
Abstract
Objective
To describe and analyze the ultrasonographic appearance of subcutaneous angiolipoma in pathology-proven cases.
Materials and methods
We retrospectively searched the January 2004 to May 2011 surgical pathology database for cases of pathology-proven angiolipoma. The ultrasonographic findings were analyzed for angiolipoma size, shape, margin, echo texture, echogenicity, acoustic enhancement, calcifications, and color Doppler flow.
Results
Of 31 angiolipomas, 19 lesions occurred in an upper extremity, one in a lower extremity, nine in the chest and abdominal wall, and two in the back. The mean tumor size was 17.7 mm. Twenty-five cases (80%) appeared as oval mass and all tumors had well-defined margins. All cases showed hyperechoic; 14 (45%), homogeneous; 17 (55%), heterogeneous. Seven cases (23%) showed blood flow in the mass. Acoustic enhancement and calcification was not shown in any cases. A correct preoperative diagnosis was made in three cases (10%) by ultrasonography.
Conclusions
Most subcutaneous angiolipomas are oval-shaped, have well-defined margins, and hyperechoic appearance on ultrasonography. Although color Doppler flow of subcutaneous angiolipoma is not seen in many cases, it may helpful in differentiating angiolipoma from ordinary subcutaneous lipoma.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Angiolipoma was originally described by Howard and Helwig in 1960 [1]; it is a common vascular lipoma variant which accounts for 5–17% of all lipomas [2], which are classified as a noninfiltrating form and a rare, deeper infiltrating form involving skeletal muscle and deep soft tissues [3]. The noninfiltrating type occurs on the trunk and extremities of young adults, with the forearm being the most common location [2, 3]. Lesions previously described as being deep infiltrating angiolipomas have now been recognized by the World Health Organization (WHO) as intramuscular hemangiomas [4, 5]. Angiolipomas manifest as small (< 2 cm), slowly growing, subcutaneous mass that are painful on palpation. The pain often diminishes over time and is not intensified by thermal changes. Trauma has been suggested as a possible contributing cause of the lesion [6].
There are several clinical reports of subcutaneous angiolipoma in the English pathology and dermatology literature [7, 8]. Because of their subcutaneous location and indolent clinical appearance in young patients, angiolipomas are only rarely imaged. The ultrasonographic appearance of subcutaneous angiolipoma has been described in a case report [9], however, ultrasonographic findings including the internal vascularity in a large number of subcutaneous angiolipomas, have not been reported in the literature.
In the present study, we analyze and describe the ultrasonographic findings of subcutaneous angiolipoma.
Materials and methods
We retrospectively searched our hospital’s surgical pathology database from January 1, 2004 and May 31, 2011 for cases of pathologically proven angiolipoma. Sixty-eight cases were identified. We excluded 35 angiolipomas without preoperative imaging studies as well as two patients who had undergone MRI. Therefore, 31 angiolipomas with preoperative ultrasonography were included in this study. Two patients had four angiolipomas, three patients had three angiolipomas, and one patient had two angiolipomas in different anatomic sites. The study population consisted of five female patients and 13 male patients (mean age, 40.8 years; range, 22–58 years). The study was conducted according to the principles of the Declaration of Helsinki, and all patients gave informed consent for the use of their information.
Ultrasonography was performed by an experienced musculoskeletal radiologist (B.S.K.) using either an HDI 5000 (Philips Medical Systems, Bothell, WA) or an iU-22 scanner (Philips Medical Systems, Bothell, WA) equipped with a 5- to 12-MHz or 7- to 15-MHz linear array transducer. Gray-scale and color Doppler flow ultrasonographic images were obtained. Scanning was done in both the transverse and longitudinal planes. The images were reviewed in consensus by two musculoskeletal radiologists (B.S.K. and S.Y.L.) with 8 years and 3 years, respectively, of musculoskeletal ultrasonography.
The gray-scale images were evaluated for the following characteristics: size (maximum diameter); shape (round, oval, or lobular); margin (well-defined or ill-defined); echogenicity relative to the adjacent muscle (hyperechoic, isoechoic, or hypoechoic); echotexture (homogeneous or heterogeneous); acoustic enhancement; and internal calcification. The presence of vascularity was determined and its pattern (peripheral, central, or peripheral and central) was identified on color Doppler ultrasonographic images.
Results
Of the 31 angiolipomas included in this study, 19 (61%) were located in the upper extremity [forearm (n = 11), upper arm (n = 4), elbow (n = 4)], one (3%) was in the lower extremity, nine (29%) were in the chest and abdominal wall, and two (7%) were in the back. All 31 lesions appeared as painless, palpable masses according to our medical records. Thirty tumors (97%) were slow-growing over several months or years.
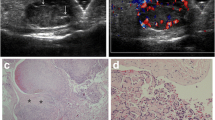
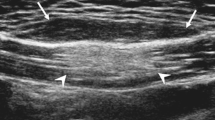
The ultrasonographic features of subcutaneous angiolipoma are shown in Table 1. On examination, the largest tumor diameters varied from 7 to 44 mm (mean, 17.7 mm) and 20 (65%) were between 11 and 20 mm. With regard to lesion shape, 25 (80%) were oval, three (10%) were round, and three (10%) were lobular. All tumors had well-defined margins and showed hyperechoic appearance versus muscle echogenicity. Internal echogenicity had as homogeneous appearance in 14 cases (45%) (Fig. 1) and heterogeneous appearance in 17 cases (55%) (Fig. 2a). No tumor showed acoustic enhancement or internal echogenic foci representing calcification. Doppler flow signals were observed in seven cases (23%) but not in the other 24 cases (77%); they were also visible in the peripheral region in all cases (Fig. 2b).

A 27-year-old male with a subcutaneous angiolipoma on the left forearm. Ultrasonography shows a well-circumscribed, homogeneous, hyperechoic mass (white arrows)

A 29-year-old male with a subcutaneous angiolipoma on the left abdominal wall. a. Ultrasonography of the palpable mass shows its well-circumscribed, hyperechoic appearance with occasional, internal hypoechoic areas (white arrows). b. Color Doppler image shows the inner peripheral vascularity of the mass
A correct preoperative diagnosis was made in three cases (10%) by ultrasonography. The common ultrasonographic misdiagnoses were lipoma and hemangioma.
Discussion
Angiolipoma is a common vascular lipoma variant. Subcutaneous angiolipoma is a distinct lesion differing from the most common ordinary lipoma in several respects. It is usually smaller than a lipoma and appears at an earlier patient age, usually as multiple subcutaneous small nodules in young adults [1, 10]. Angiolipoma generally occurs sporadically, although a familial tendency has been noted in approximately 10% of patients [1].
Histologically, angiolipoma has a normal karyotype in contrast to ordinary lipoma with karyotypic abnormalities. The fact that subcutaneous angiolipoma has a virtually consistent normal karyotype would be more in keeping with their non-neoplastic nature, and this supports the clinicopathologic impression of this lesion as being reactive or hamartomatous [11]. Microscopic examination of angiolipoma revealed mature adipose tissue separated by a branching network of small blood vessels. Vessels often appear as lobulated collections at the tumor periphery and may be plugged with hyaline thrombi, both of which are highly suggestive of the diagnosis [3, 12].
At our institution, 51% of all subcutaneous angiolipomas were excised without preoperative imaging studies. This is mainly due to the superficial location of subcutaneous angiolipomas. Also, the ultrasonographic features of this tumor are not well known due to excision without preoperative imaging studies. Choong et al. [9] reported the ultrasonographic appearance of subcutaneous angiolipoma as being well-defined, predominantly hyperechoic masses containing small, patchy, hypoechoic areas and with a sparse internal vasculature. Similarly, the subcutaneous angiolipoma appeared as a well-defined and hyperechoic mass compared to the muscle in a published study [13]. According to case reports regarding the ultrasonographic findings of angiolipoma in the breast, common findings also included a well-circumscribed, hyperechoic mass without posterior acoustic enhancement or shadowing [14, 15]. Most of the subcutaneous angiolipoma seen in our study showed well-defined margins, hyperechoic appearance, and no acoustic enhancement or calcification; these findings are similar to those of previous case reports.
Because subcutaneous angiolipoma is a lipoma variant, the ultrasonographic findings are expected to resemble those of lipoma; Fornage et al. [16] described its ovoid shape (100%), well-defined margin (60%), hyperechoic (29%) or hypoechoic (29%) appearance, whereas Ahuja et al. [17] described the ovoid shape (100%), well-defined margin (88%), and hyperechoic (76%) appearance on ultrasonography. In our study, subcutaneous angiolipomas had an ovoid shape in some cases, and well-defined margins and hyperechoic appearance in more cases when compared to a previous report regarding ordinary subcutaneous lipoma. Lipomas commonly have an internal structure very similar to the surrounding fat with internal striations, and may, therefore, sometimes be almost invisible on ultrasonography. The hyperechoic appearance of all of the angiolipomas in our study is one of the different findings from lipomas. In addition, acoustic enhancement or calcification was not seen in all cases in our study, and these findings are also the same as those seen in previous reports regarding ordinary subcutaneous lipoma.
Vascular signal on color Doppler images is sometimes seen in a larger, ordinary subcutaneous lipoma and is prominent in a hemangioma. As the size of an ordinary subcutaneous lipoma or hemangioma increases, proliferation of the internal vessel or of adjacent adipose tissue is thought to have occurred. Therefore, color Doppler findings of ordinary lipoma or hemangioma may be similar to those of subcutaneous angiolipoma.
The presence of blood flow within subcutaneous angiolipoma has also not been assessed previously. In our study, color Doppler flows were found in only seven cases (23%) and in a peripheral region in all cases. This finding is explained by the differences in the components of lipomatous and angiomatous elements. The ratio of mature lipocytes and angiomatous proliferation elements varies, and the degree of vascular proliferation ranges from less than 5% to more than 90% of the lesion [14]. Use of the technique of Doppler ultrasonography is also important. If the soft tissue is compressed, the vascular structures can become compromised, thus leading to an underestimation of blood flow. Ideally, minimal transducer pressure should be exerted while still maintaining good contact. The most effective way to achieve this is to use copious jelly [18]. Understanding and optimization of the Doppler parameters is necessary in order to detect low velocity flow. Compared to color Doppler, power Doppler is much more sensitive to slow flow and thus usually proves to be more valuable. In our study, only the color Doppler technique was used in all cases. If we had used power Doppler, the detection rate of blood flow in subcutaneous angiolipomas may have increased.
Most angiolipomas have an excellent prognosis after complete surgical excision [19]. There is no tendency toward either malignant transformation or local recurrence. In our study, no local recurrence or distant metastasis of subcutaneous angiolipoma was found in any cases.
The ultrasonographic differential diagnosis of subcutaneous angiolipoma includes ordinary lipoma, hibernoma, hemangioma, pilomatricoma, and liposarcoma. Ordinary lipoma cannot be distinguished from subcutaneous angiolipoma on gray-scale images. On color Doppler ultrasonographic images, an ordinary lipoma usually shows no vascular signal; however, in some large, subcutaneous lipomas with internal vascularity, the differential diagnosis is very difficult. Hibernoma may have a hypervascular appearance rather than that of subcutaneous angiolipoma. Hemangioma has occasionally calcifications (phleboliths) and usually low-frequency Doppler flows are evident within anechoic vascular channels; if a hemangioma does not have calcifications or anechoic vascular channels, it is difficult to distinguish between angiolipoma and hemangioma. Pilomatricoma has inner echogenic calcification, a peripheral hypoechoic rim, and peripheral Doppler flow. Liposarcoma, in particular the well-differentiated subtype, also appears as a well-defined, heterogeneous, multi-lobulated mass with internal vascularity; however, it rarely occurs in the subcutaneous fat layer, it appears as a larger mass, and occasionally has calcifications.
This study has several limitations. Because of its retrospective nature, we found it difficult to characterize the ultrasonographic features in a few of the earlier cases. Variability in the interpretation of the surgical specimens by the pathologists is also one of the limitations.
In conclusion, most subcutaneous angiolipomas are oval-shaped with well-defined margins and hyperechoic appearance on ultrasonography. Although color Doppler flow of subcutaneous angiolipoma is not seen in many cases, it may be helpful for differentiating angiolipoma from ordinary subcutaneous lipoma.
References
Howard WR, Helwig EB. Angiolipoma. Arch Dermatol. 1960;82:924–31.
Kyriakos M. Tumors and tumorlike conditions of the soft tissue. In: Kissane JM, editor. Anderson’s pathology. 9th ed. St Louis, Mo: Mosby; 1990. p. 1838–928.
Lin JJ, Lin F. Two entities in angiolipoma: a study of 459 cases of lipoma with review of literature on infiltrating angiolipoma. Cancer. 1974;34:720–7.
Christopher D, Unni K, Mertens F. Adipocytic tumors. WHO Classification of tumors. Pathology and genetics: tumors of soft tissue and bone. Lyon, France: IARC, 2002;19–46.
Murphey MD, Fairbairn KJ, Parman LM, Baxter KG, Parsa MB, Smith WS. Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. Radiographics. 1995;15:893–917.
Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. From the archives of the AFIP: benign musculoskeletal lipomatous lesions. Radiographics. 2004;24:1433–66.
Punia RS, Jain P. Amanjit, Mohan H, Singh R. Subcutaneous angiolipomas: a clinicopathological study of 12 cases. Indian J Pathol Microbiol. 2005;48:197–8.
Lapidoth M. Ben Amitai D, Feinmesser M, Akerman L. Capillary malformation associated with angiolipoma: analysis of 127 consecutive clinic patients. Am J Clin Dermatol. 2008;9:389–92.
Choong KK. Sonographic appearance of subcutaneous angiolipomas. J Ultrasound Med. 2004;23:715–7.
Allen PW. Tumors and proliferations of adipose tissue: clinicopathologic approach. New York: Masson Publishing; 1981. p. 14–7.
Sciot R, Akerman M, Cin PD, et al. Cytogenetic analysis of subcutaneous angiolipoma: further evidence supporting its difference from ordinary pure lipomas. Am J Surg Pathol. 1997;21:441–4.
Tavassoli FA. Mesenchymal lesions. In: Tavassoli FA, editor. Pathology of the Breast. Norwalk, CT: Appleton & Lange; 1992. p. 517–60.
Inampudi P, Jacobson JA, Fessell DP, et al. Soft-tissue lipomas: accuracy of sonography in diagnosis with pathologic correlation. Radiology. 2004;233:763–7.
Rosenfield Darling ML, Babagbemi TO, Smith DN, Brown FM, Lester SC, Meyer JE. Mammographic and sonographic features of angiolipoma of the breast. Breast J. 2000;6:166–70.
Weinstein SP, Conant EF, Acs G. Case 59: Angiolipoma of the breast. Radiology. 2003;227:773–5.
Fornage BD, Tassin GB. Sonographic appearances of superficial soft tissue lipomas. J Clin Ultrasound. 1991;19:215–20.
Ahuja AT, King AD, Kew J, King W, Metreweli C. Head and neck lipomas: sonographic appearance. Am J Neuroradiol. 1998;19:505–8.
Teh J. Applications of Doppler imaging in the musculoskeletal system. Curr Probl Diagn Radiol. 2006;35:22–34.
Weiss S, Goldblum J. Benign lipomatous tumors: Enzinger and Weiss’s soft tissue tumors. 4th ed. St Louis, Mo: Mosby; 2001. p. 571–639.
Acknowledgments
We thank Bonnie Hami, Department of Radiology, University Hospitals of Cleveland, for her editorial assistance in the preparation of this manuscript.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bang, M., Kang, B.S., Hwang, J.C. et al. Ultrasonographic analysis of subcutaneous angiolipoma. Skeletal Radiol 41, 1055–1059 (2012). https://doi.org/10.1007/s00256-011-1309-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-011-1309-x