
Abstract
Objective
The purpose of this work is to evaluate the normal meniscal and tibial dimensions in relation to age and gender in different children using conventional MRI sequences.
Materials and methods
Morphometric measurements of the menisci were retrospectively performed on knee MRIs of children (< 18 years). All knee MRIs over a 7-year period were collected. Exclusion criteria included: prior knee surgery or diseases involving the knee joint. A total of 186 children were included, 110 boys and 76 girls, with a mean age of 8.2 years (range, 0.3–17.8 years). Menisci and tibial measurement changes with age and gender as well as differences between the medial and lateral menisci were evaluated.
Results
The medial menisci measurements increased with age (p value < 0.001). The lateral menisci measurements increased with age (p value < 0.001), except for the coronal meniscal width (p = 0.084). Coronal and sagittal percentage of meniscal coverage of the tibia decreased with age (p < 0.001). Medial menisci have greater sagittal width and anterior horn height than lateral menisci (p value < 0.001). Lateral menisci are larger in their coronal width and height, and sagittal posterior horn height in comparison to medial menisci (p < 0.001).
Conclusions
Menisci increase in all dimensions in correlation with age; except in the coronal meniscal width, which is a useful dimension to diagnose discoid meniscus on MRI, based on this, it would seem that the currently published size criteria, based on adults, could be applicable to children. The tibia has a faster rate dimension increase in correlation with age in comparison to the menisci.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
There has been extensive scientific research to establish the anatomical, biomechanical, and functional importance of the meniscus within the knee joint [1]. The meniscus was initially described as a functionless remnant of leg muscles [2, 3] and total meniscectomies were performed indiscriminately for patients with meniscal injuries with adverse sequelae such as early osteoarthritis and ligamentous instability [4]. Currently, the importance of meniscal preservation and reconstruction during meniscal surgeries to avoid these complications is well known. There is also increased research interest towards tissue engineering and its potential for successful treatment of meniscal lesions [1].
Knowledge of the normal meniscal growth is essential for surgical planning of meniscal tears and the diagnosis of discoid meniscus in the pediatric population. Studies of the meniscal histological and immunohistochemical structure, blood supply, and biomechanics have been performed [2, 5,6,7]; however, magnetic resonance (MR) studies of the normal meniscal growth development are not available. The purpose is to evaluate the normal meniscal and tibial dimensions in relation to age and gender in different children using conventional MRI sequences and therefore to evaluate indirectly the meniscal and tibial growth.
Materials and methods
The study was approved by the Institutional Review Board (IRB) of our hospital, and was performed in compliance with the Health Insurance Portability and Accountability Act (HIPAA). We conducted a retrospective search to identify subjects who underwent knee MRI with normal lateral and medial menisci at our institution during a 7-year period. Inclusion criteria were patients less than 18 years of age with arthroscopic and/or MRI report of normal lateral and medial menisci. This search yielded 454 children. This included children with internal derangement of the knee. Exclusion criteria included prior knee surgery (n = 112) or diseases involving the knee joint (n = 156). We excluded patients with the following pathologies: inflammatory/infectious knee pathology such as osteomyelitis, synovitis, juvenile idiopathic arthritis or septic arthritis; primary or metastatic knee neoplasm; clinical suspicion for discoid meniscus; avascular necrosis; skeletal deformity involving the lower extremity; extensive local vascular malformation or neurofibroma; and congenital knee dislocation. The indications for the knee MRI included knee pain/swelling, superficial soft tissue inflammation and/or edema, clinical concern for osteomyelitis; popliteal cyst, trauma, and evaluation of cortical desmoid cysts of the distal femur.
Image analysis
All MR images were reviewed in a blinded and randomized order by a pediatric radiologist with 3 years of pediatric musculoskeletal experience and a radiology research assistant with 2 years of experience in pediatric musculoskeletal radiology. All images and measurements were evaluated in the institutional picture archiving and communication system (PACS) in a blinded fashion regarding patient’s name, age, arthroscopic findings and MRI indication. Thirty randomly selected cases were reviewed with a 4-month interval and intra-observer agreement was evaluated. The same 30 randomly selected cases were reviewed by another pediatric radiologist with 4 years of pediatric musculoskeletal experience and inter-observer agreement was calculated. The selection and definition of the measurements was performed in consensus by the two pediatric MSK radiologists and the research assistant. Parameters measured in the sagittal and coronal planes for each meniscus are presented in Table 1 and Fig. 1. We measured tibial coronal and sagittal width. For each knee, a total of 13 measurements were obtained. The tibial measurements include unossified epiphyseal cartilage in younger patients.

Example of the medial meniscal measurements on the (a) sagittal and (b) coronal planes in the right knee of an 11-year-old girl. a Sagittal proton density (PD) MR image in the mid-condylar slice showing the sagittal measurements of the medial menisci: meniscal sagittal width (1a + 1b), meniscal anterior horn height (2), meniscal posterior horn height (3), and medial tibial sagittal width (4). b Coronal fat-saturated PD MR image showing the coronal measurements of the medial menisci: meniscal coronal width (5), meniscal coronal height (6), and tibial coronal width (7). Measurements 1 to 6 were repeated for the lateral meniscus. Each child had a total of 13 measurements
We calculated the following parameters based on the coronal and sagittal measurements: (1) Coronal percentage of coverage of the lateral and medial meniscus on the tibial plateau ((Medial meniscal coronal width + Lateral meniscal coronal width /Tibial coronal width)×100); (2) Sagittal percentage of coverage of the medial meniscus on the medial tibial plateau ((Medial anterior meniscal sagittal width + Medial posterior meniscal sagittal width / Medial tibial sagittal width)×100); and (3) Sagittal percentage of coverage of the lateral meniscus on the lateral tibial plateau ((Lateral anterior meniscal sagittal width + Lateral posterior meniscal sagittal width / Lateral tibial sagittal width)×100).
MRI parameters
Dedicated knee MRI examinations were performed in a 1.5-T (73 patients, 39%) or 3.0-T (113 patients, 61%). A total of 136 studies (73%) were performed in our institution in Siemens MRI imaging units (Siemens Medical Solutions, Erlangen, Germany) using either an eight-channel knee coil (In vivo, Gainesville, FL, USA) or a 15-channel knee coil (Quality Electrodynamics, Mayfield Village, OH, USA). Fifty studies (27%) were performed with extra-institutional knee protocols.
For the measurements, we used an intermediate sequence (proton density, PD) with or without fat saturation. In the sagittal plane, the following sequences were used: PD (1.5 T: repetition time range ms/echo time range ms: 1500–4470/15–37; 3.0 T: 1500–3260/10–39) and a fat-saturated PD (1.5 T: 597–4560/12–48; 3.0 T: 4450/49). Sagittal slice thickness ranged from 1.5 to 4 mm. In the coronal plane, we used a fat-saturated PD (1.5 T: 2840–5400/14–37; 3.0 T: 2121–4500/9.7–49). Coronal slice thickness ranged from 2 to 4 mm. Various matrix sizes were used, depending on the clinical concern and the patient size; ranging from 320 to 448 × 256–384.
Statistical analysis
Descriptive statistics including mean, range, and standard deviation were used to summarize demographic information. The Shapiro–Wilk test was used to assess the distribution of data. To assess the differences of the measurements with correction for age and gender, hierarchical linear regressions were performed with each measurement value as the dependent variable, with age entered first, gender second, and the gender–age interaction term last. Paired t tests were used to evaluate differences between medial and lateral meniscal measurements, and between anterior and posterior horn heights. To evaluate inter-observer agreement and intra-observer agreement, intraclass correlation coefficient (ICC) with a two-way mixed model and with absolute agreement were performed. P values of less than 0.05 were considered significant. All analyses were performed using SPSS statistical software (IBM Corporation, Version 21.0.0, Armonk, NY, USA).
Results
The evaluable study population consisted of 186 knee MRIs (110 boys; 76 girls) (96 right; 90 left) with mean age (range ± SD) of 8.2 years (0.3–17.8 years ± 5.1 years) in boys and 10.1 years (1.3–17.6 years ± 4.6) in girls.
Arthroscopically proven normal lateral and medial menisci were identified in 92 subjects (49.5%) with mean age of 13.2 years (2.8–17.8 years ± 2.8 years). The mean time between MRI and arthroscopy was 0.2 years (2.4 months) (0.01–1.2 years ± 0.2 years). The arthroscopy indications were: osteochondritis dissecans (OCD) of the femoral condyle (n = 26; 28.3%); patellar dislocation (n = 26; 28.3%); ACL tear (n = 19; 20.7%); acute osteochondral injury (n = 9; 9.8%); tibial spine fracture (n = 6; 6.5%); symptomatic plica (n = 2; 2.2%); patella baja (n = 1; 1.1%); popliteal cyst (n = 1; 1.1%); bipartite patella (n = 1; 1.1%); and intra-articular cyst (n = 1; 1.1%). A total of 94 subjects (50.5%) with mean age of 4.9 years (0.3–10.0 years, ± 2.6 years) did not have knee arthroscopy, but had normal appearing menisci on MRI.
Medial menisci dimensions increase with age (p values < 0.001); however, the association with age and coronal width (transverse diameter) was weak (R2 = 0.087; p = 0.001). Lateral menisci dimensions also increased with age in all dimensions (p values < 0.001); except in the coronal width (transverse diameter) (p = 0.084; R2 = 0.016) (Table 2, Fig. 2).

Scatter plot shows the relationship of age with the medial and lateral meniscal width in the coronal plane
Tibial sagittal and coronal width in the medial and lateral side increased with age (p values < 0.001) (Table 2) (Fig. 3). As the rate of tibial growth was greater than the rate meniscal growth rate, the coronal and sagittal percentage of coverage of the menisci decreased with age (p values < 0.001).

Scatter plot showing the relationship of age with the medial (a) and lateral meniscal (b) width and the medial and lateral tibial width in the sagittal plane
Boys were significantly younger than girls in our study sample (p = 0.015); therefore, after controlling by age, boys had larger medial meniscal anterior horn height (p = 0.008), medial meniscal coronal width (transverse diameter) (p = 0.013), medial tibial sagittal width (AP diameter) (p = 0.005) and lateral tibial sagittal width (AP diameter (p = 0.002) (Table 2) (Fig. 4).

Scatter plot showing the age relation of the medial meniscal coronal width. Boys have greater medial meniscal coronal width in comparison to girls
Table 3 shows the differences between medial and lateral measurements. Tibial sagittal width was not significantly different between the medial and lateral side (p = 0.176). Medial menisci had significantly larger sagittal width and anterior horn height, and sagittal percentage of coverage in comparison to lateral menisci (p values < 0.001). Lateral menisci were significantly larger in their coronal width and height, sagittal posterior horn height, and the coronal percentage of coverage in comparison to medial menisci (p values < 0.001).
In the medial meniscus, the anterior horn height did not differ from the posterior horn height (p = 0.065). In the lateral meniscus, the posterior horn height was significantly larger than the anterior horn height (p < 0.001) (Fig. 5).

Scatter plots of the medial and lateral meniscal anterior and posterior horn size. Scatter plot of the medial meniscus shows that the anterior horn height of the medial meniscus did not differ with the posterior horn height (a). Scatter plot of the lateral meniscus shows that the posterior horn height is larger than the anterior horn height in the lateral meniscus (b)
The mean ICC of the intra-observer agreement was 0.87; and the mean ICC of the inter-observer agreement was 0.91. Children with arthroscopy correlation were older than children with only MRI examination with a mean age of 13.2 years and 4.9 years, respectively (p < 0.001).
Discussion
There is limited data in the literature regarding the normal growth of both medial and lateral meniscus based on MRI examinations. The typical description of the size and shape of the medial meniscus in comparison to the lateral meniscus is that “the medial meniscus is larger, has a wider posterior horn, and is more “open” towards the intercondylar notch” [8]. Based on our findings, this statement should be analyzed carefully, as it depends on the orthogonal plane in which the meniscus is evaluated. The medial meniscus in the sagittal plane has a larger width with a larger anterior horn height, and therefore has a higher percentage of tibial coverage in the sagittal plane in comparison to the lateral meniscus; however, the lateral meniscus is larger in all the measurements on the coronal plane. The understanding of the normal meniscal growth pattern and size criteria is important as a diagnostic tool and as a primary point of further studies.
Menisci increase in size in all dimensions, in relationship to age, except in the coronal meniscal width (Fig. 6), which is the principal dimension to diagnose discoid meniscus on MRI. The MRI diagnosis of discoid meniscus in children is based on adult’s studies [9,10,11]; there is little data in the literature regarding the quantitative MR diagnostic criteria for discoid meniscus in children [12,13,14]. It is important to notice that the current diagnosis of discoid meniscus is made by a combination of clinical examination, and abnormal meniscal shape and size in the sagittal and coronal planes. The MRI diagnostic criteria of discoid menisci in children have not been established in children, for that reason, the discrimination between a large normal meniscus and a true discoid meniscus is a diagnostic challenge. However, given that the coronal meniscal width measurement does not change with age, it would seem that the currently published size criteria, based on adults [9,10,11], could be applicable to children.

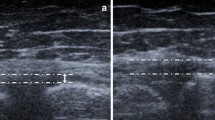
Coronal T1W images of the knees of a 7-month-old male (a) and a 17-year-old male (b). Note that there is no significant growth in the coronal meniscal width
In our study, the meniscal coverage of the tibial plateau in the coronal and the sagittal plane of both menisci decrease with age; this may be due to different growth rates between the tibia and the menisci. This is a potential pitfall, as during the evaluation of coronal MRI images, the mid-portions of the menisci may look proportionally smaller in older children/adolescents when compared to younger children, and therefore, physiologically larger menisci can potentially be confused with discoid menisci in these younger children. The disproportionate measurements of meniscal tibial coverage with age found in this study do not agree with a histological study in 28 cadaveric children, aged 3 months to 14 years, that showed a relative uniform ratio of growth between the menisci and the tibia, with a meniscal-plateau ratio not varying with age [5]. The reason for this discrepancy may be related to differences in technique regarding meniscal and tibial measurement. Clark et al. [5] measured the calculated meniscal area and the coverage of the respective tibial plateau; in comparison to our study, we measured the meniscal diameter in a two-dimensional technique; in addition, we combined the tibial measurement in the coronal plane rather than differentiating between medial and lateral tibial measurements.
Meniscal injuries have been increasing in the pediatric population, especially in adolescents, due to the increase in the number of children participating in organized and non-organized sports and increase in the prevalence of obesity in the pediatric population. MRI is the modality of choice in the evaluation of pediatric and adult patients with suspected meniscal pathology. In the most recent pediatric series, MRI showed an accuracy for detecting lateral and medial meniscal tear of 82 and 90%, respectively [12]. Open or arthroscopic meniscal surgeries are currently focused on preservation of the meniscal shape and function. There is a correlation between the amount of resected meniscal tissue and the development of osteoarthritic changes [15]. There are multiple techniques of meniscal repair with suturing, bioabsorbable implants, and more recently the use of meniscal allografts [16, 17]. MRI has been used as part of the algorithm to determinate the appropriate size for selecting meniscal allografts [18,19,20]. Knowledge of the meniscal growth and their expected size for age is important to improve these new surgical approaches and reduce the risk of early degenerative changes of the joint; additionally, the correlation between meniscal and tibial growth and the difference between medial and lateral meniscal dimensions play a relevant role in the determination of the meniscal allograft size [19, 21].
Approximately 50% of children included in this study had arthroscopically proven normal menisci. Younger children did not have arthroscopy correlation as the principal indications for arthroscopy in younger children are infection, and primary or metastatic knee neoplasms; these pathologies were excluded from our study given the likelihood of affecting vascular supply of the knee and therefore induce or delay skeletal growth. In comparison, in older children the principal indications for arthroscopy are trauma and OCD.
This study has the inherent limitations of a retrospective study, including variability in knee MRI protocols, particularly in slice thickness and although there was no known meniscal abnormality in the included subjects, they were not free of disease; however, we excluded all the possible factors that we thought could have an effect on meniscal growth. We did not analyze the meniscal signal in children because it is out of the scope of the study and it has been previously described [22]; and no patients with meniscal tears were included in our study. Although unlikely, not having the same protocol for all subjects may affect the measurements of the different components of the menisci and tibial plateau; however, we used intermediate sequences (PD and PD fat-saturated) for our cases; these sequences are preferred for the evaluation of meniscal margins and meniscal pathology [15]. Finally, knee rotation could potentially be a source of variability in the provided measurements; however, to decrease this possible variability, we chose consistent measurement locations based on the established knee landmarks (Table 1); in addition, all knee MRI studies performed at our institution are performed using a 15–30-degree knee flexion.
Conclusions
Menisci grow in all dimensions; except in the coronal meniscal width, which is a key dimension to diagnose discoid meniscus on MRI; based on this, it would seem that the currently published size criteria, based on adults, could be applicable to children. The tibia has a faster rate of growth in comparison to the menisci, which is important for image interpretation in younger children, and surgical planning of meniscectomies in children.
References
Makris EA, Hadidi P, Athanasiou KA. The knee meniscus: structure-function, pathophysiology, current repair techniques, and prospects for regeneration. Biomaterials. 2011;32:7411–31.
Arnoczky SP, Warren RF. Microvasculature of the human meniscus. Am J Sports Med. 1982;10:90–5.
Sutton J. Ligaments. their nature and morphology. London: M. k. Lewis; 1897.
Gray JC. Neural and vascular anatomy of the menisci of the human knee. J Orthop Sports Phys Ther. 1999;29:23–30.
Clark CR, Ogden JA. Development of the menisci of the human knee joint. Morphological changes and their potential role in childhood meniscal injury. J Bone Joint Surg Am. 1983;65:538–47.
McDevitt CA, Webber RJ. The ultrastructure and biochemistry of meniscal cartilage. Clin Orthop Relat Res. 1990:8–18.
Petersen W, Tillmann B. Age-related blood and lymph supply of the knee menisci. A cadaver study. Acta Orthop Scand. 1995;66:308–12.
Fox MG. MR imaging of the meniscus: review, current trends, and clinical implications. Radiol Clin N Am. 2007;45(1033–1053):vii.
Silverman JM, Mink JH, Deutsch AL. Discoid menisci of the knee: MR imaging appearance. Radiology. 1989;173:351–4.
Araki Y, Yamamoto H, Nakamura H, et al. MR diagnosis of discoid lateral menisci of the knee. Eur J Radiol. 1994;18:92–5.
Samoto N, Kozuma M, Tokuhisa T, et al. Diagnosis of discoid lateral meniscus of the knee on MR imaging. Magn Reson Imaging. 2002;20:59–64.
Gans I, Bedoya MA, Ho-Fung V, et al. Diagnostic performance of magnetic resonance imaging and pre-surgical evaluation in the assessment of traumatic intra-articular knee disorders in children and adolescents: what conditions still pose diagnostic challenges? Pediatr Radiol. 2014.
Stark JE, Siegel MJ, Weinberger E, et al. Discoid menisci in children: MR features. J Comput Assist Tomogr. 1995;19:608–11.
Connolly B, Babyn PS, Wright JG, et al. Discoid meniscus in children: magnetic resonance imaging characteristics. Can Assoc Radiol J. 1996;47:347–54.
Anderson MW. MR imaging of the meniscus. Radiol Clin N Am. 2002;40:1081–94.
Rath E, Richmond JC. The menisci: basic science and advances in treatment. Br J Sports Med. 2000;34:252–7.
Riboh JC, Tilton AK, Cvetanovich GL, et al. Meniscal allograft transplantation in the adolescent population. Arthroscopy. 2016;32(1133–1140):e1131.
Donahue TL, Hull ML, Howell SM. New algorithm for selecting meniscal allografts that best match the size and shape of the damaged meniscus. J Orthop Res. 2006;24:1535–43.
Stone KR, Freyer A, Turek T, et al. Meniscal sizing based on gender, height, and weight. Arthroscopy. 2007;23:503–8.
Elsner JJ, Portnoy S, Guilak F, et al. MRI-based characterization of bone anatomy in the human knee for size matching of a medial meniscal implant. J Biomech Eng. 2010;132:101008.
McDermott ID, Sharifi F, Bull AM, et al. An anatomical study of meniscal allograft sizing. Knee Surg Sports Traumatol Arthrosc. 2004;12:130–5.
Francavilla ML, Restrepo R, Zamora KW, et al. Meniscal pathology in children: differences and similarities with the adult meniscus. Pediatr Radiol. 2014;44:910–25 quiz 907-919.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Bedoya, M.A., Barrera, C.A., Chauvin, N.A. et al. Normal meniscal dimensions at different patient ages—MRI evaluation. Skeletal Radiol 48, 595–603 (2019). https://doi.org/10.1007/s00256-018-3072-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-018-3072-8