
Abstract
Objective
To describe a technique and its clinical applications of three-dimensional ultrasonography to type VI and VII radial polydactyly for identification of potential muscular anomalies.
Materials and methods
Ultrasonographic examinations were performed at an out-patient department without sedation or an operative room prior to surgery. The palm was scanned in the transverse direction using a 18-MHz linear transducer under speed regulation at 3 mm/s. Sequential images acquired at 0.2 mm intervals were converted into volume data. After validation of the technique, patients with a radial polydactyly in association with triphalangism (type VII) or with polydactylies of metacarpal duplication (type VI) were included for the examination.
Results
Five hands of five patients, one with type VI and four with type VII, were included the study. All the patients were male and the ages at examination ranged from 7 months to 2 years. Of the five patients, four examinations were performed at an out-patient department without sedation and one was under anesthesia just prior to surgery. The muscular abnormalities identified were mal-positions of the thenar muscles in a type VI case and a deficiency of the abductor pollicis brevis muscle in a type VII case with a delta phalanx in the ulnar part.
Conclusion
Three-dimensional ultrasound technique could be an aid to plan strategies in radial polydactyly if intrinsic muscular anomalies are suspected to be involved.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The principle of surgery for radial polydactyly is removal of the hypoplastic part and reconstruction of the retained component. Stabilizing the joints, aligning the bones, and repositioning the muscles are the essential elements of the reconstruction; however, intrinsic muscle anomalies can complicate the reconstruction. Especially in radial polydactylies with triphalangism (Wassel’s type VII), the involvement of thenar hypoplasia has been indicated [1, 2]. Additionally, metacarpal duplications (Wassel’s type VI) are frequently present in association with hypoplastic metacarpal [3–5]. Advance knowledge of potential muscular abnormalities is of use to surgeons; nevertheless, requirement of sedation limits clinical uses of scanning imaging modalities for infants. By recent technological advances of high-frequency transducers, the applicability of ultrasonography to superficial pathologies has been heightened in the pediatric orthopedic field. Acknowledging the easy maneuverability and the minimum invasive nature of ultrasonography, we have applied it to infants’ superficial conditions; however, on-site two-dimensional (2D) visualization limited total anatomical identifications. Since 2014, we have employed a three-dimensional (3D) imaging technique of ultrasonography to resolve the limitation. The purpose of this paper is to describe the technique and its clinical applications in type VI and VII radial polydactylies.
Materials and methods
This study was approved by the ethical committee of our institution and performed in compliance with the Declaration of Helsinki. To establish the technique to visualize the thenar muscular conditions, healthy volunteers of infants who had no histories of hand traumas or hand-related congenital conditions were recruited. After confirming the utility of the technique, we applied the technique to patients with radial polydactyly associated with triphalangism or duplications of metacarpal with/without a narrow first web. The patients’ families received an explanation regarding the examination and surgery, and a written informed consent form was obtained. All the subjects had health conditions that did not prevent the use of the technique. The examinations were performed at an outpatient department without sedation or an operative room prior to surgery under general anesthesia. The maximum repetition of the trials of examination was limited to three times when the examination was performed without sedation.
3D ultrasound technique
An ultrasound instrument (Preirus; Hitachi Aloca Medical Co., Ltd., Tokyo, Japan) fitted with an 18-MHz linear array transducer, was used for the examination. The transducer was set longitudinally to scan the palm in the transverse direction. A polymer gel pad (Sonagel; Takiron Co., Ltd., Osaka, Japan), 5 mm in thickness, was positioned between the transducer and the skin to create a flat surface to be scanned smoothly. The palm was scanned transversely under regulated scanning speed at 3 mm/s by an electronic-controlled mover. Consecutive images at 0.2-mm intervals were converted into volume data using imaging software (Volume Extractor 3.0; i-Plants Systems Co., Ltd., Iwate, Japan), enabling automatic multi-planar visualization composed of three orthogonal sections. The scanning and imaging processing were performed bilaterally for comparison. The reading comprised of three steps. Firstly, coronal sections were imaged layer by layer to ascertain the gross anatomy of the hand. Next, the multi-planar views were used for individual anatomical identifications. Lastly, freely sectioned reconstructed images were obtained to be compared with those of the contralateral side. The agreements of identified findings were verified at the review meeting of the Department for each of the cases.
Results
The normal anatomy of the thenar muscles is illustrated in Fig. 1.The preliminary studies using the volunteers’ hands revealed the high spatial resolution of the thenar muscles (Fig. 2). The muscles at the thenar region, visualized in dark gray to black tone with some striations, were well differentiated from the subcutaneous fat layer toned in gray, the volar cortical surfaces of the metacarpal in white, and the unossified epiphyses in deep black. The light gray tone of the septal fascial planes facilitated the individual anatomical identifications of the muscles. Although the flexor pollicis longus tendon showed a multi-striated appearance, it was not delineated distally from the surrounding connective tissues because of the similarity of their tonal levels.

Schematic illustration of the normal anatomy of the thenar muscles (a superficial layer, b middle to deep layer). The opponens pollicis (in the middle layer) is covered by two superficial muscles: the abductor pollicis brevis radially and the superficial head of the flexor pollicis brevis ulnarly. The flexor pollicis longus tendon is a landmark indicating the intermuscular plane between the superficial and the deep head of the flexor pollicis brevis. The adductor pollicis locates distally in the deep layer. The adductor pollicis inserts into the ulnar sesamoid, whereas the abductor pollicis brevis and the flexor pollicis brevis inserts into the radial sesamoid. Colored stripes or slashes in each muscle indicate the direction of its fibers

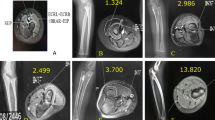
Three-dimensional multi-planar views of ultrasonography composed of three orthogonal sections showing the anatomies of the thenar regions of a healthy 5-year-old infant. The coordinate of each sectional plane can be adjusted to show the anatomies of interest (a superficial, b middle to deep layer). Also, the cross sections are observed from any different viewpoints by flipping and rotating them freely (a–b the volar viewpoint, c–d the radial viewpoint), thereby precise anatomical identifications can be facilitated. Red arrows indicate the directions of the adjustment of coordinate. Yellow arrows indicate flip or rotation of the cross sections
Five hands of five patients, one with type VI and four with type VII, were included the study. All the patients were male and the ages at examination ranged from 7 months to 2 years. Of the five patients, four were examined at an outpatient department and one was at an operative theater. The ultrasound examinations revealed muscular abnormalities in two hands of two patients. No muscular anomalies were detected in the other three patients. The abnormalities included mal-positions of the thenar muscles in the patient with type VI and a deficiency of the abductor pollicis brevis (APB) muscle in the patient with type VII.
Case reports
Case 1
A 7-month-old boy presented with type VII polydactyly of the right hand (Fig. 3). X-rays revealed duplication at the metacarpophalangeal joint in combination with a delta middle phalanx of the radial component. The first metacarpal showed a bi-condylar configuration distally. The radial thumb was ulnarly angulated at the distal interphalangeal joint but the ulnar thumb was aligned straight. An ultrasonographic examination was performed without sedation at an outpatient department. After volume data was obtained, coronal sections at different levels were reconstructed to visualize both the superficial and the middle to deep layers of the thenar muscles (Fig. 4). No deficiency or hypoplasia of the thenar muscles was detected.

The right hand of a 7-month-old boy with radial polydactyly of metacarpal duplication with triphalangism of the radial thumb (case 1). a A volar view, b An X-ray. Note that the thenar eminence seems developed normally (arrowheads). A delta phalanx is shown in the radial duplicated component (arrow). The section scanned by ultrasonography is indicated by the dotted lines

Three-dimensional reconstructions of ultrasonography (a case 1, b normal). Consecutive images in the sagittal plane were stacked transversely to provide parallelepiped-shaped volume data (central small images). Two reconstructed coronal sections (the images in the red and the green sections) show the superficial and the deep layers of the thenar muscles, respectively
Case 2
A 1-year-old boy presented with a proximal phalangeal duplication of the right hand (Fig. 5). He had no family members with hand anomalies. X-rays showed a delta middle phalanx of the ulnar component, indicating type VII polydactyly. The ulnar thumb angulated radially at the proximal interphalangeal joint. The radial part was undeveloped distally, showing no nail apparatus. The thenar eminence seemed hypoplastic radially, and the first web space was narrow. An ultrasonographic examination was performed at an outpatient department when the boy was sleeping. Multi-planar views of ultrasonography revealed a deficiency of the APB muscle (Fig. 6). Surgical exploration confirmed the finding. An on-top transposition in combination with shortening and fusions was performed. The muscular deficiency was not treated simultaneously. If dysfunction in opposition was substantial during follow-up, an additional muscle transfer would have to be considered.

The right hand of a 1-year-old boy with radial polydactyly of proximal phalangeal duplication with triphalangism of the ulnar thumb (case 2). a A volar view, b An X-ray. A delta phalanx is shown in the ulnar duplicated component (arrow). Note that the thenar eminence seems undeveloped radially (arrowheads). The section scanned by ultrasonography is indicated by the dotted lines

Multi-planar view of 3D ultrasonography (a–b case 2, c–d normal). Both the coronal sections of the volar viewpoint (a, c) and the axial section of the radial viewpoint (b, d) reveal a deficiency of the abductor pollicis brevis muscle. Note that there is no muscle belly on the radial side of the first metacarpal—red arrow (a), red dotted lines (b). 1st, 2nd, and 5th MC: the first, second, and fifth metacarpal bone, respectively. Green planes (a, c) indicate the locations of the axial sections (b, d), respectively. Yellow arrows indicate flip or rotation of the cross sections
Case 3
A 2-year-old boy underwent surgery for type VI polydactyly of the right hand (Fig. 7). The radial component of the duplicated thumb, arising transversely from the metacarpal joint, was ulnarly angulated and hypoplastic. The ulnar component aligned straight in the slight adducted position. The thenar eminence seemed undeveloped and the first web showed mild adduction contracture. X-rays did not reveal metacarpal hypoplasia or any evidence of triphalangism. An ultrasonographic examination was performed at an operative room prior to the surgery. Multi-planar views revealed locational abnormalities of the intrinsic muscles (Fig. 8). The APB and flexor pollicis brevis (FPB) muscles, located more proximally than is normal, ran transversely with insertion into the base of the metacarpal of the radial component. The transverse head of the adductor pollicis muscle ran proximally over the condyle of the metacarpal of the ulnar component with insertion into the ulnar aspect of the metacarpal of the radial component. Surgical exploration confirmed these findings. After resection of the radial part, the residual thenar muscles were transferred to the ulnar component by detachment with a fascial extension, and attachments to the proximal phalanx base.

The right hand of a 2-year-old boy with a metacarpal duplication of the thumb (case 3). a A volar view, b An X-ray. Note the undeveloped thenar eminence. The section scanned by ultrasonography is indicated by the dotted lines

Multi-planar views of three-dimensional ultrasonography (a–b case 3, c–d normal). The coronal sections of the volar viewpoint (a, c) reveal anomalous insertions of the abductor pollicis brevis and flexor pollicis brevis muscles into the radial metacarpal base (red circle). Normally, these muscles insert into the radial sesamoid of the metacarpophalanangeal joint of the first ray (yellow circle). b, d Multi cross-sections of the dorsal, ulnar viewpoint. Note that the adductor muscle shows an abnormal insertion into the metacarpal base of the radial duplicated thumb (blue circle) instead of that of the ulnar component. 1st MC, the first metacarpal; 1st MC (r) and 1st MC (u), the first metacarpal of the radial and ulnar component of the duplicated thumb, respectively
Discussion
In the present study, the 3D imaging technique of ultrasonography successfully visualized intrinsic muscular anomalies. The patient with a type VI polydactyly (case 3) showed anomalous insertions of the thenar muscles into the metacarpal base. Consequently, we planned a procedure utilizing the residual muscular functions. Technically, the metacarpal transposition procedure has been proposed for type VI or type VII polydactyly, especially when the radial part is distally hypoplastic, and the ulnar part is undeveloped proximally but well-formed distally [3, 4]. In our case, we did not perform the transposition procedure because the whole ulnar part was well developed and narrowing of the first web was not so severe. The ultrasonographic findings led us to accomplish muscle transfer in combination with a fascial extension. Also, the patient with a radial polydactyly with triphalangism in the ulnar thumb (case 2) showed a deficiency of the APB muscle, leading us to consider the necessity of an additional muscular reconstruction, whereas the patients with a radial polydactyly with triphalangism in the radial thumb as in case 1 showed no hypoplasia or deficiency of the thenar muscles, indicating radial ablation with joint reconstruction including the APB reattachment.
Etiological association between radial polydactyly and thenar hypoplasia has been suggested, especially in polydactylies in combination with triphalangism. The relationship between radial polydactyly and triphalangism remains unestablished, but genetic association of these two conditions has been suggested by many authors [1, 6]. Graham et al. reported four hereditary cases of polydactyly associated with thenar hypoplasia, suggesting variability of genetic expression ranging from thumb hypoplasia to triphalangism or duplication of the thumb [6]. Whether triphalangism occurs genetically or not, its association with thenar hypoplasia has been indicated. Hovius et al. documented that the involvements of articular or muscular hypoplasia, as well as insufficiency of the first web, can be present in triphalangism, therefore sufficient knowledge of the underlying anatomic differences is required [2]. The relationship among radial polydactyly, triphalangism, and thenar hypoplasia is confusing, and clinical differences between hereditary and sporadic cases are still unclear; however, it might be meaningful to consider potential intrinsic anomalies when surgeons treat type VII polydactyly. Similar to the clinical manifestations of triphalangism, metacarpal involvements of radial polydactyly are frequently present in association with hypoplastic metacarpal and/or adduction contracture of the first web [3–5]. This association implies the possibility of thenar hypoplasia or muscular anomalies in this condition.
Potential intrinsic anomalies in radial polydactyly have been of concern to surgeons; nonetheless, literature regarding such soft–tissue conditions has been sparse, possibly because imaging modalities safely applicable for infants are limited. Magnetic resonance imaging (MRI) has high spatial resolutions for soft parts. Andreisek et al. employed MRI to assess intrinsic muscular pathologies of adults’ hands [7]. Belouli et al. also utilized MRI to visualize thenar anomalies of triphalangeal thumb [8]. These studies demonstrated the feasibility of MRI in the verification of muscular anomalies of the hand; however, the need of sedation during a MRI scan limits its routine clinical uses. Also, computed tomography (CT) has a constant issue of radiation exposure. In contrast, ultrasound is safe and less expensive (it costs less than one-fifth of MRI scan fees in our country). Moreover, its fast activation and transportability enables bed-side use; nonetheless, some disadvantages minimize its reliability as a diagnostic tool as follows: localized 2D images limit objectivity; additional images from different viewpoints are not obtainable afterwards; infant movements limit the examination time, which can result in an incomplete investigation. To resolve these disadvantages, the 3D visualization technique was employed in the present study.
The methodology used in the study was based on the traditional concept of 3D reconstruction [9]. In the concept, volume data is acquired by mechanical horizontal sweeping of a linear array transducer. Recent 3D/four-dimensional (4D) ultrasound probe has been specifically designed for anomaly scanning of fetus or neonate [10, 11]. To visualize superficial pathologies precisely, we revived the traditional conception for 3D reconstructions. Volk et al. performed volumetric evaluations of the facial muscles in facial nerve palsies using a 3D ultrasonography based on the same conception [12]. In the present study, the 3D visualization successfully facilitated anatomical identifications using multi-planar observations.
The limitation of the technique is three-fold. The first is the lack of dynamic information of the muscles. The technique reveals the muscle in situ, not in function. Thus if any insufficiencies are suspected of ultrasound, manual checking is required intraoperatively. Additionally, intraoperative inspection could be needed for bone and joint conditions. The second is the duration of the examination time. It takes around 15 s to scan the whole thenar portion, but this time frame may only be available if the infant does not experience stress. The examination at an operative room prior to surgery would be a reliable alternative as long as speedy 3D processing is available. Progress in the technology of linear 3D/4D transducer will offer fast and fine visualization for superficial pathologies in the near future. The third is the limited information on false positives or negatives of the technique. We recognize that true diagnostic accuracy of the technique is judged after complete confirmation of the correlations or inconsistencies between the ultrasonographic and the operative findings; however, extensive exposures of the volar and ulnar sides were avoided in consideration of the less-invasive priority of surgeries.
In conclusion, we believe that the 3D imaging technique of ultrasonography could be an aid to plan strategies in radial polydactyly surgeries, especially when muscular anomalies are suspected to be involved. Further investigations would clarify the whole picture of the potential intrinsic muscle anomalies in a variety of radial polydactylies.
References
Miura T, Nakamura R, Horii E, et al. Three cases of syndactyly, polydactyly, and hypoplastic triphalangeal thumb: (Haas’s malformation). J Hand Surg [Am]. 1990;15:445–9.
Hovius SE, Zuidam JM, de Wit T. Treatment of the triphalangeal thumb. Tech Hand Up Extrem Surg. 2004;8:247–56.
Ogino T, Ishii S, Takahata S, Kato H. Long-term results of surgical treatment of thumb polydactyly. J Hand Surg [Am]. 1996;21:478–86.
Tonkin MA. Thumb duplication: concepts and techniques. Clin Orthop Surg. 2012;4:1–17.
Iba K, Wada T, Yamashita T. Atypical thumb polydactyly with duplicated metacarpal bone: a report of 2 cases. Ann Plast Surg. 2013;70:38–41.
Graham Jr JM, Brown FE, Hall BD. Thumb polydactyly as a part of the range of genetic expression for thenar hypoplasia. Clin Pediatr (Phila). 1987;26:142–8.
Andreisek G, Kilgus M, Burg D, et al. MRI of the intrinsic muscles of the hand: spectrum of imaging findings and clinical correlation. AJR Am J Roentgenol. 2005;185:930–9.
Belouli K, Beer GM, Burg D, et al. Verification of thumb-specific muscles in a triphalangeal thumb with magnetic resonance imaging. Handchir Mikrochir Plast Chir. 2005;37:207–9.
Fenster A, Lee D, Sherebrin S, et al. Three-dimensional ultrasound imaging of the vasculature. Ultrasonics. 1998;36:629–33.
Bennasar M, Martínez JM, Gómez O, et al. Intra- and interobserver repeatability of fetal cardiac examination using four-dimensional spatiotemporal image correlation in each trimester of pregnancy. Ultrasound Obstet Gynecol. 2010;35:318–23.
Chapman T, Mahalingam S, Ishak GE et al. Diagnostic imaging of posterior fossa anomalies in the fetus and neonate: part 1, normal anatomy and classification of anomalies. Clin Imaging. 2014.39(1):1–8.
Volk GF, Pohlmann M, Finkensieper M, et al. 3D-Ultrasonography for evaluation of facial muscles in patients with chronic facial palsy or defective healing: a pilot study. BMC Ear Nose Throat Disord. 2014;14:4.
Acknowledgements
We received a research grant from Fujiwara Memorial Foundation to make an instrument involved in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflict of interest.
Rights and permissions
About this article

Cite this article
Saito, S., Ueda, M., Takahashi, N. et al. Three-dimensional ultrasonography for visualization of muscular anomalies in type VI and VII radial polydactyly. Skeletal Radiol 45, 541–547 (2016). https://doi.org/10.1007/s00256-015-2271-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-015-2271-9