
Abstract
Objective
Diffusion-weighted imaging (DWI) provides essential information regarding tumor composition, such as cellularity and/or perfusion. DWI is helpful in distinguishing between malignant and benign lesions. Malignant intramuscular/soft tissue lesions consist of a wide spectrum of tumors that have different cell counts and matrix. It is presumed that these different tumors have different DWI findings and have different apparent diffusion coefficient (ADC) values. The aim of this study was to analyze DWI findings of different intramuscular malignancies in a multicentric study by using a standardized DWI protocol, and to compare the ADC values acquired.
Materials and methods
The data banks of four radiology departments were screened retrospectively for malignant intramuscular tumors. Only lesions that were investigated by MRI (with a 1.5-T scanner) using DWI (multishot EPI sequence with b values of 0 and 1,000 s/mm2) were included in the study. Overall, 51 patients (28 women, 23 men; mean age 58.8 ± 16.1 years) with 57 different malignant intramuscular lesions were collected. In every case apparent diffusion constant (ADC) maps were calculated. In 14 patients muscle lymphoma, 11 patients intramuscular metastases from different primary tumors, and in 26 cases several muscle sarcomas were identified.
Results
The mean ADC value of the estimated lesions was 1.24 ± 0.53 × 10−3 mm2s−1, median value, 1.11 × 10−3 mm2s−1, range, 0.54–2.9 × 10−3 mm2s−1. The mean ADC value in muscle metastases was 1.28 ± 0.24 × 10−3 mm2s−1, in muscle lymphoma 0.76 ± 0.14 × 10−3 mm2s−1, and in muscle sarcomas 1.82 ± 0.63 × 10−3 mm2s−1. Muscle lymphoma showed statistically significant lower ADC values in comparison to muscle metastases (p = 0.01) and muscle sarcoma (p = 0.001). There was no significant differences between ADC values in muscle metastases and sarcomas (p = 0.48). ADC values in muscle lymphoma were homogeneous with less inter-patient variability and were within a relatively close range. Muscle sarcomas had a broad range of ADC values.
Conclusion
Intramuscular malignant lesions had different ADC values on DWI. 22.8 % of the tumors analyzed had low ADC values, 26.3 % moderate, and 50.9 % high ADC values. Muscle lymphoma had statistically significantly lower ADC values in comparison to muscle metastases and sarcomas. Muscle sarcomas presented with a broad range of ADC values.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Diffusion-weighted imaging (DWI) is an imaging technique that provides essential information regarding tumor composition, such as cellularity and/or perfusion [1–4]. Several reports showed significant correlation between DWI and cell count in different malignancies [4, 5]. Furthermore, DWI is helpful in distinguishing between malignant and benign lesions [1, 2, 6, 7]. According to the literature, malignant tumors have lower apparent diffusion coefficient (ADC) values than benign lesions [1–3]. For example, it has been shown that benign breast lesions had statistically significantly higher ADC values in comparison to breast cancer [3]. In addition, DWI can differentiate between metastatic and nonmetastatic lymph nodes [6].
Similar results were also reported in soft tissue/muscle neoplasms [1, 7].
However, malignant muscle/soft tissue lesions consist of a wide spectrum of tumors that have different cell counts and matrix. Therefore, it is presumed that these different tumors have different DWI findings and different ADC values. In fact, the reported data confirm this hypothesis (Table 1). As shown in Table 1, malignant intramuscular lesions have a broad spectrum of ADC values, ranging from 0.46 × 10−3 mm2/s in lymphomas to 1.99 × 10−3 mm2/s in muscle metastases [1, 8–14]. In addition, the mean ADC values in sarcomas are also different, varying from 0.88 × 10−3 mm2/s to 1.7 × 10−3 mm2/s [1, 7–10]. In the reported studies, different MR protocols and different DWI data acquisition were used. For example, Einarsdóttir et al. used b values of 0 and 600 s/mm2 [8], Genovese et al. utilized b values of 50 and 800 s/mm2 [9], and in another study b values were 0 and 701 s/mm2 [7].
The aim of this study was to analyze the DWI findings of different intramuscular malignancies in a multicentric study by applying a standardized DWI protocol and to compare the ADC values acquired.
Materials and methods
Patients and imaging
The data banks of five radiology departments (Department of Radiology, Martin-Luther-University Halle-Wittenberg, Germany; Department of Radiology, Kurume University School of Medicine, Japan; Department of Diagnostic Radiology, Mansoura Faculty of Medicine, Mansoura, Egypt; Department of Imaging, Dana-Farber Cancer Institute and Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA) were screened retrospectively for malignant muscle tumors. Approval of the institutional review board was obtained in all the contributing institutions with a waiver for informed consent. Only lesions that were investigated by MRI (1.5 T scanner) by using DWI (multishot EPI sequence with b values of 0 and 1,000 s/mm2) were included in the study. The technical parameters were as follows: TR/TE: 2,200-10,000/61–120 ms; acquisition matrix: 128–256 × 83–512 pixels; section thickness 5–6 mm.
Overall, 51 patients (28 women, 23 men; mean age 58.8 ± 16.1 years, range, 22–86 years) with 57 different malignant intramuscular lesions were collected. The histopathology of all the tumors was confirmed as part of routine oncology care.
In every case apparent diffusion constant (ADC) maps were calculated according to the following equation [7]:
where S0 and S1000 represent the signal intensities of corresponding pixels of the b = 0 and b = 1,000 images. The section with the largest diameter of the investigated lesions was selected for ADC calculation. The ADC value was classified in to low, moderate, and high using the cutoffs of <0.8, 0.8–1.1, and >1.1 × 10−3 mm2s−1 respectively.
Statistical analysis
For statistical analysis the SPSS statistical software package was used (SPSS 17.0; SPSS, Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables as absolute and relative frequencies. Analyses of ADC values were performed by ANOVA and subsequent post-hoc tests. P values were adjusted for multiple testing (Bonferroni correction). The significance level was chosen to be 0.05.
Results
In 14 patients muscle lymphoma, in 11 patients intramuscular metastases from different primary tumors, and in 26 cases several muscle sarcomas were identified. The mean ADC value of the estimated lesions was 1.24 ± 0.53 × 10−3 mm2s−1, median value, 1.11 × 10−3 mm2s−1, range, 0.54–2.9 × 10−3 mm2s−1 (Figs. 1–3). In 22.8 % the ADC values were low, in 26.3 % moderate, and in 50.9 % high.

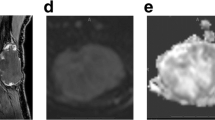
Imaging findings of a muscle metastasis (arrows) in known renal cell carcinoma. a T2-weighted image shows a large mass within the right erector spine muscle. b Apparent diffusion coefficient (ADC) map. The calculated ADC value is 1.4 × 10−3 mm2s−1

Intramuscular manifestation of a large B cell lymphoma (arrows) within the biceps brachii muscle. a T2-weighted image of the lesion. b ADC map. The calculated ADC value is 0.9 × 10−3 mm2s−1

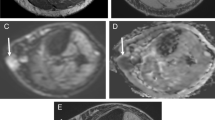
Intramuscular malignant peripheral nerve sheath tumor (arrows) in the right quadriceps muscle. a T2-weighted image of the tumor. b T1-weighted image with fat saturation after intravenous administration of contrast medium. c ADC map. The calculated ADC value is 1.94 × 10−3 mm2s−1
The mean ADC value in muscle metastases was 1.28 ± 0.24 × 10−3 mm2s−1, median value, 1.20, range, 0.99–1.74 × 10−3 mm2s−1 (Table 2). Muscle lymphoma had the mean value of 0.76 ± 0.14 × 10−3 mm2s−1, range, 0.54–1.1, median value, 0.76 × 10−3 mm2s−1 (Table 3). In muscle sarcoma the mean ADC value was 1.82 ± 0.63 × 10−3 mm2s−1 (median value, 1.40, range, 0.9–2.9 × 10−3 mm2s−1; Table 4).
Muscle lymphoma showed statistically significant lower ADC values in comparison to muscle metastases (p = 0.01) and muscle sarcoma (p = 0.001; Fig. 4). There was no significant differences between ADC values in muscle metastases and sarcomas (p = 0.48). Furthermore, ADC values in muscle lymphoma were homogeneous with less inter-patient variability and were within a relatively closely range. Muscle sarcomas had a broad range of ADC values (Fig. 4). Liposarcomas showed statistically significantly higher ADC values than rhabdomyosarcoma (2.04 ± 0.56 vs 0.86 ± 0.09 × 10−3 mm2s−1, p = 0.001).

Comparison of ADC values in different muscle tumors. Muscle lymphoma shows lowest ADC values (0.76 ± 0.14 × 10−3 mm2s−1) in comparison to muscle metastases (1.28 ± 0.24 × 10−3 mm2s−1, p = 0.01) and to muscle sarcomas (1.82 ± 0.63 × 10−3 mm2s−1, p = 0.001). There is no statistically significant difference between the ADC values in muscle sarcoma and metastases (p = 0.48)
Discussion
Our study showed that malignant muscle tumors can have a wide range of ADC values on DWI depending on the histology.
As reported previously, ADC values can help to distinguish malignant and benign muscle lesions [1, 7, 9, 10, 15–17]. For example, van Rijswijk et al. showed that malignant soft-tissue tumors had lower ADC values in comparison to benign masses (1.08 vs 1.71 × 10−3 mm2s−1, p < 0.05) [7]. Razek et al. had similar results in their analysis [10]. Furthermore, the authors postulated that the selection of 1.34 × 10−3 mm2s−1 as the threshold ADC value had an accuracy of 91 %, sensitivity of 94 %, and specificity of 88 % in distinguishing between malignant and benign soft-tissue tumors [10]. In another study, a threshold ADC value of 1.7 × 10−3 mm2s−1 was proposed [1].
However, Einarsdóttir et al. found no difference between ADC values in benign soft-tissue tumors and sarcomas, which were 1.8 and 1.7 × 10−3 mm2s−1 respectively [8]. In addition, other authors also identified no significant difference in the mean ADC values among benign, intermediate, and malignant soft-tissue lesions [12]. Furthermore, according to Nagata et al., malignant and benign myxoid tumors had similar ADC values, namely 2.05 and 2.10 × 10−3 mm2s−1 respectively [12]. This fact suggests that the balance between matrix (and type of matrix) and cellularity determines diffusion, but not the dignity of lesions.
In the present analysis, the mean ADC value of all malignancies was 1.24 × 10−3 mm2s−1. However, our study showed that malignant muscle lesions, especially sarcomas, had a broad spectrum of ADC values. Some lesions were obviously above the previously reported threshold ADC values. For example, 35.1 % of our tumors were above the value of 1.34 × 10−3 mm2s−1. This discrepancy can be related to the different proportion of several malignant lesions in the studies reported. In fact, Razek et al. analyzed 23 solid sarcomas with a high proportion of rhabdomyosarcomas and several benign lesions, but not muscle metastases [10].
A unique feature of our study was the comparison of the ADC values among different malignant histologies. Interestingly, we observed that lymphomas had statistically significantly lower ADC values than sarcomas and metastases. The reason for this is uncertain, but can be related to the closely packed homogeneous architecture of lymphoma in contrast to sarcomas and metastases, which tend to have a more heterogeneous cellularity.
Our study had several limitations, including the retrospective study design. Different sarcomas were included in our analysis, but their ADC values could not be compared because of small groups. Likewise, ADC values of muscle metastases from different primary malignancies could also not be compared.
Clearly, further investigations using standardized MR protocols are needed to compare ADC values in several sarcomas and muscle metastases in a large sample.
In conclusion, our study showed that intramuscular malignant lesions had different ADC values on DWI. 22.8 % of the tumors analyzed had low ADC values, 26.3 % moderate, and 50.9 % high ADC values. Muscle lymphoma had statistically significantly lower ADC values in comparison to muscle metastases and sarcomas. Muscle sarcomas presented with a broad range of ADC values.
References
Subhawong TK, Durand DJ, Thawait GK, Jacobs MA, Fayad LM. Characterization of soft tissue masses: can quantitative diffusion weighted imaging reliably distinguish cysts from solid masses? Skeletal Radiol. 2013;42:1583–92.
Sasaki M, Eida S, Sumi M, Nakamura T. Apparent diffusion coefficient for sinonasal diseases: differentiation of benign and malignant lesions. AJNR Am J Neuroradiol. 2011;32:1256–62.
Fornasa F, Pinali L, Gasparini A, Toniolli E, Montemezzi S. Diffusion-weighted magnetic resonance imaging in focal breast lesions: analysis of 78 cases with pathological correlation. Radiol Med. 2011;116(2):264–75.
Driessen JP, Caldas-Magalhaes J, Janssen LM, et al. Diffusion-weighted MR imaging in laryngeal and hypopharyngeal carcinoma: association between apparent diffusion coefficient and histologic findings. Radiology 2014;272(2):456–63.
Schnapauff D, Zeile M, Niederhagen MB, et al. Diffusion-weighted echo-planar magnetic resonance imaging for the assessment of tumor cellularity in patients with soft-tissue sarcomas. J Magn Reson Imaging. 2009;29:1355–9.
Yamaguchi K, Schacht D, Nakazono T, Irie H, Abe H. Diffusion weighted images of metastatic as compared with nonmetastatic axillary lymph nodes in patients with newly diagnosed breast cancer. J Magn Reson Imaging. 2014; doi: 10.1002/jmri.24829.
Van Rijswijk CSP, Kunz P, Hogendoorn PC, et al. Diffusion-weighted MRI in the characterization of soft-tissue tumors. J Magn Reson Imaging. 2002;15:302–7.
Einarsdóttir H, Karlsson M, Wejde J, Bauer HC. Diffusion-weighted MRI of soft tissue tumours. Eur Radiol. 2004;14:959–63.
Genovese E, Canì A, Rizzo S, Angeretti MG, Leonardi A, Fugazzola C. Comparison between MRI with spin-echo echo-planar diffusion-weighted sequence (DWI) and histology in the diagnosis of soft-tissue tumours. Radiol Med. 2011;116(4):644–56.
Razek A, Nada N, Ghaniem M, Elkhamary S. Assessment of soft tissue tumours of the extremities with diffusion echoplanar MR imaging. Radiol Med. 2012;117(1):96–101.
Surov A, Behrmann C. Diffusion-weighted imaging of skeletal muscle lymphoma. Skeletal Radiol. 2014;43(7):899–903.
Nagata S, Nishimura H, Uchida M, et al. Diffusion-weighted imaging of soft tissue tumors: usefulness of the apparent diffusion coefficient for differential diagnosis. Radiat Med. 2008;26(5):287–95.
Oka K, Yakushiji T, Sato H, et al. Usefulness of diffusion-weighted imaging for differentiating between desmoid tumors and malignant soft tissue tumors. J Magn Reson Imaging. 2011;33(1):189–93.
Surov A, Fiedler E, Voigt W, et al. Magnetic resonance imaging of intramuscular metastases. Skeletal Radiol. 2011;40:439–46.
Khoo MM, Tyler PA, Saifuddin A, Padhani AR. Diffusion-weighted imaging (DWI) in musculoskeletal MRI: a critical review. Skeletal Radiol. 2011;40:665–81.
Subhawong TK, Jacobs MA, Fayad LM. Diffusion-weighted MR imaging for characterizing musculoskeletal lesions. Radiographics. 2014;34(5):1163–77.
Subhawong TK, Jacobs MA, Fayad LM. Insights into quantitative diffusion-weighted MRI for musculoskeletal tumor imaging. AJR Am J Roentgenol. 2014;203(3):560–72.
Conflict of interest
There are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Surov, A., Nagata, S., Razek, A.A.A. et al. Comparison of ADC values in different malignancies of the skeletal musculature: a multicentric analysis. Skeletal Radiol 44, 995–1000 (2015). https://doi.org/10.1007/s00256-015-2141-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-015-2141-5