET could not be interpreted.
Mankoff et al. used 15O-water and FDG PET to study 37 patients with locally advanced breast cancer before chemotherapy [43]. They found both metabolic rate for FDG (MRFDG) and blood flow were higher in tumours than in normal breast. There was a weak correlation between high MRFDG and poor response to chemotherapy. High flow relative to MRFDG was the best predictor of a complete response (p = 0.02).
A later publication from this group reported an overlapping population of 35 patients imaged at baseline and again after 2 months [42]. Most of the patients (30/35) had a clinical response. Blood flow tended to fall in chemotherapy responders (−32%) but increased in non-responders (+48%) (p < 0.005). This analysis was robust to partial-volume correction.
Anderson et al. used 15O-water and 15O-carbon monoxide PET at baseline and after 4–8 weeks of treatment with razoxane in 12 patients with renal cell carcinoma [39]. Razoxane is an oral agent with mixed cytotoxic and antiangiogenic activity. The perfusion of renal tumours at 87 ml/min per 100 ml (range: 33–167) was lower than that of normal kidney (range: 116–288 ml/min per 100 ml), though still higher than reported ranges for most reference tissues. Comparison of baseline with follow-up scans found no significant changes in tumour perfusion (mean value fell to 72 ml/min per 100 ml), VT of water (rose from 0.66 to 0.71) or blood volume (fell from 0.18 to 0.167). Neither was there any significant change in the subgroup of four patients showing disease progression.
Lara et al. used PET with 15O to study 14 of 30 patients with renal cell carcinoma (RCC) who had SU5416 plus low dose interferon (IFN)-alpha 2B [15]. They do not name the 15O probe used, nor describe the method used to analyse PET images, and in fact do not provide any numerical estimates of perfusion in their report, but refer to ‘perfusion imaging studies’. Correlative end-points included FDG PET, and plasma vascular endothelial growth factor (VEGF) and plasminogen activator inhibitor-1. They reported significant declines in plasma markers to suggest the combination would have biological activity. They were able to monitor response with PET in five patients. From these small numbers and limited reporting, glucose metabolism and intensity of perfusion images seemed to increase in the presence of progressive disease. Poor clinical outcomes (6% 1-year event-free survival and adverse toxicity) reduced the authors’ enthusiasm for further work with SU5416 and interferon in RCC.
Kurdziel et al. used 15O-water (AM), 11C-carbon monoxide and FDG PET in six patients receiving thalidomide for androgen-independent prostate cancer [40]. They found an inverse correlation between change in blood flow and prostate-specific antigen (r = −0.83, p = 0.032). This small study is compatible with the idea that response to antiangiogenic agents is associated with improved tumour circulation.
Miller et al. used 15O-water and 11C-carbon monoxide PET in 19 of 70 patients with locally advanced carcinoma of breast [14]. This was in a phase II trial of primary chemotherapy with sequential doxorubicin and docetaxel. Their aim was to correlate clinical and laboratory outcomes with surrogate markers also including serology and ultrasound. Investigations were done at baseline, at cross-over and the end of chemotherapy. The clinical response rate was 91%, and the authors found that uptake of PET tracers fell during treatment in almost all patients. It was an ambitious study design with a disappointing result in that no parameter reliably correlated with microvascular density or predicted response. The PET results are hard to interpret in view of limited methodological reporting; the methods are not referenced, and no quantitative calculations are made, only ‘uptake indices’ (similar to Lara et al.).
The reports in this section are interesting in that there remains no clear evidence from 15O-water PET imaging to support the idea of vascular normalisation, with improved perfusion, as a consequence of antiangiogenic treatment.
Positive evidence of response to vascular disrupting agents with 15O-water PET
Logan et al. used 15O-water PET to monitor response at baseline and 2, 4 and 24 h post-infusion in patients with pulmonary metastases in a phase I trial of interleukin-1 alpha (IL-1) and carboplatin [17]. Of 16 patients, 8 could be scanned and had evaluable data. The mean baseline tumour blood flow was 182 ml/min per 100 g. It fell after 2 h to 135 ml/min per 100 g (p < 0.008), then improved to 167 at 4, and 162 at 24 h. During this time the VT of water ranged from 0.26 to 0.83. Liver blood flow was measured in parallel in four patients and showed no change with treatment. There was significant neutropaenia accompanied by increased cell surface expression of adhesion integrin CD11b. This study revealed early effects of IL-1 and carboplatin on vascular and leukocyte physiology.
Anderson et al. used 15O-water and 15O-carbon monoxide PET to study 13 patients with solid tumours in a phase I dose-ranging study of the vascular disrupting agent combretastatin A4P (CA4P) [52]. Thirty minutes after infusion of CA4P they found that tumour perfusion fell on average by 49% (p = 0.001), and blood volume fell by 15% (p = 0.007). Higher doses in the range 5 –114 mg/m2 led to larger falls that persisted out to 24 h. The VT of water ranged from 0.50 to 0.87. Of note they also recorded falls in cardiac output and circulation of the spleen and kidney, to suggest systemic as well as local effects of CA4P.
In contrast to cytotoxics and antiangiogenics, the vascular disrupting agents show definite and rapid effects on 15O-water PET parameters. These studies derive added persuasive power in that they estimate and thereby control for variation in VT of water.
Proposed application of MIBI SPECT to studies of tumour perfusion
Methoxyisobutylisonitrile (MIBI) is rapidly and extensively metabolised by respiring tissues. 99mTc-labelled MIBI has established use as a SPECT marker of cardiac perfusion, where metabolism is sufficiently rapid and extensive for blood flow to determine tissue uptake. Two studies report MIBI’s adaptation for imaging tumour blood flow.
Kim et al. used MIBI SPECT to study 29 patients with carcinoma of breast before primary surgery [21]. They found no correlation between a tracer washout index and intratumoural microvessel density or VEGF mRNA reverse transcriptase polymerase chain reaction (RT-PCR). There was a negative correlation between tracer washout and power Doppler US grading (r = −0.945, p = 0.001). They described ultrasound as ‘well correlated’ with microvascular density (r = 0.552, p = 0.033; we would say a correlation in the range 0.3–0.7 is moderate at best). They concluded that ultrasound could predict tumour angiogenesis but more study was needed for 99mTc-MIBI SPECT.
Cermik et al. used 99mTc-MIBI SPECT to study 26 patients with carcinoma of lung under normal and raised levels of arterial oxygenation [35]. They found an up to 10% increase in tumour tracer uptake following oxygen inhalation. The authors interpreted their results as showing a positive acute cellular response of tumour tissue to raised oxygen tensions, analogous to the probe’s ability to diagnose ‘hibernating myocardium’. The authors concede their interpretation is speculative, since they were not able to directly measure intratumoural oxygen tension.
In summary, although MIBI is of established value in clinical imaging of cardiac perfusion, one has to be more sceptical about its significance in malignant disease. The basic point is that the MIBI probe provides information not only about its delivery into tissue via the circulation, but also about metabolic viability of those tissues it reaches. Cermik et al.’s finding that MIBI uptake is sensitive to oxygenation and ‘cellular response’ sheds light on Kim et al.’s finding of only moderate correlation between MIBI uptake and a Doppler ultrasound index of perfusion.
Evaluation of tumour hypoxia with 18F-misonidazole (FMISO) PET
The imaging paradigm for hypoxia is to internalise a probe that accumulates in hypoxic/acidotic tissues and washes out from normoxic/normal pH tissues. The main technical challenge in this field is to develop probes with improved signal to noise characteristics. It is a task for medicinal chemists to design agents with rapid and extensive distribution and washout in low-perfusion tissues.
Rajendran et al. used FMISO to study 19 patients with soft tissue sarcomas prior to surgery. This included ten patients imaged before and after preoperative chemotherapy [28]. The primary analysis was FMISO regional tissue to blood ratio. This was correlated with FDG images and histological VEGF expression. The authors found no consistent relationship between hypoxic volume and tumour grade or volume, FDG uptake or VEGF expression; 76% of tumours showed significant hypoxia at baseline, usually heterogeneous in distribution. Most tumours showed lower uptake of both FMISO and FDG after chemotherapy.
Eschmann et al. used FMISO to study 40 patients with cancers of head and neck and lung (non-small cell) who had radiotherapy [26]. Their primary analysis was ratio-based (SUVs and tumour to reference tissue ratios) although they also plotted time-activity curves for visual classification. The authors found that accumulation of probe in the time-activity curve, high SUV and high tumour to reference tissue ratios were predictive of local recurrence at 1 year. They concluded that FMISO might be used at baseline to select for intensified therapy.
Lawrentschuk et al. used FMISO to study 17 patients with various renal tumours prior to nephrectomy [23]. They compared this with histological microvascular density in 15 patients and with polarographic oxygen tension in 3 patients. They found only mild FMISO uptake in the subset of tumours that were renal cell carcinomas. Polarography found only mild hypoxia in RCCs, in that median pO2 did not fall below 9.5 mmHg. The authors found no correlation (r = −0.02959, range: 1.0–1.0) between microvascular density and tumour uptake of FMISO.
Although this is an important negative result, it may simply reflect the loss of information about tissue heterogeneity inherent in whole-tumour analyses. The physical limit on resolution of PET is at best 1–2 mm. This seems likely to prohibit the coregistration needed to study the anatomical correlation of hypoxia and angiogenic markers with in vivo imaging. The question could be approached in a pixel-wise analysis combining PET hypoxia and molecular angiogenesis probes.
Gagel et al. reported preliminary data on the use of FMISO and FDG PET to study eight patients with non-small cell carcinoma of lung before and at the end of chemoradiotherapy with gemcitabine and vinorelbine [31]. They were able to demonstrate hypoxic tumour subvolumes which they postulated might be sites for later local recurrence.
Rischin et al. used FMISO to study 45 patients with squamous cell carcinoma of the head and neck in a randomised study of cisplatin chemoradiotherapy with or without tirapazamine [32]. This followed on from previously reported pilot work [25, 30]. All patients had pre- and mid-treatment scans with qualitative scoring of uptake. The baseline prevalence of hypoxia was 71%. In 23 patients not receiving tirapazamine, baseline hypoxia was a strong predictor for locoregional failure (hazard ratio: 7.1, exact log-rank, p = 0.038), whereas in 22 patients receiving tirapazamine, hypoxia was no longer adverse for failure. This was an important study to support the idea that tirapazamine would act by targeting hypoxic tumour cells.
Swanson et al. used FMISO to study 24 patients with glioblastoma multiforme [22]. In view of the role of hypoxia in upregulating angiogenesis, they hypothesised that hypoxic volumes on PET would show increased vascular permeability on concurrent MRI. FMISO was analysed as a tumour to blood activity ratio. They found a significant correlation between MRI- and PET-defined volumes, and concluded that hypoxia might indeed drive angiogenesis and the peripheral growth of glioblastomas.
Other PET hypoxia probes
Lehtiö et al. used 15O-water (AM) and 18F-fluoroerythronitroimidazole (FETNIM) to study ten patients with cancer of the head and neck [29]. They found that performance of FETNIM is poor in tissues such as skeletal muscle with blood flow in the range 2–6 ml/min per 100 g. It performs well once flows exceed 20 ml/min per 100 g, as seen in many tumours. In these settings, hypoxia is reasonably estimated by static tissue to plasma FETNIM activity ratios. Importantly the authors note that plasma is preferable to muscle as a reference tissue for such ratios, since plasma tracer levels are more uniform.
A later report from Lehtiö et al. increased the study population to 21 in the setting of primary radiotherapy [38]. They also used FDG PET to define tumour volumes. They found blood flows in the range 12.4–64.1 ml/min per 100 g. They found a worse prognosis after radiotherapy in cases of higher blood flow and/or higher fractional hypoxic volume.
Dietz et al. used 60Cu-diacetyl-bis (N4-methylthiosemicarbazone) (ATSM) PET to study 19 patients with carcinoma of rectum who had preoperative 5-FU chemoradiotherapy [24]. The authors calculated a semi-quantitative tumour to muscle activity ratio, where higher ratios corresponded to increased tumour hypoxia. Tumours with ratios above the population median 2.6 were less likely to respond and had worse 3-year survival (p < 0.05). FDG uptake was measured coincidentally in 11 patients and did not correlate with ATSM uptake or hypoxia.
SPECT hypoxia probes
Hulshof et al. used 99mTc-hexamethylpropylene amine oxime (HMPAO) SPECT in a pre- and post-treatment protocol to study 19 patients with glioblastoma multiforme who had radiotherapy with nicotinamide and carbogen (respired 95% oxygen, 5% carbon dioxide) [34]. These agents are thought to improve hypoxia perhaps by increasing tumour perfusion and oxygen delivery. The SPECT assay’s reliability was evaluated in a further six patients who had test and re-test without intervening treatment. The authors found no significant change in tumour or brain perfusion, or their ratio, compared to control patients. The negative findings in this report compared to Gupta et al. most likely reflect the inferior sensitivity of earlier SPECT methods compared to PET.
Hoebers et al. studied the safety and biodistribution of the SPECT hypoxia marker 99mTc-BRU 59-21 in ten patients with carcinoma of the head and neck up to 2 weeks before their surgery [33]. Image data were correlated with pimonidazole immunohistochemistry. Tumour to normal tissue ratios for the primary correlated with intensity of pimonidazole staining (p < 0.05). The correlation appeared less reliable for involved lymph nodes.
Li et al. used 99mTc-HL91 SPECT to study 32 patients with non-small cell carcinoma of lung who had radiotherapy [27]. All patients had a baseline scan, and 18 had scans during and after the end of treatment. The authors calculated a tumour to normal tissue (T/N) radioactivity ratio. They found a threshold baseline T/N ratio of 1.47 to segregate for response rates of 25% (if T/N higher) and 81% (if T/N lower; p = 0.002). The median survival for these groups was 14 and 17.2 months, respectively (p = 0.043).
Although there is a large literature to link hypoxia with angiogenesis at the molecular level, the links are less clearly drawn in functional imaging [53]. In particular, we have not seen in vivo study in humans of the interaction between antiangiogenic treatment and tumour hypoxia. In the case of FMISO, Rischin and colleagues found that tirapazamine could greatly reduce the excess hazard associated with tumour hypoxia. The bittersweet here is that tirapazamine has essentially been withdrawn from development due to toxicity. There remains wide scope for radionuclide hypoxia imaging to investigate other agents of vascular relevance.
General comments
Of the three physiological parameters we have reviewed, perfusion is the most readily apparent biomarker for angiogenesis, insofar as blood flow is a vessel’s usual function. The biomarker potential of VT is in its link with exchange of water between vessel lumen and the extravascular space. The efficiency of such exchange, and hence VT, is likely to depend on the state of the tumour capillary network. We could predict that VT would be reduced where recently formed capillaries are structurally disordered. VT might then increase with vascular normalisation.
Another factor reducing VT however is likely to be necrosis. Necrosis would limit the scale of VT’s recovery with vascular normalisation. This could turn out to be of relevance to more metabolic probes such as FDG and the hypoxic markers. These probes could define the amount of viable tissue in a tumour volume. Knowledge of the amount of viable tissue would permit more precise statements about the level of ongoing angiogenesis to account for VT.
The ability to microdose lends radionuclide imaging the advantage that a wide range of probe molecules can potentially be investigated, with reduced risk of chemical toxicity. There is large scope for PET and SPECT probes to be designed to monitor specific points in physiological functional pathways. The principal technical drawback of radionuclides is that resolution tends to be poorer, due to the physics of image acquisition. Whereas the strongest MRI magnets can now resolve down to submillimetre scales, the best that PET can theoretically achieve is on the order of 1–2 mm. The advent of PET/CT has been significant in that volumes of interest for PET analysis can now be more confidently related to anatomy. Even so, radionuclide methods can inform only indirectly as to heterogeneity of tissue structure and function on microscopic scales.
A challenge with radionuclides compared to other imaging modalities is that image acquisition times tend to be longer, in the order of minutes. This reduces temporal resolution and means that more rapid dynamic processes cannot be as readily studied. This point is mitigated by newer generations of camera that include more sensitive detector crystals and improved electronics.
A major point to arise from this review is the variable rigour of methods for acquisition and analysis of 15O-water PET data. We are very sceptical as to whether simplified methods based on metabolic trapping, developed for use in physiological heart and brain, can reliably be applied to study of tumours. Such methods have given the impression that radionuclide functional imaging is ‘semi-quantitative’ [54]. In fact radionuclides offer great potential for quantitative imaging, since the internalised dose of tracer can be carefully controlled and exactly measured.
This review has identified a range of applications for radionuclide imaging of vascular function, primarily in research settings. Most of these remain in the category of ‘shows promise’. The most successful results seen with 15O-water PET perfusion were studies of vascular disruptive agents. There is surely potential to apply the methods for study of antiangiogenic agents.
With attention to methodological detail, including assays of repeatability, and more accurate data analysis supported by newer generations of PET/CT cameras, PET functional imaging has the potential to reveal much about tumour circulation and the effect of treatment. It will help us understand the pathophysiology of tumour angiogenesis and its treatment. It promises to reduce attrition and wasted effort in drug development. These methods should continue to be developed and reported.
Notes
The term VT is the result of a recent consensus and replaces previous usage, notably VD [47]. For consistency we adhere to the current nomenclature.
References
Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med 1971;285:1182–6.
Jain RK. Antiangiogenic therapy for cancer: current and emerging concepts. Oncology (Williston Park) 2005;19(4 Suppl 3):7–16.
Gimbrone MA, Leapman SB, Cotran RS, Folkman J. Tumor angiogenesis: iris neovascularization at a distance from experimental intraocular tumors. J Natl Cancer Inst 1973;50(1):219–28.
Weidner N, Semple J, Welch W, Folkman J. Tumor angiogenesis and metastasis—correlation in invasive breast carcinoma. N Engl J Med 1991;324(1):1–8.
Less J, Skalak T, Sevick E, Jain R. Microvascular architecture in a mammary carcinoma: branching patterns and vessel dimensions. Cancer Res 1991;51(1):265–73.
Hashizume H, Baluk P, Morikawa S, McLean J, Thurston G, Roberge S, et al. Openings between defective endothelial cells explain tumor vessel leakiness. Am J Pathol 2000;156(4):1363–80.
Jain RK. Determinants of tumor blood flow: a review. Cancer Res 1988;48(10):2641–58.
Laking GR, West C, Buckley DL, Matthews J, Price PM. Imaging vascular physiology to monitor cancer treatment. Crit Rev Oncol Hematol 2006;58(2):95–113.
Mees G, Dierckx R, Vangestel C, Van de Wiele C. Molecular imaging of hypoxia with radiolabelled agents. Eur J Nucl Med Mol Imaging 2009;36(10):1674–86.
Ng CS, Kodama Y, Mullani NA, Barron BJ, Wei W, Herbst RS, et al. Tumor blood flow measured by perfusion computed tomography and 15O-labeled water positron emission tomography: a comparison study. J Comput Assist Tomogr 2009;33(3):460–5.
Eby PR, Partridge SC, White SW, Doot RK, Dunnwald LK, Schubert EK, et al. Metabolic and vascular features of dynamic contrast-enhanced breast magnetic resonance imaging and 15O-water positron emission tomography blood flow in breast cancer. Acad Radiol 2008;15(10):1246–54.
Lüdemann L, Warmuth C, Plotkin M, Förschler A, Gutberlet M, Wust P, et al. Brain tumor perfusion: comparison of dynamic contrast enhanced magnetic resonance imaging using T1, T2, and T2* contrast, pulsed arterial spin labeling, and H2 15O positron emission tomography. Eur J Radiol 2009;70(3):465–74.
Hentschel M, Paulus T, Mix M, Moser E, Nitzsche EU, Brink I. Analysis of blood flow and glucose metabolism in mammary carcinomas and normal breast: a H2 15O PET and 18F-FDG PET study. Nucl Med Commun 2007;28(10):789–97.
Miller K, Soule S, Calley C, Emerson R, Hutchins G, Kopecky K, et al. Randomized phase II trial of the anti-angiogenic potential of doxorubicin and docetaxel; primary chemotherapy as Biomarker Discovery Laboratory. Breast Cancer Res Treat 2005;89(2):187–97.
Lara PN, Quinn DI, Margolin K, Meyers FJ, Longmate J, Frankel P, et al. SU5416 plus interferon alpha in advanced renal cell carcinoma: a phase II California Cancer Consortium Study with biological and imaging correlates of angiogenesis inhibition. Clin Cancer Res 2003;9(13):4772–81.
Anderson H, Yap J, Wells P, Miller M, Propper D, Price P, et al. Measurement of renal tumour and normal tissue perfusion using positron emission tomography in a phase II clinical trial of razoxane. Br J Cancer 2003;89(2):262–7.
Logan T, Jadali F, Egorin M, Mintun M, Sashin D, Gooding W, et al. Decreased tumor blood flow as measured by positron emission tomography in cancer patients treated with interleukin-1 and carboplatin on a phase I trial. Cancer Chemother Pharmacol 2002;50(6):433–44.
Herbst R, Mullani N, Davis D, Hess K, McConkey D, Charnsangavej C, et al. Development of biologic markers of response and assessment of antiangiogenic activity in a clinical trial of human recombinant endostatin. J Clin Oncol 2002;20(18):3804–14.
Hoekstra C, Stroobants S, Hoekstra O, Smit E, Vansteenkiste J, Lammertsma AA. Measurement of perfusion in stage IIIA-N2 non-small cell lung cancer using H2 15O and positron emission tomography. Clin Cancer Res 2002;8(7):2109–15.
Yamaguchi A, Taniguchi H, Kunishima S, Koh T, Yamagishi H. Correlation between angiographically assessed vascularity and blood flow in hepatic metastases in patients with colorectal carcinoma. Cancer 2000;89(6):1236–44.
Kim S-W, Park S-S, Ahn S-J, Chung K-W, Moon WK, Im J-G, et al. Identification of angiogenesis in primary breast carcinoma according to the image analysis. Breast Cancer Res Treat 2002;74(2):121–9.
Swanson KR, Chakraborty G, Wang CH, Rockne R, Harpold HLP, Muzi M, et al. Complementary but distinct roles for MRI and 18F-fluoromisonidazole PET in the assessment of human glioblastomas. J Nucl Med 2009;50(1):36–44.
Lawrentschuk N, Poon AMT, Foo SS, Putra LGJ, Murone C, Davis ID, et al. Assessing regional hypoxia in human renal tumours using 18F-fluoromisonidazole positron emission tomography. BJU Int 2005;96(4):540–6.
Dietz DW, Dehdashti F, Grigsby PW, Malyapa RS, Myerson RJ, Picus J, et al. Tumor hypoxia detected by positron emission tomography with 60Cu-ATSM as a predictor of response and survival in patients undergoing neoadjuvant chemoradiotherapy for rectal carcinoma: a pilot study. Dis Colon Rectum 2008;51(11):1641–8.
Rischin D, Peters L, Hicks R, Hughes P, Fisher R, Hart R, et al. Phase I trial of concurrent tirapazamine, cisplatin, and radiotherapy in patients with advanced head and neck cancer. J Clin Oncol 2001;19(2):535–42.
Eschmann S-M, Paulsen F, Reimold M, Dittmann H, Welz S, Reischl G, et al. Prognostic impact of hypoxia imaging with 18F-misonidazole PET in non-small cell lung cancer and head and neck cancer before radiotherapy. J Nucl Med 2005;46(2):253–60.
Li L, Yu J, Xing L, Ma K, Zhu H, Guo H, et al. Serial hypoxia imaging with 99mTc-HL91 SPECT to predict radiotherapy response in nonsmall cell lung cancer. Am J Clin Oncol 2006;29(6):628–33.
Rajendran JG, Wilson DC, Conrad EU, Peterson LM, Bruckner JD, Rasey JS, et al. [18F]FMISO and [18F]FDG PET imaging in soft tissue sarcomas: correlation of hypoxia, metabolism and VEGF expression. Eur J Nucl Med Mol Imaging 2003;30(5):695–704.
Lehtiö K, Oikonen V, Nyman S, Grönroos T, Roivainen A, Eskola O, et al. Quantifying tumour hypoxia with fluorine-18 fluoroerythronitroimidazole ([18F]FETNIM) and PET using the tumour to plasma ratio. Eur J Nucl Med Mol Imaging 2003;30(1):101–8.
Hicks RJ, Rischin D, Fisher R, Binns D, Scott AM, Peters LJ. Utility of FMISO PET in advanced head and neck cancer treated with chemoradiation incorporating a hypoxia-targeting chemotherapy agent. Eur J Nucl Med Mol Imaging 2005;32(12):1384–91.
Gagel B, Reinartz P, Demirel C, Kaiser HJ, Zimny M, Piroth M, et al. [18F] fluoromisonidazole and [18F] fluorodeoxyglucose positron emission tomography in response evaluation after chemo-/radiotherapy of non-small-cell lung cancer: a feasibility study. BMC Cancer 2006;6:51.
Rischin D, Hicks RJ, Fisher R, Binns D, Corry J, Porceddu S, et al. Prognostic significance of [18F]-misonidazole positron emission tomography-detected tumor hypoxia in patients with advanced head and neck cancer randomly assigned to chemoradiation with or without tirapazamine: a substudy of Trans-Tasman Radiation Oncology Group Study 98.02. J Clin Oncol 2006;24(13):2098–104.
Hoebers FJP, Janssen HLK, Olmos AV, Sprong D, Nunn AD, Balm AJM, et al. Phase 1 study to identify tumour hypoxia in patients with head and neck cancer using technetium-99m BRU 59-21. Eur J Nucl Med Mol Imaging 2002;29(9):1206–11.
Hulshof MC, Rehmann CJ, Booij J, van Royen EA, Bosch DA, González González D. Lack of perfusion enhancement after administration of nicotinamide and carbogen in patients with glioblastoma: a 99mTc-HMPAO SPECT study. Radiother Oncol 1998;48(2):135–42.
Cermik TF, Altiay G, Firat MF, Hatipoglu ON, Berkarda S. Assessment of Tc-99 m sestamibi tumor tissue uptake under the influence of increased arterial oxygen saturation. Nucl Med Biol 2005;32(2):165–70.
de Langen AJ, Lubberink M, Boellaard R, Spreeuwenberg MD, Smit EF, Hoekstra OS, et al. Reproducibility of tumor perfusion measurements using 15O-labeled water and PET. J Nucl Med 2008;49(11):1763–8.
Gupta N, Saleem A, Kötz B, Osman S, Aboagye EO, Phillips R, et al. Carbogen and nicotinamide increase blood flow and 5-fluorouracil delivery but not 5-fluorouracil retention in colorectal cancer metastases in patients. Clin Cancer Res 2006;12(10):3115–23.
Lehtiö K, Eskola O, Viljanen T, Oikonen V, Grönroos T, Sillanmäki L, et al. Imaging perfusion and hypoxia with PET to predict radiotherapy response in head-and-neck cancer. Int J Radiat Oncol Biol Phys 2004;59(4):971–82.
Anderson HL, Yap JT, Miller MP, Robbins A, Jones T, Price P. Assessment of pharmacodynamic vascular response in a phase I trial of combretastatin A4 phosphate. J Clin Oncol 2003;21(15):2823–30.
Kurdziel K, Figg W, Carrasquillo J, Huebsch S, Whatley M, Sellers D, et al. Using positron emission tomography 2-deoxy-2-[18F]fluoro-D-glucose, 11CO, and 15O- water for monitoring androgen independent prostate cancer. Mol Imaging Biol 2003;5(2):86–93.
Wells P, Jones T, Price P. Assessment of inter- and intrapatient variability in C15O2 positron emission tomography measurements of blood flow in patients with intra- abdominal cancers. Clin Cancer Res 2003;9(17):6350–6.
Mankoff D, Dunnwald L, Gralow J, Ellis G, Schubert E, Tseng J, et al. Changes in blood flow and metabolism in locally advanced breast cancer treated with neoadjuvant chemotherapy. J Nucl Med 2003;44(11):1806–14.
Mankoff D, Dunnwald L, Gralow J, Ellis G, Charlop A, Lawton T, et al. Blood flow and metabolism in locally advanced breast cancer: relationship to response to therapy. J Nucl Med 2002;43(4):500–9.
Mullani N, Herbst R, Abbruzzese J, Charnsangavej C, Kim E, Tran H, et al. 9:00–9:15. Antiangiogenic treatment with endostatin results in uncoupling of blood flow and glucose metabolism in human tumors. Clin Positron Imaging 2000;3(4):151.
Ponto L, Madsen M, Hichwa R, Mayr N, Yuh W, Magnotta V, et al. Assessment of blood flow in solid tumors using PET. Clin Positron Imaging 1998;1(2):117–21.
Wilson C, Lammertsma A, McKenzie C, Sikora K, Jones T. Measurements of blood flow and exchanging water space in breast tumors using positron emission tomography: a rapid and noninvasive dynamic method. Cancer Res 1992;52(6):1592–7.
Innis RB, Cunningham VJ, Delforge J, Fujita M, Gjedde A, Gunn RN, et al. Consensus nomenclature for in vivo imaging of reversibly binding radioligands. J Cereb Blood Flow Metab 2007;27(9):1533–9.
Cunningham VJ, Jones T. Spectral analysis of dynamic PET studies. J Cereb Blood Flow Metab 1993;13(1):15–23.
Tawhai MH, Burrowes KS. Modelling pulmonary blood flow. Respir Physiol Neurobiol 2008;163(1–3):150–7.
Anonymous. Analytical Methods Committee: AMC Technical Brief. Tech. Rep.; Royal Society of Chemistry; 2003.
Ruotsalainen U, Raitakari M, Nuutila P, Oikonen V, Sipilä H, Teräs M, et al. Quantitative blood flow measurement of skeletal muscle using oxygen-15-water and PET. J Nucl Med 1997;38(2):314–9.
Anderson HL, Yap JT, Miller MP, Robbins A, Jones T, Price PM. Assessment of pharmacodynamic vascular response in a phase I trial of combretastatin A4 phosphate. J Clin Oncol 2003;21(15):2823–30.
Liao D, Johnson RS. Hypoxia: a key regulator of angiogenesis in cancer. Cancer Metastasis Rev 2007;26(2):281–90.
Turkbey B, Kobayashi H, Ogawa M, Bernardo M, Choyke PL. Imaging of tumor angiogenesis: functional or targeted? AJR Am J Roentgenol 2009;193(2):304–13.
Acknowledgements
GL and PP’s collaboration was supported by Cancer Research UK. We thank Terry Jones for helpful comments.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Laking, G., Price, P. Radionuclide imaging of perfusion and hypoxia. Eur J Nucl Med Mol Imaging 37 (Suppl 1), 20–29 (2010). https://doi.org/10.1007/s00259-010-1453-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-010-1453-x