
Abstract
Hip resurfacing arthroplasty is an increasingly common procedure for osteoarthritis. Conventional radiographs are used routinely for follow-up assessment, however they only provide limited information on the radiological outcome. Various complications have been reported in the scientific literature although not all are fully understood. In an effort to investigate problematic or failing hip resurfacings, various radiological methods have been utilized. These methods can be used to help make a diagnosis and guide management. This paper aims to review and illustrate the radiographic findings in the form of radiography, computerized tomography (CT), magnetic resonance imaging (MRI), and ultrasound of both normal and abnormal findings in hip resurfacing arthroplasty. However, imaging around a metal prosthesis with CT and MRI is particularly challenging and therefore the potential techniques used to overcome this are discussed.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In recent years, metal-on-metal (MoM) hip resurfacing arthroplasty (HRA) has become an increasingly common option particularly in the younger, more-active patient because of the relatively poor results in young patients with conventional total hip arthroplasty (THA) when compared to elderly less-active patients [1, 2]. Hip resurfacing now accounts for up to one in ten primary hip arthroplasties [3]. As HRA becomes more common, it is encumbent on the radiologist to recognize the different prostheses, to understand how to facilitate imaging around bulky metal implants, and to recognize the normal appearances and complications of these prostheses as the modes of failure may be different to conventional total hip arthroplasty.
The various advantages of hip resurfacing include the preservation of metaphyseal and diaphyseal bone, which is particularly important in the younger patient who may well in time require a revision procedure, the reduced rate of dislocation, improved wear properties of the bearing surfaces, and improved biomechanics of the hip joint [4]. A number of clinical series have reported good short to medium-term clinical outcomes including survival [5–9]. Despite these advantages, a number of complications specific to MoM HRA have been encountered. The aim of this paper is to review the normal radiological findings and complications associated with hip resurfacings in the form of conventional plain radiographs, magnetic resonance imaging (MRI), and computerized tomography (CT). The challenges to imaging metal implants and methods of improving image quality are discussed.
Indications and advantages of hip resurfacing
Hip resurfacing is particularly indicated in the young active patient with good bone stock. There is preservation of the metaphyseal and diaphyseal femoral bone and this is particularly important in the younger population as they may need revision surgery in the future. There is also restoration of the radiological biomechanics of the hip [4]. The larger femoral head sizes as compared to total hip arthroplasty reduce the risk of dislocation [10]. Furthermore, longevity should be improved by the improved wear characteristics of the metal-on-metal bearing surfaces.
Resurfacing is primarily used for patients with osteoarthritis of the hip. However, if the bone quality is satisfactory, then patients with ankylosing spondylitis, rheumatoid arthritis, and other inflammatory arthropathies affecting the hip can undergo resurfacing. Patients with developmental dysplasia of the hip can also be treated with HRA. One particular benefit compared to conventional hip arthroplasty is the ability to resurface patients with proximal femoral deformities, as there is no need to place a stem in the proximal femur.
Brands/types of hip resurfacing
Virtually all the major orthopedic implant companies now produce their own version of hip resurfacing implants (Table 1). They are all very similar, with some minor differences.
The most common implant in use in England and Wales is the Birmingham Hip Resurfacing (BHR) (Smith and Nephew Inc., Memphis, TN), accounting for 45% of all hip resurfacings [3] in England and Wales (Table 1). The BHR consists of an uncemented acetabular component that achieves primary fixation through press-fit and circumferential fins. This is similar to other hip resurfacing implants such as the Durom Resurfacing (Zimmer, Warsaw, IN), which sports acetabular components with and without circumferential fins. The acetabular components of the different brands of hip resurfacings are coated using various methods and materials; however, they all serve to provide a bone ingrowth surface at the implant bone interface and to achieve maximum secondary stability.
There are some variations in the thickness of the acetabular component. The ReCap (Biomet, Warsaw, IN) resurfacing has an acetabular thickness of 3 mm allowing for greater preservation of acetabular bone stock whereas the BHR is 3–4 mm thick. The acetabular components are also varied in that some are a full hemisphere while others are sub-hemispherical as there is always a balance between increasing range of motion (sub-hemispherical) and achieving maximal coverage of the femoral head and improving stability (hemispherical). For example, the 165° acetabular component of the Durom Resurfacing is less than a hemisphere and therefore allows for a greater range of motion, and is also similar in shape to the natural acetabulum. Consequently, less reaming is required, conserving bone stock. The ASRFootnote 1 (Articular Surface Replacement, DePuy, Johnson and Johnson, Leeds, UK) hip resurfacing is also sub-hemispherical, whereas the BHR almost a full hemisphere, and the ReCap hip resurfacing also has a fully hemispherical acetabular component.
The femoral component of a resurfacing may be cemented or uncemented depending on the manufacturer. The BHR and Durom hip resurfacings have a cemented femoral component (hybrid fixation) as do most other hip resurfacings. In contrast, the Cormet hip resurfacing (Corin, Gloucestershire, UK) has options for both cemented and cementless femoral components. If the femoral component is cemented, this is not visible on radiography as the cement mantle lies under the femoral head. The implant components are made from high carbon cobalt-chromium alloys, although there are some slight variations in the manufacturing technique.
Dysplasia cup
If there is a deficiency in the superolateral aspect of the acetabulum, the dysplasia cup is also available. This is designed with two superolateral screw holes to allow for additional fixation (Fig. 1).

Pre (a) and post-op (b) radiographs of the BHR Dysplasia Cup used for acetabular dysplasia. Note the superolateral screws for additional fixation
Birmingham mid head resection arthroplasty
A standard resurfacing is not always possible because of certain contraindications such as large cysts of the femoral head or avascular necrosis. In these cases, an alternative must be considered including a conventional total hip arthroplasty. Alternatively, the Birmingham Mid Head Resection arthroplasty (BMHR) can be utilized and has both uncemented acetabular and femoral components. The BMHR consists of a short proximal load-bearing stem with a larger portion resected from the femoral head (Fig. 2). The BMHR also offers the advantage of being bone-conserving relative to THA, although less so than the standard BHR.

Pre-op radiograph of right hip with large cysts of the femoral head (a) (note a standard BHR has already been performed on the left hip). (b) Intra-operative picture showing large cyst which would not be suitable for standard resurfacing. (c) Post-op radiograph showing the Birmingham Mid-Head Resection of the right hip which can be compared with the left hip BHR
Imaging around metal: challenges to CT and MR
Computed tomography
Plain radiographic assessment of hip resurfacing is routinely used for follow-up of hip resurfacing. However, as with conventional total hip arthroplasty, there remains a definite role for computed tomography (CT) in the evaluation of HRA, as it is complimentary to standard radiography and provides a three-dimensional image, allowing for easier identification of complications.
A particular problem with CT is the artefact caused by the large metal head and socket, which results in beam hardening, attenuation of the x-ray beam, and degradation of the image produced. This is particularly so with HRA, as these are invariably manufactured from cobalt-chromium (CoCr), which has a very high x-ray beam attenuation coefficient compared to other materials such as titanium and stainless steel. To overcome this, various adjustments to the scanning protocol can be made.
An increase in the tube charge (mAs) with multichannel CT with lower pitch settings can be used to improve image quality. Lower pitch settings also reduce splay artefacts, which can be further reduced if the number of detector rows is increased. Furthermore, lower pitch settings also increase the likelihood of collecting adequate projection data by collecting redundant data. Using a narrow collimation can help reduce artefact even further. The peak kilovoltage can also be increased to improve penetration of the metal by the x-ray beam, thereby further reducing artefact. Image reconstruction algorithms can also be improved to further reduce artefact. The reconstruction filter used is important, particularly with the dense CoCr components where a standard or a smooth filter will reduce artefact, although it will also result in a reduction in spatial resolution [11]. On the other hand, if a bone algorithm is used, the artefact is accentuated. Multiplanar reconstruction can result in reformatted images that are thicker (having acquired thinner sections to avoid partial volume artefacts) and have reduced metal-artefacts and better signal-to-noise ratio. Reconstruction can also be performed to produce surface 3D or volumetric rendered images, which can be used to better define the position of the HRA components relative to the pelvis (Fig. 3). In addition, volumetric rendering may also provide semitransparent views of bones that can help reduce artefact. The use of wide windows (up to 40,000 Hounsfield units) reduces metal artefact and this is facilitated by using extended scale CT and dedicated workstations. However, extended-scale CT scanners are not commonly available. The position of the components relative to the x-ray beam plays an important role in the amount of artefact as the degree of attenuation is proportional to the thickness of the attenuating components. Artefact is reduced if the x-ray beam passes through the component at its smallest cross-sectional area. However, in practice, it is generally not possible to alter significantly the position of the patient.

3D reconstruction showing the HRA of the right hip. The triangle represents the anterior pelvic plane (APP), which is a plane made up of both the anterior superior iliac spines and the pubic tubercle. The anteversion of the acetabular component for example is calculated by fitting a plane to the face of the socket and measuring the angle of this relative to the APP
Magnetic resonance imaging
MRI has traditionally played a limited role in the assessment of hip replacements due to the susceptibility artefact caused by the large metal components, and this is exacerbated at high-field strengths. Despite this, various imaging techniques can be utilized to reduce artefact and improve the quality of the MR images.
Artefact may be reduced by using wide bandwidth sequences and lower magnetic field strengths. Artefact reduction may also be achieved by using short tau inversion recovery (STIR) rather than spectral fat-saturation sequencing (which is often used on musculoskeletal imaging to reduce the signal from fat). However, each of these techniques reduce the signal-to-noise ratio of the images. Further reduction in artefact can be achieved by reducing the voxel size, which is determined by the field of view (small field of view reduces artefact), image matrix (high-resolution matrix reduces artefact), and section thickness (thinner sections reduce artefact) selected at image acquisition. Furthermore, increasing the frequency-encoding gradient strength and using spin-echo (SE) and fast spin-echo (FSE) sequences rather than gradient echo reduces artefact. FSE helps reduce diffusion-related signal loss, which is represented by dark areas around the components by refocusing spins at a faster interval than with SE imaging. This can be further enhanced with short echo spacing (short time intervals between echoes); FSE also reduces artefact arising from malrotation. However, misregistration artefacts are a major problem with SE and FSE sequences. This can be overcome to some extent by selective orientation of the frequency and phase encoding directions of the acquisition to move the misregistration artefact away from the area of clinical interest [12].
View angle tilting (VAT) is an additional tool used to reduce metallic artefact [13]. It involves adding a compensatory gradient during image acquisition to correct inhomogeneity-induced artefacts. VAT results in a lower image signal-to-noise ratio, and also causes blurring of the image, which can be partially improved by increasing the phase and frequency-encoding gradients. Slice Encoding for Metal Artefact Correction (SEMAC), can be used to further correct metal artefacts by extending a VAT spin-echo sequence with additional z-phase encoding [14]. Butts et al. [15] have described various methods for reducing blurring associated with VAT by the use of quadratic phase radiofrequency (RF) pulse, or multiple high-bandwidth readout techniques including echo-planar and flyback trajectories.
Another method used is single-point imaging (SPI). The images produced are immune to the susceptibility artefacts observed with conventional MRI as this method acquires only one point of the free induction decay immediately after excitation. The disadvantages of SPI are that it requires large gradient amplitudes and long scanning times [16].
Many of these metal artefact reduction sequences (MARS) can be combined and are now commonly used to assess both conventional hip arthroplasty and MoM HRA.
HRA are composed primarily of cobalt, which is ferromagnetic and chromium, which is not. The greater the ferromagnetism the greater the artefact created [17]. In addition, the severity of the artefact is also increased with increasing component size. Although these factors cannot be changed, it is important to consider these when imaging HRAs. Artefact can also be reduced by aligning the primary magnetic field with the longitudinal axis of the components [17]; however, as with CT this is not really an option, as the patient position cannot be significantly adjusted within the confines of the magnet bore
Ultrasound
With the continued improvements and accessibility to CT and MRI, the role of ultrasound is fairly limited in the assessment of the resurfaced hip. However, it can provide a simple, cost-effective method of evaluating an HRA when other methods are not available. It may be particularly useful in demonstrating and evaluating collections of fluid around the hip or within the periarticular bursae and can show periarticular soft tissue masses or evidence of iliopsoas tendinopathy (see below). Furthermore, ultrasound has been used to guide aspiration of collections in and around the hip joint and similarly it can be used to guide therapeutic injections for example in iliopsoas tendinopathy.
Assessment of the post-operative prosthesis: Radiographic criteria
At follow-up, clinical outcome can be measured not only by assessing patient satisfaction but also by using various outcome measures, which can help quantify the outcome. These may include the Harris Hip Score (HHS) [18], Oxford Hip Score (OHS) [19], Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) [20], or a modified University of California Los Angeles Activity (UCLA) scale [21].
From a radiological point of view, standard post-operative x-rays are taken routinely. These include an anteroposterior (AP) radiograph of the pelvis and a lateral of the hip (Fig. 4). These initial radiographs are used to assess satisfactory positioning of the components and exclude any complications such as fractures. They also act as a baseline with which future serial radiographs can be compared. Although there is some variation in the timing of follow-up, in general, radiographs are taken at 4–6 weeks, 3–6 months, and at 1-year intervals after this.

Immediate post-op AP (a) and lateral (b) radiographs of the Birmingham Hip Resurfacing in a 55-year-old patient. This radiograph shows both the cemented femoral component (note that the cement is within the metal cap of the femoral component and does not extend to the stem and therefore is not visible) and the uncemented acetabular component. The femoral neck is preserved
An AP radiograph can be used to assess the orientation of the components in the coronal plane. The angle of inclination is the angle between a horizontal line drawn tangential to the ischial tuberosities (or the inter-teardrop line) and a line drawn across the opening of the acetabular component (Fig. 5). The valgus/varus orientation of the femoral component can also simply be measured relative to the axis of the femoral neck (Fig. 5). Similarly, on a lateral radiograph, the angle of planer anteversion can be determined by the angle between a line drawn against the opening of the acetabular component and a vertical reference line (Fig. 6), although this can be somewhat inaccurate if the functional position of the pelvis is not known.

Normal postoperative AP pelvis showing measurement of angle of inclination on the right hip and the relative valgus position of the femoral component on the left hip (dashed line)

Planer anteversion as measured on a standard lateral postoperative x-ray
In the AP plane, it is generally recommended that the femoral component is placed in a relative valgus position of 5–10° (Fig. 5), while avoiding notching of the superolateral cortex of the femoral neck [22, 23]. The acetabular component is placed at 40±10° of inclination (Fig. 4) and 15±10° of anteversion (Fig. 6), as described by Lewinnek et al. [24]. Intra-operatively, this is assessed both with the instrumentation provided and also the degree of anteversion can be guided by the transverse acetabular ligament. An important point of consideration is that hip resurfacings create a relatively small head-to-neck ratio compared to total hip arthroplasty, and therefore accurate positioning is important, as inaccuracies can lead to increased risk of femoral neck impingement resulting in abnormal loading patterns (so-called edge loading) and even femoral neck fracture. Accurate surgery is therefore critical in achieving a good clinical and functional outcome.
Complications of HRA and imaging strategies
Pain following hip resurfacing can occur and the cause of the pain can be difficult to identify. However, an attempt to elucidate this should be made, as a number of causes of failure have been identified and these include fractures, loosening of the femoral or acetabular component of the prosthesis, hip impingement, metal hypersensitivity, and iliopsoas tendinopathy. Although clinical assessment of the pain is critical in directing further investigation and excluding other causes, imaging plays an important role in assessing pain, and with other investigations (blood tests, etc.) the cause of pain may be identified.
Ramakrishnan et al. [25] described a system of illustrating the abnormalities found on radiography around the hip resurfacing components. Abnormalities around the acetabular component are described according to Charnley zones [26]; abnormalities around the femoral stem are divided into superior, tip, and inferior zones [27]; in addition, a new zonal system was used to describe the bone response and remodeling in the proximal femur (Fig. 7).

A new zonal system with five femoral zones (A, B, I, II, and III) was devised to analyze the proximal femur to study the bone remodeling effects of HR. Zones A and B refer to the superior and inferior areas of the neck. The other three zones represent the proximal, lateral, and medial areas of the femur in the AP view (reprinted from Ramakrishnan et al. [21], with permission from Elsevier)
Femoral neck narrowing
After hip resurfacing, the femoral neck can narrow [28], and in some series this has been reported to occur in up to 70% of patients [28, 29]. Although the etiology of this phenomenon is unknown, factors implicated include vascular damage to the femoral head/neck at the time of operation, impingement, stress shielding and remodeling or even an inflammatory response to wear particles from the metal on metal bearing surfaces. Although it has been suggested that femoral neck narrowing stabilizes after the first 3 years, it would be reasonable to monitor patients longer, particularly if narrowing is rapid or progressive (Fig. 8).

Radiographs of a 54-year-old male at 4 months (a), and 39 months (b) post-op showing clear evidence of femoral neck narrowing. There is also some subsidence of the femoral component and a change in the angle between the femoral peg and the femoral shaft can be noted. (c) Collapse of the femoral component at 42 months requiring revision to total hip arthroplasty
Implant subsidence and loosening
Radiographic monitoring is also important in identifying changes in the angle between the peg of the femoral component and the femoral shaft, which may indicate progressive failure. In this way, subsidence (i.e., migration of the femoral component relative to the femur) of the implant can also be assessed, and this may indicate instability of the femoral component, which may for example be secondary to avascular necrosis of the femoral head (Fig. 8).
Radiolucent lines around the femoral peg may indicate loosening of the prosthesis. Amstutz et al. [27] described a classification system to systematically record progressive changes for both the acetabular component and the femoral peg. However, it is important to distinguish between radiolucencies and sclerotic or reactive lines [30] (Fig. 9), which are not thought to be associated with an adverse outcome. Similarly, the so-called pedestal sign, which is a sclerotic line commencing at the tip of the stem and extending symmetrically towards the head for a variable distance may be observed [31]; in some series this has not been associated with adverse outcome [31] although others have shown a clear progression of the pedestal sign to subsequent failure of the femoral component [32].

Radiograph of a 43-year-old male at 42 months post-op, showing a reactive line (arrow) around the inferomedial aspect of the femoral peg. The patient was pain free and remained very active in subsequent follow-up
Osteolysis around either the femoral component or the acetabular component can occur (Fig. 10). This may be related to metal sensitivity or be wear-particle induced and therefore warrants regular follow-up and sometimes further investigation. CT is particularly useful in identifying osteolysis particularly around the complex anatomy of the acetabular component. In contrast to plain radiography, which may only show larger areas of osteolysis, CT can be used to identify small areas of osteolysis and also allows the extent of this to be measured accurately [33, 34]. The characteristic features of osteolysis are well-demarcated lucencies adjacent to the components and the absence of osseous trabeculae. A number of factors have been implicated in contributing to femoral component loosening, including female gender, large femoral head cysts, and small component size [27]. Furthermore, surgical factors such as cementing techniques have also been associated with loosening, with insufficient cement penetration [27] or thermal necrosis due to cement penetration resulting in femoral component loosening [35].

a Radiograph showing large cyst around acetabular component (black arrow) at 7 years post-op in a 51-year-old male. Cystic change can also be seen around the proximal stem on the lateral side (white arrow). b CT confirming large periacetabular cyst
In addition to loosening of the femoral component, the acetabular component can also fail (Figs. 11c, 12), which may be due to inadequate initial fixation or even secondary to impingement on the femoral neck. Acetabular component loosening has also been associated with male sex and a high body mass index (BMI) [36]. Patients who are found to have a loose component are treated operatively with revision of the loose component.

a Initial post-operative radiograph demonstrating notching of the superolateral cortex in a 61-year-old female. Follow-up radiograph (b) shows a fracture line propagating from the superior implant-neck junction. This was treated conservatively. However, the acetabular component failed subsequently (c). Also note the scalloping of the inferomedial femoral neck which has occurred secondary to impingement on the displaced acetabular component

AP (a) and lateral (b) radiographs of a displaced acetabular component in a 50-year-old male
Fracture
Fracture of the femoral (Figs. 11b, 13) neck after hip resurfacing is one of the most common complications, and is unique to this type of arthroplasty. Femoral neck fracture occurs in 1.46% [37] of cases although higher rates have been reported [38]. Risk factors associated with femoral neck fracture include female sex, reduced bone density, poor surgical technique including notching of the superior lateral femoral cortex (Fig. 11a), relative varus placement of the femoral component, inadequate seating of the femoral component, and inaccurate direction of impaction on the implant [22, 23, 37, 38]. As previously described, the femoral component should be placed in a relative valgus position, however, care needs to be taken, as this may cause notching of the superolateral cortex. If this happens, then there is increased risk of fracture of the femoral neck (Fig. 13). Femoral neck fractures are generally an early complication presenting acutely. However, in some cases, patients may present with hip pain prior to fracturing [37], or have an occult fracture. It is therefore essential that these patients are assessed and investigated thoroughly and managed appropriately.

Fracture of the femoral neck in a 63-year-old male at 2 months post-op (a) that required conversion to a total hip arthroplasty (b)
Impingement
Groin pain after HRA may occur secondary to impingement of the femoral neck on the acetabular component resulting in femoral neck scalloping (Fig. 14) seen on post-operative AP or lateral radiographs [28, 29, 38, 39]. The risk of impingement after HRA is greater because of the reduction in the head-to-neck ratio and preservation of the native femoral neck. Other factors that can make impingement more likely include abnormal anterior protrusion of the femoral neck, reduced anterior femoral head-neck offset, which is particularly true in patients with arthritis secondary to femoroacetabular impingement (FAI), bony deformity of the proximal femur, and component malpositioning for example an inadequately anteverted or indeed a retroverted acetabular component or posterior translation of the femoral component [39].

Lateral radiographs demonstrating scalloping of the femoral neck both anteriorly and posteriorly (Reproduced with permission from Ball ST, Schmalzried TP: Posterior femoroacetabular impingement (PFAI) after hip resurfacing arthroplasty. Bull NYU Hosp Jt Dis. 2009;67(2):173–6; www.nyuhjdbulletin.org)
It is essential that every effort is made in the preoperative planning and intraoperatively to reduce the likelihood of impingement. Any bony deformities including femoral neck osteophytes should be identified and addressed at the time of surgery. Restoration of the head-neck offset can be achieved by placing the acetabular component slightly anteriorly, particularly if the pre-operative femoral head-neck offset ratio is less than 0.15 (this can be estimated from a cross-table lateral radiograph), which is consistent with FAI [39]. Furthermore, the surgeon must ensure adequate anteversion of the acetabular component to prevent anterior impingement on flexion of the hip.
Iliopsoas tendinopathy
Iliopsoas tendinopathy is a well-recognized cause of groin pain after conventional THA with a reported 5% of patients with a painful THA having this condition [40]. Similarly, patients undergoing HRA may also suffer from this condition, where the iliopsoas tendon impinges over the anterior part of the acetabular component. Patients can be predisposed to this by malpositioning of the component or oversized implants leading to an increased anterior prominence. The acetabular component in HRA is generally more hemispherical than the acetabular component of a conventional THA and this may make iliopsoas impingement more likely due to uncovering of the component [41]. In addition, the loss of anterior head-neck offset and anterior osteophytes in the preserved femoral neck may contribute to iliopsoas tendinopathy.
Diagnosis of iliopsoas tendinopathy is based on both clinical and radiological evaluation, with MRI or ultrasound. Treatment should start with conservative approaches including physiotherapy and non-steroidal anti-inflammatories. Injection of local anesthetic and steroids is often used for symptomatic relief and as a diagnostic test. Surgical intervention to correct any underlying causes may be necessary and occasionally surgical tendon release may be required [40].
Metal hypersensitivity
A particular disadvantage of metal-on-metal resurfacing arthroplasty is the release of large amounts of very small wear particles and metal ions. The long-term biological consequences of the exposure to these cobalt (Co) and chromium (Cr) ions remain largely unknown, although various consequences have been suggested. Co and Cr levels may in turn be influenced by the type, design, and positioning of the implant.
The prevalence of adverse reactions to metal debris has been reported as high as 3% [42] with patients presenting with unexplained hip pain, spontaneous dislocation, neurologic symptoms, or even a palpable mass. Initial radiographic imaging may be normal or only show some periprosthetic osteolysis. Consequently, these patients with MoM HRA require full investigation including CT, MRI, and whole-blood Co and Cr levels [43]. When a diagnosis of an adverse reaction has been made, then these patients should be treated by revision arthroplasty and removal of the MoM-bearing surfaces.
From a pathophysiological point of view, a spectrum of changes have been described within the periprosthetic tissues of patients who have undergone MoM hip arthroplasty. These include tissue necrosis, a perivascular lymphocyte infiltrate, and a macrophage response to wear particles. These reactions are thought to be secondary to either a hypersensitivity reaction or a direct cytotoxic effect [44–47], or indeed a combination of the two [48]. The term aseptic lymphocytic vasculitis-associated lesions (ALVAL) has been used to describe these features [46]. Mahendra et al. [48] observed coagulative necrosis around failed MoM HRA, a potential explanation for which may be a form of vasculitis. Soft tissue inflammatory masses or fluid collections have been termed ‘pseudotumors’ and are most commonly diagnosed and best described with MRI [43, 49]. Toms et al. [42] reported that the most common periprosthetic soft tissue abnormality seen on MRI comprised of intermediate T1W signal, and a large proportion also consisted of hyperintense fluid-like signal on T2W with an irregular low signal periphery varying from 1 to 5 mm in thickness. There were also two cases where the abnormal areas were isointense. They also reported muscle atrophy of the gluteus medius and minimus in over half the cases. Muscle edema was also reported but the significance of this was uncertain.
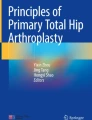
CT may be helpful in identifying soft tissue masses or collections (Fig. 15), although magnetic resonance imaging (MRI) plays a significant role in this. In MoM HRA, the positioning of both the femoral component and the acetabular component is particularly important, as inaccuracies have been associated with various complications including high metal ion levels [50]. 3D CT (Fig. 3) can be used to accurately assess the position of the components, including the degree of anteversion and the inclination of the acetabular component as well as the version and stem shaft angle of the femoral head.

a Transverse CT (with soft tissue window). b Transverse T2-weighted MRI. c Coronal STIR MRI. d Coronal T1-weighted MRI. e Ultrasound image. This 65-year-old man presented 8 years after a Birmingham resurfacing of the left hip and with a painless swelling in the groin. There is a well-defined mass (arrow) seen on all images lying anterior to the prosthesis. On the MR scan, the mass has a low signal margin with heterogeneous signal centrally on both T1- and T2-weighted images. The appearances are entirely in keeping with an inflammatory mass associated with metal hypersensitivity reaction
Conclusions
With the projected increase in patients undergoing metal-on-metal hip resurfacing, particularly in the relatively younger population, the number of patients presenting with symptoms of an adverse outcome will also increase. Traditional radiographic evaluation of the HRA is inadequate, as HRA has different modes of failure, which may be related to wear of the MoM-bearing surfaces with high levels of cobalt and chromium and an adverse reaction to high levels of metal wear debris. Radiological investigation should therefore include CT ± 3D reconstruction and MARS MRI.
Notes
The Dupuy system is currently withdrawn for further testing as they have had a higher revision rate than would be expected.
References
Dorr LD, Kane 3rd TJ, Conaty JP. Long-term results of cemented total hip arthroplasty in patients 45 years old or younger: a 16-year follow-up study. J Arthroplasty. 1994;9:453–6.
Joshi AB, Porter ML, Trail IA, Hunt LP, Murphy JC, Hardinge K. Long-term results of Charnley low-friction arthroplasty in young patients. J Bone Joint Surg Br. 1993;75(4):616–23.
National Joint Registry 6th Annual Report. Available at: http://www.njrcentre.org.uk/NjrCentre/LinkClick.aspx?fileticket=V5%2bELEMfw20%3d&tabid=86&mid=523. Accessed 13 July 2010.
Silva M, Lee KH, Heisel C, Dela Rosa MA, Schmalzried TP. The biomechanical results of a total hip arthroplasty. J Bone Joint Surg Am. 2004;86-A(1):40–6.
Heilpern GN, Shah NN, Fordyce MJ. Birmingham Hip Resurfacing arthroplasty: a series of 110 consecutive hips with a minimum five-year clinical and radiological follow-up. J Bone Joint Surg Br. 2008;90(9):1137–42.
Steffen RT, Pandit HP, Palan J, et al. The five-year results of the Birmingham Hip Resurfacing arthroplasty: an independent series. J Bone Joint Surg Br. 2008;90(4):436–41.
Rahman L, Muirhead-Allwood SK, Alkinj M. What is the midterm survivorship and function after hip resurfacing? Clin Orthop Relat Res. 2010 Jun 24. [Epub ahead of print]
Treacy RB, McBryde CW, Pynsent PB. Birmingham Hip Resurfacing arthroplasty: a minimum follow-up of five years. J Bone Joint Surg Br. 2005;87-B:167–70.
Back DL, Dalziel R, Young D, Shimmin A. Early results of primary Birmingham Hip Resurfacings: an independent prospective study of the first 230 hips. J Bone Joint Surg Br. 2005;87:324–9.
Burroughs BR, Hallstrom B, Golladay GJ, Hoeffel D, Harris WH. Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J Arthroplasty. 2005;20(1):11–9.
Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. RadioGraphics. 2004;24:1679–91.
Sofka CM, Potter HG. MR imaging of joint arthroplasty. Semin Musculoskelet Radiol. 2002;6:5–17.
Cho ZH, Kim DJ, Kim YK. Total inhomogeneity correction including chemical shifts and susceptibility by view angle tilting. Med Phys. 1998;15(1):7–11.
Lu W, Pauly KB, Gold GE, Pauly JM, Hargreaves BA. SEMAC: Slice Encoding for Metal Artifact Correction in MRI. Magn Reson Med. 2009;62(1):66–76.
Butts K, Pauly JM, Gold GE. Reduction of blurring in view angle tilting MRI. Magn Reson Med. 2005;53(2):418–24.
Harris CA, White LM. Metal artifact reduction in musculoskeletal magnetic resonance imaging. Orthop Clin N Am. 2006;37:349–59.
Lee MF, Kim S, Lee SA, et al. Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multidetector CT. RadioGraphics. 2007;27:791–803.
Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty: an end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51-A:737–55.
Dawson J, Fitzpatrick R, Carr A, Murray D. Questionnaire on the perceptions of patients about total hip replacement. J Bone Joint Surg Br. 1996;78-B:185–90.
Bellamy N, Buchanan W, Goldsmith C, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15(12):1833–40.
Daniel J, Pynsent PB, McMinn DJW. Metal-on-metal resurfacing of the hip in patients under the age of 55 years with osteonecrosis. J Bone Joint Surg Br. 2004;86-B:177–84.
Beaul’e PE, Lee JL, Le Duff MJ, Amstutz HC, Ebramzadeh E. Orientation of the femoral component in surface arthroplasty of the hip. A biomechanical and clinical analysis. J Bone Joint Surg Am. 2004;86:2015–21.
Anglin C, Masri BA, Tonetti J, Hodgson AJ, Greidanus NV. Hip resurfacing femoral neck fracture influenced by valgus placement. Clin Orthop Relat Res. 2007;465:71–9.
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60-A:217–20.
Ramakrishnan R, Jaffe WL, Kennedy WR. Metal-on-metal hip resurfacing radiographic evaluation techniques. J Arthroplasty. 2008;23(8):1099–104.
DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976;121:20–32.
Amstutz HC, Beaulé PE, Dorey FJ, Le Duff MJ, Campbell PA, Gruen TA. Metal-on-metal hybrid surface arthroplasty: two to six-year follow-up study. J Bone Joint Surg Am. 2004;86-A(1):28–39.
Hing CB, Young DA, Dalziel RE, Bailey M, Back DL, Shimmin AJ. Narrowing of the neck in resurfacing arthroplasty of the hip: a radiological study. J Bone Joint Surg Br. 2007;89:1019–24.
Back DL, Dalziel R, Young D, Shimmin A. Early results of primary Birmingham Hip Resurfacings. J Bone Joint Surg Br. 2005;87-B:324–9.
Freeman MA, MacInnes T, Revell PA. The histology of “reactive lines” in wellfixed components. J Arthroplasty. 2003;18:224–6.
Pollard TC, Baker RP, Eastaugh-Waring SJ, Bannister GC. Treatment of the young active patient with osteoarthritis of the hip. A five- to seven-year comparison of hybrid total hip arthroplasty and metal-on-metal resurfacing. J Bone Joint Surg Br. 2006;88(5):592–600.
Madhu TS, Akula MR, Raman RN, Sharma HK, Johnson VG. The Birmingham Hip Resurfacing prosthesis. An Independent single surgeon’s experience at 7-year follow-up. J Arthroplasty. 2010 Jan 5. [Epub ahead of print].
Kitamura N, Pappedemos PC, Duffy 3rd PR, et al. The value of anteroposterior pelvic radiographs for evaluating pelvic osteolysis. Clin Orthop Relat Res. 2006;453:239–45.
Leung S, Naudie D, Kitamura N, Walde T, Engh CA. Computed tomography in the assessment of periacetabular osteolysis. J Bone Joint Surg Am. 2005;87:592–7.
Morlock MM, Bishop N, Ruther W, et al. Biomechanical, morphological, and histological analysis of early failures in hip resurfacing arthroplasty. Proc Inst Mech Eng H. 2006;220(2):333–44.
Kim PR, Beaule PE, Laflamme GY, Dunbar M. Causes of early failure in a multicenter clinical trial of hip resurfacing. J Arthroplasty. 2008;23(6 Suppl 1):44–9.
Shimmin AJ, Back D. Femoral neck fractures following Birmingham Hip Resurfacing: a national review of 50 cases. J Bone Joint Surg Br. 2005;87:463–4.
Shimmin A, Beaulé PE, Campbell P. Metal-on-metal hip resurfacing arthroplasty. J Bone Joint Surg Am. 2008;90(3):637–54.
Ball ST, Schmalzried TP. Posterior femoroacetabular impingement (PFAI) - after hip resurfacing arthroplasty. Bull NYU Hosp Jt Dis. 2009;67(2):173–6.
Johnston CA, Wiley JP, Lindsay DM, Wiseman DA. Iliopsoas bursitis and tendinitis. A review. Sports Med. 1998;25(4):271–83.
Bin Nasser A, Beaulé PE, O’Neill M, Kim PR, Fazekas A. Incidence of groin pain after metal-on-metal hip resurfacing. Clin Orthop Relat Res. 2010;468(2):392–9.
Toms AP, Marshall TJ, Cahir J, Tucker JK, et al. MRI of early symptomatic metal-on-metal total hip arthroplasty: a retrospective review of radiological findings in 20 hips. Clin Radiol. 2008;63(1):49–58.
Hart AJ, Sabah S, Henckel J, et al. The painful metal-on-metal hip resurfacing. J Bone Joint Surg Br. 2009;91(6):738–44.
Doorn PF, Mirra JM, Campbell PA, Amstutz HC. Tissue reaction to metal on metal total hip prostheses. Clin Orthop Relat Res. 1996;329:S187–205.
Davis AP, Willert HG, Campbell PA, Learmonth ID, Case CP. An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements. J Bone Joint Surg Am. 2005;87:18–27.
Willert HG, Buchhorn GH, Ing D, et al. Metal-on-metal bearings and hypersensitivity inpatients with artificial hip joints; A clinical and histomorphological study. J Bone Joint Surg Am. 2005;87:28–36.
Korovessis P, Petsinis G, Repanti M, Repantis T. Metallosis after contemporary metal-on-metal total hip arthroplasty: five to nine-year follow-up. J Bone Joint Surg Am. 2006;88:1183–91.
Mahendra G, Pandit H, Kliskey K, Murray D, Gill HS, Athanasou N. Necrotic and inflammatory changes in metal-on-metal resurfacing hip arthroplasties. Acta Orthop. 2009;80(6):653–9.
Fang CS, Harvie P, Gibbons CL, Whitwell D, Athanasou NA, Ostlere S. The imaging spectrum of peri-articular inflammatory masses following metal-on-metal hip resurfacing. Skeletal Radiol. 2008;37(8):715–22.
Hart AJ, Buddhdev P, Winship P, Faria N, Powell JJ, Skinner JA. Cup inclination angle of greater than 50 degrees increases whole blood concentrations of cobalt and chromium ions after metal-on-metal hip resurfacing. Hip Int. 2008;18(3):212–9.
Acknowledgements
The work of Dr. Margaret Hall-Craggs was undertaken at University College London Hospital/University College London, which receives funding from the Department of Health’s National Institute for Health Research Comprehensive Biomedical Research Centre funding scheme. The views expressed in this publication are those of the authors and not necessarily those of the United Kingdom Department of Health.
Conflict of Interest
The authors declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rahman, L., Hall-Craggs, M. & Muirhead-Allwood, S.K. Radiology of the resurfaced hip. Skeletal Radiol 40, 819–830 (2011). https://doi.org/10.1007/s00256-010-1081-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-010-1081-3