
Abstract
Objective
To assess ligament lesions and subluxations of the carpometacarpal joints of the thumbs (CMC I) of asymptomatic volunteers and of patients with CMC I osteoarthritis using advanced magnetic resonance imaging (MRI).
Materials and Methods
A total of 20 CMC I joints of 14 asymptomatic volunteers (6× both sides) and 28 CMC I joints of 22 patients (6× both sides) with symptomatic and X-ray-diagnosed osteoarthritis of CMC I joints were studied. During extension, flexion, abduction and adduction of the thumb, the anterior oblique (AOL), intermetacarpal (IML), posterior oblique (POL) and dorsal radial (DRL) ligaments were evaluated using 3-T MRI on two standard planes, and translation of metacarpal I (MC I) was assessed.
Results
The MRI demonstrated that ligament lesions of the AOL and IML are frequent. Isolated rupture of the AOL was found in 6 of 28 (21 %), combined rupture of the AOL + IML in 5 of 28 (18 %) and isolated IML rupture in 4 of 28 (14 %) joints.
The patients had a significantly increased dorsal translation of MC I during extension with a median of 6.4 mm vs. 5.4 mm in asymptomatic volunteers (p < 0.05).
Conclusion
MRIs of CMC I in two standardized planes frequently show combined ligament ruptures. The dorsal subluxation of MC I, which is increased in patients, correlates with OA severity based on X-ray and can be quantified by MRI. For joint-preserving surgical procedures and for prosthesis implantation of the CMC I, we recommend performing an MRI in two planes of the thumb—extension and abduction—to evaluate the ligaments and dorsal subluxation of MC I.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Approximately one fifth of all women aged older than 60 years of age develop symptomatic osteoarthritis of the carpometacarpal joint I (CMC I) [1] and nearly one third exhibit signs of osteoarthritis on conventional X-rays [2–6]. Additionally, CT scan [7] and ultrasound imaging [8] can be used to visualize osteoarthritic changes of the CMC I.
According to patients’ symptoms and depending on the X-ray of the CMC I, the therapeutic options are primarily conservative. If conservative therapy fails, surgical procedures, such as trapezectomy or arthroplasty, are recommended [9–11]. Joint-preserving surgical techniques for CMC I osteoarthritis include ligament reconstruction [12] or osteotomy [13] of metacarpal I (MC I), and they are only applicable in early stages of osteoarthritis. Arthroscopic treatment of CMC I osteoarthritis has only rarely been reported [14, 15]. Knowing the status of the ligaments of CMC I allows for ligament reconstruction and/or osteotomy in metacarpal I patients with early stages of osteoarthritis.
The most frequently used classification of osteoarthritis of the CMC I is that of Eaton and Littler (1973) [16]. Nevertheless, this orthopaedic radiographic classification has had only moderate reliability of 0.66 and 0.53, respectively, in different reports [17, 18].
Beyond the moderate reliability of the radiographically based classification, subluxation of MC I cannot be measured exactly, and degenerative changes of the ligaments cannot be evaluated.
As magnetic resonance imaging, even in small joints, is improving [19, 20], it is obvious that osteoarthritis is not only a disease of the cartilage but also a whole-organ disorder, involving multiple joint tissues and resulting in eventual joint failure [21]. Connel et al. (2004) were the first to study ligamental injuries of the CMC I with magnetic resonance imaging (MRI) at 1.5 T in an in vivo study [22]. Additionally, at 1.5 T, Hirschmann et al. recently investigated the ligaments of the CMC I of asymptomatic volunteers [23].
So far, with 3-T MR, the frequency of ligamental lesions between asymptomatic volunteers and symptomatic patients with osteoarthritis of the CMC I has not been compared. The presented study aimed to standardize MRI evaluations of the thumb saddle joint using bony landmarks. The advantage of standardized images consists of comparable and measurable data from volunteers and patients. Our objective was to closely examine the differences in the frequency and location of ligament lesions of the CMC I joint by MRI. As such, we assessed the thumb in the following four positions: extension, flexion, abduction and adduction.
Materials and methods
The current study was approved by the institutional board of ethics. Prospective data sets were compared between symptomatic patients and asymptomatic volunteers.
Between 2011 and 2012, 20 carpometacarpal joints of the thumbs of 14 asymptomatic volunteers (6× both sides) were consecutively included, and 28 carpometacarpal joints of the thumbs of 22 symptomatic patients (6× both sides) with CMC I osteoarthritis were enrolled in this prospective study. The mean age of the asymptomatic volunteers (8 women, 6 men) was 43 years (range, 23-57 years), and the mean age of the patients (20 women, 2 men) was 53 years (range, 28-73 years).
Asymptomatic volunteers were defined as asymptomatic, in terms of medical history, for CMC I osteoarthritis, thumb pain or pain of the CMC I, and they had free range of motion. Volunteers were excluded with previous operations, CMC I injuries, MRI contraindications, such as pacemakers, or acute or chronic infections of the hand.
Symptomatic patients were defined as symptomatic in terms of pain or having functional deficits of the CMC I joint. We used the numeric rating scale (NRS 0-10) to measure pain. The patients had a mean joint pain of 7.6 (SD 1.7) during activity according to the NRS.
We used the questionnaire “Disabilities of the arm, shoulder and hand” (DASH) [24, 25] to evaluate patient disabilities. A value of 0 corresponded to optimal function, and a value of 100 corresponded to maximal disability. The mean DASH value of the symptomatic patients was 44.7 (SD 19.9). In symptomatic patients, X-rays of CMC I on two standard planes were obtained and classified according to Eaton and Littler [16] by an experienced radiologist (A.V.) and a senior hand surgeon (C.D.) in consensus. Eaton and Littler have classified the joint degeneration stages of CMC I noted on X-rays. Stage I equates to a normal articular contour and less than one-third subluxation in any projection. Stage II is characterized by osteophytes of less than 2 mm in diameter and at least one-third subluxation of the joint. Stage III consists of osteophytes of greater than 2 mm, greater than one-third subluxation and slight joint-space narrowing.
Stage IV is characterized by cystic and sclerotic subchondral bone changes, major subluxation and narrow joint space.
In our study showed the following distribution: Eaton Littler type I (n = 7), type II (n = 4) and type III (n = 12). None of the patients was classified as Eaton Littler type IV, with destruction of the joint surface.
MR imaging
With 3-T MRI, we used two defined standard imaging planes, as explained in the section entitled “Reformations of standard planes” (Fig. 1), to describe the ligaments involved comprehensively and to measure reference distances of MC I.

a The sesamoid bones are the bony landmark for axis A. A’ is the paracoronal standard plane. B is the parasagittal standard plane, perpendicular to plane A’. b and c The white arrow indicates the sesamoid bones. The top of both images is distal, and the bottom is proximal. In b, the left side of the image is radial, and the right side is ulnar; in c, the left side of the images is dorsal, and the right side is palmar
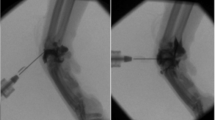
Each CMC I was examined in four different thumb positions (extension, flexion, abduction and adduction) using a custom-made, one-size-fits-all hand orthesis (Fig. 2). We used a standard ring coil in a 3-T MRI system (TIM-Trio, VB17, Siemens, Healthcare AG, Erlangen, Germany). The ring coil was placed in a dorsoradial position, centered over CMC I to avoid interference with the hand orthesis. We chose a 3D turbo spin echo sequence with variable flip angles (3D-TSE_VFL), with a voxel size of 0.5 × 0.5 × 0.4 mm (TR/TE = 1,800 ms/331 ms, field of view 220 mm, phase field of view 45 %, acquisition matrix 448 × 203, 10 % oversampling). The acquired sequences provided high resolution of the anatomy with T2 contrast. A 3D block was acquired on an oblique plane to cover the whole first metacarpal bone and the entire trapezium, in addition to the CMC I. The time for an acquisition of a single 3D data set was approximately 8-10 min. The 3D data set of all four of the thumb positions was post-processed using multiplanar reformats.

Custom-made hand orthesis: left side with a holding device for the thumb in extension, flexion, abduction and adduction
The patients and asymptomatic volunteers were positioned prone-lateral on the MRI examination table, with the arm extended overhead to place the wrist in the center of the gantry. The orthesis, used to place the thumb in the desired positions, was side-specific and was universally applicable to all of the volunteers and patients. The orthesis, which was constructed of semirigid supporting material (3 M®), was essential for the reproducibility of the imaging examinations. After the hand orthesis had been applied, a vacuum cushion was adjusted, surrounding the entire arm up to the shoulder to eliminate any involuntary movement.
All of the asymptomatic volunteers and symptomatic patients were able to tolerate the positioning during the scan period. The mean duration of the entire scan was approximately 50 min.
Reformats of standard planes
All of the 3D data sets were reformatted onto two standard imaging planes to ensure easy interindividual comparison: a paracoronal plane (subsequently called the standard plane) and a parasagittal plane. The paracoronal plane was defined by the connecting axis of the two sesamoid bones of MC I and by the longitudinal axis of MC I (Fig. 1).
The parasagittal plane runs perpendicular to the paracoronal plane.
The sesamoid bones of the human hand are visible in almost 100 % of all cases [26, 27], and they were therefore used as orientation points for the definition of the standard plane. All of the reformats were generated with a dedicated 3D software package (Siemens Syngo Via) as overlapping slices, with a section thickness of 1.2 mm and a reconstruction interval of 0.8 mm. The reformats were performed by the same radiologic technologist after being instructed, and it took approximately 20 min.
In one case of a symptomatic patient, the evaluation of the reformats in abduction of the thumb was not possible because of aliasing artifacts.
All of the images were evaluated in consensus by an experienced radiologist (A.V.) and a senior hand surgeon (C.D.), both with more than 6 years of experience in musculoskeletal imaging.
Ligaments
Although the anatomical nomenclature of the CMC I ligaments has been inconsistent [28, 29], we focused on four ligaments (Fig. 3a-c):
-
1.
The anterior oblique ligament (AOL or palmar beak ligament), which arises from the palmar tubercle of the trapezium and enters the base of MC I (Fig. 3a-b);
Fig. 3 
Palmar view of CMC I (a). Parasagittal view of CMC I with palmar tilt (b). Dorsal view of CMC I with radial translation of MC I (c)
Fig. 4 
a-b Intact and ruptured IML on the paracoronal plane. The top of the images is distal, and the bottom is proximal. The left side of the images is radial, and the right side is ulnar
Fig. 5 
a-b Intact and ruptured AOL and POL in the parasagittal section. The top of the images is distal, and the bottom is proximal. The palmar sides of the MC I`s are front to front
Fig. 6 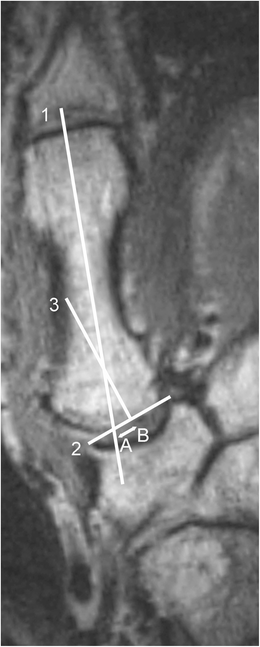
Example and schema of radial translation of MC I
Fig. 7 
Pathological dorsal translation of MC I showing the tangent to the dorsal metacarpal line of MC I
-
2.
The dorsal radial ligament (DRL), which arises from the dorsoradial tubercle of the trapezium to enter the opposite base of MC I (Fig. 3a-c);
-
3.
The posterior oblique ligament (POL), which extends from the dorsal-ulnar tubercle of the trapezium to the ulnar base of MC I (Fig. 3c); and
-
4.
The intermetacarpal ligament (IML), which extends from the radial base of metacarpal II to the ulnar base of MC I (Figs. 3a, 4).





The ligaments were evaluated with regard to morphology and abnormal signal intensity [30] in the four thumb positions on both reconstructed standard planes (Fig. 1). Four ligaments, i.e., the AOL, POL, DRL and IML, were assessed according to the criteria “intact,” “ruptured” or “non-assessable” (Figs. 4, 5, 6). Ligaments were classified as “intact” when three consecutive images showed homogeneous continuity. Ligaments were defined as “ruptured” when inhomogeneity or discontinuity was present on three consecutive images. Ligaments were classified as “indeterminate” when three consecutive images showed inconsistent results with regard to homogeneity or continuity.
Dorsal translation
In parasagittal reformats, a reference line was drawn tangential to the dorsal metacarpal surface of MC I: This is line 1 (Figs. 3b, 7 Fig. 8). The second bony landmark for dorsal translation of MC I was the dorsoradial tubercle of the trapezium, which is known to be present with a reliability of 100 % [31]. From this point of insertion of the dorsal radial ligament (DRL), a perpendicular line was drawn. The distance between the applied tangent and the dorsoradial tubercle, which was equivalent to the middle of the DRL, was measured: line 2 (Fig. 3b, Fig. 7).

Pathological palmar tilt showing the increased angle α

Box plot of MC I in extension—volunteers vs. patients
Radial translation
Radial translation of MC I, or subluxation on the trapezium, was assessed on the paracoronal standard plane (Fig. 3c). The outer edges of the concave joint area of the trapezium were connected to each other at the trapezium’s most distinctive concavity, line 2. Additionally, the longitudinal axis of the MC I diaphysis was indicated, line 1. The bisector of the angle, formed by these two lines, was drawn in an orthogonal manner, line 3, and the distance between points A and B was measured (mm), yielding the result of radial translation (Fig. 3c, Fig. 6).
MR palmar tilt of metacarpal I
MR palmar tilt was measured on MR images in a modified manner, as described on X-rays by Miura et al. [32]. First, a tangent was applied to the dorsal metacarpal line of MC I, followed by attachment of a perpendicular line to this tangent. The outer palmar and the dorsal edges of the concavity of the MC I base were then connected in a standardized manner at the radial side, amounting to the jacking point of the DRL. The angle α between the line perpendicular to the tangent and the connecting line was defined as the “MR palmar tilt” (Fig. 3b).
Osteophytes
Osteophytes were evaluated at the trapezium and at MC I in terms of localization and size (mm).
Statistics
To compare the translation positions of MC I, nonparametric test procedures were performed (Mann-Whitney U-test, p < 0.05). Statistical evaluation was performed using Microsoft Excel 2011 and Statistica, version 10 (StatSoft®).
Results
Ligaments
In the asymptomatic volunteer group, neither combined ligament lesions nor dorsal ligament lesions were observed (Table 1), although isolated ligament ruptures were observed in 4 of 20 (20 %) of asymptomatic volunteers. The AOL was ruptured in 1 of 20 (5 %) and the IML was ruptured in 3 of 20 subjects (15 %).
In symptomatic patients, isolated rupture of the AOL was found in 6 of 28 (21 %), combined rupture of the AOL + IML in 5 of 28 (18 %), isolated IML rupture in 4 of 28 (14 %), combined AOL + IML + POL + DRL in 2 of 28 (7 %), AOL + DRL + IML in 2 of 28 (7 %) and AOL + POL + DRL rupture in 1 of 28 patients (4 %).
Dorsal translation of MC I
In extension of the CMC I, dorsal translation of MC I was significantly smaller in asymptomatic volunteers than in patients (median 6.4 mm vs. 5.4 mm; p < 0.05).
The mean distance of dorsal translation of asymptomatic volunteers was 4.4 mm (3.8–4.9) vs. 6.1 mm (5.5–6.7) in patients (95 % confidence interval), with standard deviations of 1.2 and 1.6, respectively.
During flexion of CMC I, MC I came to a centered position over the trapezium and the dorsal subluxation decreased in asymptomatic volunteers. In contrast, in the patients, dorsal translation was not corrected to normal values in flexion of the CMC I, but it remained in pathological subluxation.
In asymptomatic volunteers, dorsal translation of MC I was greatest during extension (median = 5.4 mm, SD = 1.1) (Fig. 9), followed by adduction (median = 4.5 mm, SD = 1.2), abduction (median = 4.2 mm, SD = 1.1) and flexion (median = 4 mm, SD = 0.9) (Table 1). Therefore, the extension position of the thumb is recommended if dorsal translation of MC I must be evaluated.
Radial translation of MC I
Compared to dorsal translation of MC I, the distance of radial translation was significantly smaller in each of the four thumb positions (p < 0.05) in both the volunteer group and the patient group.
Radial translation of MC I was not significantly different between the asymptomatic volunteers and patients. In the asymptomatic volunteers, radial translation of MC I was greatest in adduction (median = 3.1 mm, SD = 1.1 mm); the same was true in the patient group (median = 3.1 mm, SD = 1.6 mm). Radial translation was least in abduction in both the asymptomatic volunteers (median = 1 mm, SD = 1.2 mm) and the patients (median = 1 mm, SD = 1.2 mm).
Two volunteers and three patients showed ulnar translation of MC I during abduction of the thumb (Table 1). During extension and flexion, the base of the first metacarpal bone underwent radial subluxation in both groups.
Because radial translation of MC I is pronounced in adduction of the thumb, this position is recommended if radial translation of MC I must be evaluated. Nevertheless, an additional series in abduction of the thumb is necessary to detect varieties in thumb movement.
Descriptive statistic between ligament rupture and translation of MC I
Based on our results, we sought an interrelationship between ligament rupture and dorsal and radial translation of MC I. Fifteen of the 16 cases (94 %) of AOL rupture had dorsal translation of more than 5 mm in extension.
In these cases, unlike in the cases of the asymptomatic volunteers, we observed no re-centering of MC I in flexion.
MR palmar tilt of MC I
The angle of inclination of the proximal articular surface of MC I, measured on the sagittal plane (in extension), was significantly smaller in the asymptomatic volunteers than the patients (Table 1).
The mean palmar tilt angle of MC I of asymptomatic volunteers was 8.5 degrees (7.3-9.9) vs. 15.3 degrees (13-17.6) in patients (95 % confidence interval), with standard deviations of 2.7 and 5.9, respectively.
In the asymptomatic volunteers, a palmar tilt angle of between 0° and 10° was observed in 13 of 20 (65 %), an angle of 11-20° was observed in 7 of 20 (35 %), and an angle of 20-30° was observed in 0 of 20 subjects (0 %).
In symptomatic patients, a palmar tilt angle of 0-10° was observed in 4/28 (14 %), an angle of 11-20° in 10 of 28 (36 %) and from 20-30° was observed in 14 of 28 subjects (50 %).
Osteophytes
In 18 of 28 (64 %) CMC I joints of the patients, the osteophytes of the trapezium were greater than 2 mm in width and were localized radially and ulnarly. The osteophytes of the base of MC I were located palmarly and radially.
Discussion
MRI has become increasingly important as a method for the noninvasive diagnosis of musculoskeletal disorders, especially when small joints are involved [19, 33, 34].
The present study aimed to standardize MRI evaluation of the thumb saddle joint using bony landmarks and to compare ligaments between volunteers and patients. The sesamoid bones are reliable bony landmarks in defining standard planes for MR imaging of the CMC I. Three of the four ligaments (AOL, DRL and POL) were detected on reformatted parasagittal planes, with a consistency of 100 % in asymptomatic volunteers, and one ligament (IML) was detected in paracoronal reformats, with a consistency of 90 %.
Within the four CMC I positions of the thumb we recommend assessment of AOL, POL and DRL in extension and abduction of the thumb, permitting evaluation of the ligaments in 90 % and 100 %, respectively.
Whereas assessment of IML is recommended in extension and adduction by this 90 % of the IML ligaments can be evaluated. Our results are supported by anatomical studies showing that the ligaments of the thumb obtain their maximum lengths in extension and abduction [35].
In symptomatic patients with osteoarthritis of the CMC I, isolated ruptures of ligaments of the carpometacarpal joint of the thumb are uncommon. More frequently, several ligaments are affected at the same time; the AOL and IML are most often involved in these combined lesions.
Pathologic joint instability is assumed to be one cause of trapeziometacarpal osteoarthritis [23]. Integration of the degree of radial/dorsal subluxation of MC I into an X-ray classification for osteoarthritis of the thumb was performed by Eaton and Littler [16], whose classification has been widely accepted [18].
Our results showed that the dorsal translation of MC I was significantly greater than the radial translation of MC I in all thumb positions in both the volunteers and patients. Furthermore, dorsal translation in patients with osteoarthritis did not normalize to the results obtained with asymptomatic volunteers during flexion but remained in pathological subluxation. We believe that dorsal translation of MC I of more than 6 mm indicates pathological subluxation of MC I and is a hint for advanced osteoarthritis of the CMC I.
Radial translation of MC I is, to some extent, physiological, and it can be observed in asymptomatic volunteers as well as in patients with osteoarthritis. We observed only slight differences in the degree of radial translation between the asymptomatic volunteers and patients, and we did not detect a significant increase in radial subluxation in thumbs with a ruptured IML (three asymptomatic volunteers). Hunter et al. examined the relationship between radial subluxation and the occurrence of radiological signs of CMC I osteoarthritis, and they showed that there was a correlation between these two aspects in men but not in women [36]. Our study groups were too small to verify these findings.
The third aim of this study was to evaluate differences in the MR palmar tilt of metacarpal I. Our results, obtained from parasagittal reformats, showed that MR palmar tilt was significantly greater in the patients than the asymptomatic volunteers. Therefore, an increased palmar tilt could be a predisposing factor for developing osteoarthritis of the CMC I, as assumed by other authors [32].
Concerning osteophytes in patients, these were most often located radially and ulnarly on the trapezium and on the palmar side of MC I. These results are consistent with the findings of North and Rutledge, who observed that osteophytes formed on the trapezium and the metacarpals at the edges of the concave portion of the articular surface [37].
Other authors have reported the results of research on ligaments of the CMC I in cadaveric specimens (28) using a 1.5-T MRI system and 2-mm sections to describe the ligaments. Our results, using 3-T MR imaging in two standard projections, show that parasagittal standard sections are adequate to image the AOL, DRL and POL, while paracoronal standard sections are necessary to image the IML reliably. In both cases, we recommend using thin sections (approximately 0.4 mm), as acquired in the present study, if possible.
Our study had limitations. First, the results were not adjusted according to sex or age. Second, the sensitivity and specificity of the presented MR technique can be restricted, compared with previous studies [38, 39], but it must be proved in a separate, subsequent study. We only studied patients with Eaton Littler stages I-III; stage IV was excluded because, for those patients, trapezectomy was the recommended operation. Finally, the MRI technique presented here required increased examination time and effort. The examination of four end-range positions of the CMC I joint requires approximately 50 min, even if the team is experienced.
Despite these limitations, the findings of the present study are clinically relevant. To our knowledge, the dorsal translation of MC I in patients with osteoarthritis has not been quantified. Our findings show that different isolated and combined ligament lesions of the CMC I are present. Lesions of the AOL and/or the IML are predominant, and they account for more than 50 % of ligamentous tears.
For joint-preserving surgical techniques for CMC I osteoarthritis, such as ligament reconstruction [12], it would be valuable to have information about ligament status. In particular, patients presenting with stage I or II osteoarthritis, according to Eaton and Littler [16], could benefit from ligament reconstruction when symptomatic clinical instability and MR imaging show that isolated ligament ruptures coincide. Also, patients with increased palmar tilt and planned osteotomy of MC I [13] could possibly benefit more when the ligaments of the CMC I are intact. The same holds true for prosthetic replacement. Prior to prosthetic replacement of the carpometacarpal joint of the thumb, MRI can provide information regarding possible subluxation tendencies.
We propose the following procedure for patients with symptomatic osteoarthritis of CMC I: Patients with disabilities and pain in the CMC I joint who are intended for trapezectomy do not need an MRI before surgery.
Patients with disabilities and pain in the CMC I joint who are intended for ligament reconstruction or osteotomy of MC I or prosthetic replacement should be imaged in two planes during extension and abduction of the thumb. A custom-made orthesis is an easy to produce, inexpensive and helpful accessory to prevent movement artifacts.
References
Dillon CF, Hirsch R, Rasch EK, Gu Q. Symptomatic hand osteoarthritis in the United States. Am J Phys Med Rehabil. 2007;86(1):12–21.
Haugen IK, Englund M, Aliabadi P, Niu J, Clancy M, Kvien TK, et al. Prevalence, incidence and progression of hand osteoarthritis in the general population: the Framingham Osteoarthritis Study. Ann Rheum Dis. 2011;70(9):1581–6.
Marshall M, van der Windt D, Nicholls E, Myers H, Dziedzic K. Radiographic thumb osteoarthritis: frequency, patterns and associations with pain and clinical assessment findings in a community-dwelling population. Rheumatology (Oxford). 2011;50(4):735–9.
Wilder FV, Barrett JP, Farina EJ. Joint-specific prevalence of osteoarthritis of the hand. Osteoarthr Cartil/OARS Osteoarthr Res Soc. 2006;14(9):953–7.
Zhang Y, Niu J, Kelly-Hayes M, Chaisson CE, Aliabadi P, Felson DT. Prevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: The Framingham Study. Am J Epidemiol. 2002;156(11):1021–7.
Armstrong AL, Hunter JB, Davis TR. The prevalence of degenerative arthritis of the base of the thumb in post-menopausal women. J Hand Surg (Br). 1994;19(3):340–1.
Saltzherr M, Neck J, Muradin GR, Ouwendijk R, Luime J, Coert JH, et al. Computed tomography for the detection of thumb base osteoarthritis: comparison with digital radiography. Skeletal Radiol. 2013;42(5):715–21.
Gondim Teixeira PA, Omoumi P, Trudell DJ, Ward SR, Blum A, Resnick DL. High-resolution ultrasound evaluation of the trapeziometacarpal joint with emphasis on the anterior oblique ligament (beak ligament). Skeletal Radiol. 2011;40(7):897–904.
Davis T, Brady O, Barton N, Lunn P, Burke F. Trapeziectomy alone, with tendon interposition or with ligament reconstruction? A randomized prospective study. J Hand Surg Br. Soc Surg Hand. 1997;22(6):689–94.
Vermeulen GM, Slijper H, Feitz R, Hovius SE, Moojen TM, Selles RW. Surgical management of primary thumb carpometacarpal osteoarthritis: a systematic review. J Hand Surg. 2011;36(1):157–69.
Aliu O, Davis MM, DeMonner S, Chung KC. The influence of evidence in the surgical treatment of thumb basilar joint arthritis. Plast Reconstr Surg. 2013;131(4):816–28.
Freedman DM, Eaton RG, Glickel SZ. Long-term results of volar ligament reconstruction for symptomatic basal joint laxity. J Hand Surg. 2000;25(2):297–304.
Tomaino MM. Treatment of Eaton stage I trapeziometacarpal disease with thumb metacarpal extension osteotomy. J Hand Surg. 2000;25(6):1100–6.
Zhang AY, Van Nortwick S, Hagert E, Ladd AL. Thumb carpometacarpal ligaments inside and out: a comparative study of arthroscopic and gross anatomy from the Robert A. Chase Hand and Upper Limb Center at Stanford University. J Wrist Surg. 2013;2(1):55–62.
Cobb TK, Berner SH, Badia A. New frontiers in hand arthroscopy. Hand Clin. 2011;27(3):383–94.
Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am. 1973;55(8):1655–66.
Kubik 3rd NJ, Lubahn JD. Intrarater and interrater reliability of the Eaton classification of basal joint arthritis. J Hand Surg. 2002;27(5):882–5.
Spaans AJ, van Laarhoven CM, Schuurman AH, van Minnen LP. Interobserver agreement of the Eaton-Littler classification system and treatment strategy of thumb carpometacarpal joint osteoarthritis. J Hand Surg. 2011;36(9):1467–70.
Braum LS, McGonagle D, Bruns A, Philipp S, Hermann S, Aupperle K, et al. Characterisation of hand small joints arthropathy using high-resolution MRI–limited discrimination between osteoarthritis and psoriatic arthritis. Eur Radiol. 2013;23(6):1686–93.
Tehranzadeh J, Ashikyan O, Anavim A, Tramma S. Enhanced MR imaging of tenosynovitis of hand and wrist in inflammatory arthritis. Skeletal Radiol. 2006;35(11):814–22.
Roemer FW, Crema MD, Trattnig S, Guermazi A. Advances in imaging of osteoarthritis and cartilage. Radiology. 2011;260(2):332–54.
Connell DA, Pike J, Koulouris G, van Wettering N, Hoy G. MR imaging of thumb carpometacarpal joint ligament injuries. J Hand Surg. 2004;29(1):46–54.
Hirschmann A, Sutter R, Schweizer A, Pfirrmann CW. The carpometacarpal joint of the thumb: MR appearance in asymptomatic volunteers. Skeletal Radiol. 2013;42(8):1105–12.
Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996;29(6):602–8.
Marks M, Schoones JW, Kolling C, Herren DB, Goldhahn J, Vliet Vlieland TP. Outcome measures and their measurement properties for trapeziometacarpal osteoarthritis: a systematic literature review. J Hand Surg Eur Vol. 2013;38(8):822–38.
Amar E, Rozenblat Y, Chechik O. Sesamoid and accessory bones of the hand—an epidemiologic survey in a Mediterranean population. Clin Anat. 2011;24(2):183–7.
Joseph J. The sesamoid bones of the hand and the time of fusion of the epiphyses of the thumb. J Anat. 1951;85(3):230–41.
Edmunds JO. Current concepts of the anatomy of the thumb trapeziometacarpal joint. J Hand Surg. 2011;36(1):170–82.
Bettinger PC, Linscheid RL, Berger RA, Cooney WP, An KN. An anatomic study of the stabilizing ligaments of the trapezium and trapeziometacarpal joint. J Hand Surg [Am]. 1999;24(4):786–98.
Connell D. MR imaging of thumb carpometacarpal joint ligament injuries. J Hand Surg: J British Soc Surg Hand. 2004;29(1):46–54.
Humes D. The Osteology of the Trapezium. J Hand Surg: J British Soc Surg Hand. 2004;29(1):42–5.
Miura T, Ohe T, Masuko T. Comparative in vivo kinematic analysis of normal and osteoarthritic trapeziometacarpal joints. J Hand Surg. 2004;29(2):252–7.
Chhabra A, Soldatos T, Thawait GK, Grande FD, Thakkar RS, Means Jr KR, et al. Current perspectives on the advantages of 3-T MR imaging of the wrist. Radiographics. 2012;32(3):879–96.
Hodgson RJ, O'Connor PJ, Grainger AJ. Tendon and ligament imaging. Br J Radiol. 2012;85(1016):1157–72.
Imaeda T, Niebur G, Cooney WP, Linscheid R, An K. Ligament length during circumduction of the trapeziometacarpal joint. J Orthop Sci. 1997;2:319–27.
Hunter DJ, Zhang Y, Sokolove J, Niu J, Aliabadi P, Felson DT. Trapeziometacarpal subluxation predisposes to incident trapeziometacarpal osteoarthritis (OA): the Framingham Study. Osteoarthr Cartil / OARS, Osteoarthr Res Soc. 2005;13(11):953–7.
North ER, Rutledge WM. The trapezium-thumb metacarpal joint: the relationship of joint shape and degenerative joint disease. Hand. 1983;15(2):201–6.
Cardoso FN, Kim HJ, Albertotti F, Botte MJ, Resnick D, Chung CB. Imaging the ligaments of the trapeziometacarpal joint: MRI compared with MR arthrography in cadaveric specimens. AJR Am J Roentgenol. 2009;192(1):W13–9.
Collins ED. Magnetic resonance imaging technology in evaluating the presence and integrity of the anterior oblique ligament of the thumb. Orthop Rev. 2012;4(2):e23.
Acknowledgments
The authors would like to thank Mrs. Ilona Pfahlert for her excellent support during the MRI investigation and Mr. Thomas Janczek for his competent support in planning and designing the orthesis used in the MR examinations.
Disclosures of Potential Conflicts of Interest
There are no potential conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dumont, C., Lerzer, S., Vafa, M.A. et al. Osteoarthritis of the carpometacarpal joint of the thumb: a new MR imaging technique for the standardized detection of relevant ligamental lesions. Skeletal Radiol 43, 1411–1420 (2014). https://doi.org/10.1007/s00256-014-1955-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-014-1955-x