
Abstract
Castleman’s disease (CD), a rare benign disease characterized by lymphoid hyperplasia, typically arises in the mediastinum as a solitary tumor. We describe herein a rare case of intramuscular CD occurring in the left deltoid in a 28-year-old woman. The present case is instructive in the differential diagnosis of primary soft tissue tumors, for which the possibility of CD should be considered.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Castleman’s disease (CD) is a relatively uncommon benign disease that is characterized by lymphoid hyperplasia. CD may occur in any area where lymphoid tissue is normally found. Extranodal CD, particularly intramuscular CD, is exceedingly rare. We describe herein a case of intramuscular CD in the deltoid and discuss with reference to the literature.
Case report
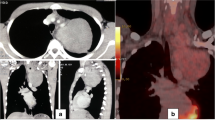
A 28-year-old woman with no history of major illness presented with a 3-year history of a painless, elastic soft mass in the left shoulder. She had no other symptoms. Regular laboratory data showed no abnormality. Magnetic resonance imaging (MRI) revealed an intramuscular tumor in the posterior area of the left deltoid, measuring 5.8 × 4.7 × 3.7 cm in size and displaying intermediate (higher-than-muscle) intensity on T1-weighted imaging (Fig. 1a), high intensity on T2-weighted imaging (Fig. 1b) and diffuse enhancement on gadolinium-enhanced T1-weighted fat-suppressed imaging (Fig. 1c). Magnetic resonance angiography showed a hypervascular tumor fed by the posterior circumflex humeral artery (Fig. 1d). These MRI findings suggested that the lesion in the deltoid was a primary hypervascular soft tissue tumor. We initially suspected this tumor to be benign, such as a hemangioma, because clinical findings did not suggest malignancy. We decided to perform an excisional biopsy to avoid excessive bleeding by incisional biopsy.

Magnetic resonance imaging shows an intramuscular tumor in the posterior area of the left deltoid, displaying a intermediate intensity on T1-weighted imaging (axial view), b high intensity on T2-weighted imaging (axial view), and c diffuse enhancement on gadolinium-enhanced T1-weighted fat-suppressed imaging (sagittal view). d Magnetic resonance angiography shows the hypervascular tumor fed by the posterior circumflex humeral artery
At surgery, the tumor involved the surrounding degenerated muscle fibers. The tumor showed a rich circulation and bleeding was observed at excision. Complete en-bloc excision was performed.
Microscopic examination of the excised specimen showed histopathological features of hyaline vascular-type CD (HVCD); that is, irregular lymphatic follicles showed a concentric, onion skin-like arrangement of lymphocytes in the mantle zone, and an aberrant and shrunken germinal center, lacking centroblasts and centrocytes, penetrated by a small, hyalinized vessel (angiosclerosis; Fig. 2a, b). On immunohistochemical staining, lymphocytes showing onion skin-like arrangement were positive for CD20 (Fig. 2c) and CD79a (Fig. 2d), which are markers of B cells. Follicular dendritic cells showing positive immunoreactivity for CD21 were observed in the lymph follicle (Fig. 2e). Plasma cells, identified by positivity for CD138, were rarely observed in the extra-follicular area and not observed at all in the lymphatic follicles. Immunohistochemical findings for CD34 (as a marker of endothelium) showed hyperplasia of small vessels and invasion into the germinal center through the mantle zone (Fig. 2f). Histological differential diagnosis of extranodal lymphoproliferative disorder includes only small number of diseases: low-grade lymphoma, especially MALT (mucosa-associated lymphoid tissue)-type lymphoma, follicular lymphoma, and CD. Immunohistochemical analysis did not show monoclonal immunoglobulin and did not suggest the diagnosis of malignant lymphoma. Thus, we histopathologically diagnosed a specimen from excision biopsy as HVCD.

a Histological section of the excised biopsy specimen shows hyperplasia of the irregular lymphatic follicles (hematoxylin-eosin stain, ×40). b Lymphatic follicles show a concentric, onion skin-like arrangement of lymphocytes in the mantle zone, with an aberrant and shrunken germinal center penetrated by a small, hyalinized vessel (hematoxylin-eosin stain, ×200). c, d Lymphocytes show an onion skin-like arrangement in the mantle zone with positive results for B-cell markers CD20 (c) and CD79a (d; immunoperoxidase stain, ×200). e CD21 (a marker of follicular dendritic cells) shows positive results in the mantle zone (immunoperoxidase stain, ×200). f CD34 (a marker of endothelium) shows hyperplasia of small vessels and invasion into the germinal center through the mantle zone (immunoperoxidase stain, ×200)
After histological diagnosis, radiological analyses (whole-body computed tomography and whole-body gallium scintigraphy) were performed to exclude the diagnosis of multicentric-type CD. However, these analyses revealed no findings of other tumorous regions or swollen lymph nodes elsewhere in the body. Moreover, additional laboratory tests including serum soluble interleukin-2 receptor level, anti-human immunodeficiency virus type 1 antibody, and bone marrow aspiration biopsy showed normal results. On the basis of the aforementioned findings, intramuscular unicentric HVCD of the left deltoid was finally diagnosed. Although the patient has received no additional therapy (chemo- or radiotherapy), she has shown no evidence of disease as of 3 years postoperatively.
Discussion
Castelman’s disease was first described by Castleman et al. [1, 2] as a localized mediastinal lymph node hyperplasia resembling a thymoma. This entity has a number of descriptive synonyms, including “angiomatous lymphoid hamartoma,” “angiofollicular hyperplasia,” and “giant lymph node hyperplasia” [3]. CD is currently classified into three variants: unicentric HVCD (representing 72% of all CD cases); unicentric plasma cell-type CD (18%); and multicentric-type CD (10%) [4]. As the etiology of CD has not been definitively established, whether CD variants represent different ends of the same pathological spectrum or entirely separate disease entities remains controversial.
Extranodal CD, particularly intramuscular CD, is extremely rare. To the best of our knowledge, only 8 cases of intramuscular CD have been reported in the English-language literature (Table 1) [5–12]. Clinical courses of all 9 cases of intramuscular CD, including the present case, have been favorable. Pathological findings for previously reported cases have included 4 cases of HVCD (as in the present case) [9–12] and 4 cases of unknown pathology (data unavailable) [5–8]. We speculate that these 4 cases of unknown pathological type might represent HVCD, given the favorable prognosis and lack of systemic clinical manifestations. Symptoms of previous cases have typically included a painless mass (excluding 1 case of a painful mass) and prognoses were favorable following surgical resection. These findings correspond with exemplary HVCD. The present case fulfilled characteristic findings of HVCD: a solitary painless mass without constitutional symptoms such as fever, nightsweats, or malaise; radiological findings of a solitary hypervascular mass; pathological findings representative of HVCD; and favorable prognosis following surgical excision.
Castleman’s disease generally occurs in young adults without any obvious gender predilection [4]. A review of 9 cases, including the present case, found that intramuscular CD shows a predilection for women (7 out of 9 cases), but no characteristic age distribution. Intramuscular CD can occur at various sites. Two cases occurred in the trunk and 7 cases occurred in the extremities. The shoulder girdle was the predominant site of intramuscular CD, particularly in 3 cases (including the present case) of intramuscular CD of the deltoid [5, 8].
Radiological findings of CD tend to show hypervascularity reflecting histological hypervascularity. This radiological hypervascular finding is nonspecific to CD. Including CD as a differential diagnosis of hypervascular tumor is thus quite difficult because of the rarity of this entity, particularly solitary extranodal CD such as in soft tissue. Radiological differential diagnosis of solitary hypervascular soft tissue tumor includes many tumors, such as vascular tumors, extrapleural solitary fibrous tumors, malignant lymphoma, metastatic tumors including soft tissue metastasis of renal cell carcinoma (hypernephroma), and soft tissue sarcoma. Regrettably, extranodal CD is extremely rare and the possibility of intramuscular CD is difficult to consider. When diagnosing primary intramuscular tumors, the possibility of CD should be considered. Although no previous reports have described multicentric-type CD including intramuscular lesions, radiological analyses of the whole body to identify other lesions, particularly in the mediastinum or cervical lymph nodes in consideration of the possibility of multicentric CD, are needed when a diagnosis of CD is established. As multicentric-type CD may follow an aggressive natural history (progression to malignant lymphoma [13]), more aggressive treatment with chemotherapy including monoclonal antibodies to interleukin-6 (tocilizumab) is needed [3, 4].
In conclusion, we have described a rare case of solitary intramuscular HVCD of the deltoid. The present case is instructive in the differential diagnosis of primary soft tissue tumor, particularly in intramuscular tissue, and the possibility of CD must be considered in such cases. Diagnosing CD without pathological findings is difficult; however, once a pathological diagnosis of CD is established, the possibility of multicentric-type CD must be considered and radiological analyses of the entire body, particularly the lymph nodes, are needed to identify any other lesions.
References
Castleman B, Towne VW. Case records of the Massachusetts General Hospital: case no. 40231. N Engl J Med. 1954;250:1001–5.
Castleman B, Iverson L, Menendez VP. Localized mediastinal lymphnode hyperplasia resembling thymoma. Cancer. 1956;9:822–30.
Waterston A, Bower M. Fifty years of multicentric Castleman's disease. Acta Oncol. 2004;43:698–704.
Casper C. The aetiology and management of Castleman disease at 50 years: translating pathophysiology to patient care. Br J Haematol. 2005;129:3–17.
Cohen H. Tumor-like proliferations of lymphoid tissue; occurrence in deltoid muscle and mediastinum. J Mt Sinai Hosp N Y. 1957;24:750–60.
Zettergren L. Probably neoplastic proliferation of lymphoid tissue (follicular lympho-reticuloma). Reports of four cases with a survey of literature. Acta Pathol Microbiol Scand. 1961;51:113–26.
Lattes R, Pachter MR. Benign lymphoid masses of probable hamartomatous nature. Analysis of 12 cases. Cancer. 1962;15:197–214.
Abell MR. Lymphoid hamartoma. Radiol Clin North Am. 1968;6:15–24.
Rooney RC, Pitcher JD. Castleman's disease in the extremity. Am J Orthop. 1998;27:373–4.
Williams HR, Millner PA, Coral A. Castleman's disease of the erector spinae muscle. Skeletal Radiol. 1998;27:637–40.
Fiel-Gan MD, Voytek TM, Weiss RG, Brown RT, Joshi VV. Castleman's disease of the left triceps in a child suspected to be a small round cell tumor of childhood. Pediatr Dev Pathol. 2000;3:286–9.
Kazakov DV, Fanburg-Smith JC, Suster S, et al. Castleman disease of the subcutis and underlying skeletal muscle: report of 6 cases. Am J Surg Pathol. 2004;28:569–77.
Isaacson PG, Campo E, Harris NL. Large B-cell lymphoma arising in HHV8-associated multicentric Castleman disease. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon: International Agency for Research on Cancer; 2008. p. 258–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hakozaki, M., Tajino, T., Yamada, H. et al. Intramuscular Castleman’s disease of the deltoid: a case report and review of the literature. Skeletal Radiol 39, 715–719 (2010). https://doi.org/10.1007/s00256-010-0895-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-010-0895-3