
Abstract
Objective
To find a correlation between the cross-over ratio of the cross-over sign on conventional anteroposterior (AP) pelvic radiographs and retroversion measurements (‘roof-edge angle’ and ‘equatorial-edge angle) on computed tomography (CT) scans. This would facilitate the interpretation of the cross-over sign regarding the amount of acetabular retroversion.
Materials and methods
Correctly projected AP pelvic radiographs (2,925 hips) were examined for the presence of the cross-over sign (COS), and the overlap ratio of the COS was measured. On CT scans of the same patients the ‘roof-edge angle’ (RE angle) and the ‘equatorial-edge angle’ (EE angle) were also calculated.
Results
A statistically significant but only weak relationship could be found between the overlap ratio of the COS and the ‘roof-edge angle’ (P < 0.0001; correlation coefficient −0.486) and between this ratio and the ‘equatorial-edge angle’ (P < 0.0001; correlation coefficient −0.395).
Conclusion
A relationship between the overlap ratio and orientation measurements on CT scans could be found, but it was less strong than expected.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Hips with a retroverted acetabulum have been shown to be associated with a more extensive anterolateral coverage of the femoral head. This aberrant morphologic feature results in abnormal contact between the proximal femur and the anterior acetabular rim and is called femoro-acetabular impingement. The repetitive stress on labrum and acetabular cartilage can lead to early degenerative changes and osteoarthritis of the hip [1–6].
Although retroversion of the acetabulum is not immediately apparent on anteroposterior (AP) pelvic radiographs, it can be detected by the presence of the so-called cross-over sign (COS) [6], which was found to correlate highly with acetabular retroversion in a study by Jamali et al. [7]. This COS is an important finding on radiographs in symptomatic hips when impingement surgery is being considered.
While visualization of the presence of the this sign is highly dependent on correct patient positioning and orientation of the X-ray beam [8], efforts have been made to correlate this finding with certain readings on computed tomography (CT) scans [6]. The COS has also been quantitatively assessed [6], and the actual amount of overlap of anterior and posterior wall has been called the ‘overlap ratio’ [9]. There are no data yet, however, on how the overlap ratio of the cross-over sign correlates with the axial plane retroversion of the acetabulum measured on CT scans.
Our investigation was designed (1) to find a relationship between cross-over ratio of the COS on AP pelvic radiographs and CT retroversion measurements, and (2) to create a nomogram to estimate the degree of retroversion without the need of a CT scan. This would represent an inexpensive and readily available method in clinical practice.
Materials and methods
Patients
AP pelvic radiographs and pelvic CT scans of patients admitted to the R Adams Cowley Trauma Center, Baltimore, USA, were retrieved from the electronic radiological archive. There were 2,964 patients (5,928 hips) who met the primary requirement of having both sets of images available (conventional AP pelvis radiographs and pelvic CT scans), and they were further assessed.
Before any set of conventional radiographs and CT scans were included in the study, they had to be validated for correct patient positioning and radiographic technique to eliminate inadvertent errors of measurements. Malrotation of either the patient or the X-ray beam has been shown to highly influence the appearance of the cross-over sign on radiographs [8] and would certainly also influence CT scan measurements.
Validation of conventional radiographs
Axial plane rotations of the pelvis could increase the cross-over on the side turned away from the source and vice versa. The criterion for a normally rotated pelvis in the axial plane was the alignment of the tip of the coccyx with the middle of the symphysis [10].
Rotation of the pelvis in the sagittal plane could lead to an increased cross-over ratio with increased inclination (more of an inlet view). Increasing reclination (more of an outlet view) could decrease the cross-over ratio. To minimize the possibility of errors in measurements, the distance between the sacrococcygeal joint and the symphysis had to be less than 32 mm in men and 47 mm in women [8].
Rotations only in the frontal plane could be corrected electronically with the picture-archiving communication system (PACS) imaging program, and, therefore, there were no exclusion criteria.
Validation of CT scans
Validation of the CT scans was somewhat more complicated. Sagittal rotation was assumed to be the same as for the conventional radiographs, since the patients remained on the same backboard for both conventional radiograph and CT scans. Correct patient positioning could also be controlled on the ‘localizer’ image of the CT scan, where the same criteria were applied as for the conventional radiographs. Axial rotation was correctable, just like frontal plane rotations in the conventional radiograph, using the PACS imaging program. Rotations in the frontal plane, however, had to be further investigated. For this, a synthetic pelvis model (Sawbones® synthetic bone, model 1301, Pacific Research Laboratories, Vashon, WA, USA) was scanned in rotations at several degrees around the frontal plane. If the pelvis was not rotated more than 5° in the frontal plane the measurements of the ‘roof-edge angle’ (RE angle) and the ‘equatorial-edge angle’ (EE angle) remained constant (see below for description of angles measured). This corresponded to four consecutive CT slices of 3 mm each and three consecutive slices of 5 mm each, respectively. Both acetabular roofs had to be within these margins for inclusion in the CT scan.
All sets of radiographs not meeting these criteria in either the conventional radiographs or CT scans, or both, were excluded from this study.
Of the initial 5,928 hips, 3,003 had to be excluded because they did not meet the aforementioned requirements. There were 2,925 hips remaining for further investigation. The mean age of the patients was 39.6 years, with a range from 14 years to 97 years.
The images were then reviewed by four physicians with different levels of expertise (1 year to several years) who had been trained to read the signs associated with acetabular retroversion prior to the study.
Measurements on conventional radiographs
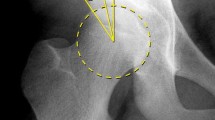
Conventional radiographs were evaluated for the presence of the cross-over sign [6], and, if present, the overlap ratio of the cross-over sign was calculated by the method proposed by Siebenrock et al. [8]. The first measurement (A) extended from the lateral border of the acetabulum to the point where the anterior acetabular rim crossed the posterior rim. The second measurement (B) extended from the lateral border of the acetabulum to its posteroinferior border. The ratio of A:B was calculated and called the overlap ratio of the COS (Fig. 1). Therefore, both the anterior and the posterior acetabular walls had to be recognizable and intact. If this criterion was not met, this was a further reason for us to exclude the acetabulum from the study.

Detailed view of a hip joint illustrating the method we used to calculate the overlap ratio (A:B). Distance A extended from the lateral border of the acetabulum to the cross-over point and distance B extended form the lateral border of the acetabulum to its posteroinferior border
We determined any overlap ratio >1% as a ‘positive’ cross-over sign.
CT measurements
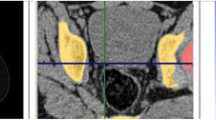
The aforementioned angles on the CT scans were measured using an adapted version of the method originally described by Reynolds et al. [6]: The EE angle was the angle of the acetabular opening at the maximum diameter of the femoral head (Fig. 2a). The RE angle was the angle at the most proximal opening of the acetabulum (Fig. 2b).

a A CT slice at the level of the maximum diameter of the femoral head. A line was drawn from the anterior to the posterior border of the acetabulum, as well as a line representing the sagittal plane. The EE angle was the angle which these two lines subtended. b A CT slice at the most proximal opening of the acetabulum. The angle of a line drawn from the anterior to the posterior border of the acetabulum subtended by a line representing the sagittal plane was called the RE angle
To simplify the method we did not calculate the angle by obtaining contour maps of superimposed CT slices [6], but the angle was measured on the most proximal CT slices, where the femoral head was depicted and could be differentiated from the acetabular roof.
The EE and RE angles were represented by the sagittal plane and a line drawn between the anterior and posterior acetabular rim on the appropriate CT slice.
According to Reynolds et al. [6], the angles were termed ‘positive’ if opening anteriorly and ‘negative’ if opening posteriorly.
Statistical analysis was performed by a statistical consultant using SPSS 13.0 for Windows (SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05, and, for statistical comparisons, the independent-samples t-test was used. To determine the relationship between the measurements on AP pelvic radiographs and the angles calculated on CT scans we used linear regression analysis.
Results
Review of the hips showed a mean RE angle of 8.9°, with a minimum of −33.6° and a maximum of 53.3°. The mean EE angle was 19.0°, with a minimum of −3.9° and a maximum of 38.4°. The overlap ratios of the COS were calculated between 0% and 93%, with a mean value of 13.64%.
When the hips were divided into two groups according to the presence of the cross-over sign, there were differences in the measured angles on the CT scans. The mean RE angle in hips without the cross-over sign was 14.0°; in hips with a positive cross-over sign it was 4.5°. The mean EE angle in cross-over negative hips accounted for 21.0°, while a positive cross-over sign was associated with an EE angle of 17.3° (Table 1).
Statistical evaluation showed significant (P < 0.0001) differences in both RE angles and EE angles, dependent on whether a cross-over sign was present or not. The mean difference in the RE angles between the group with a positive cross-over sign and the group with a negative cross-over sign was 9.5°, and the mean difference between the two groups for the EE angles was 3.7°.
Interestingly, not all hips with a positive cross-over sign also had negative values for the RE angle. With a negative cross-over sign, 91% of the RE angles were positive, while, in the presence of a cross-over sign, still 69% of the RE angles remained positive.
Regarding the correlation between the overlap ratio of the COS and the RE angle and the EE angle, respectively, Spearman’s rho showed statistically significant (P < 0.0001) correlations with the RE angle (−0.486) and the EE angle (−0.395), even though they were not strong.
Linear regression analysis showed the CT angles to depend on the overlap-ratio of the COS:
In addition, a formula was derived to determine the overlap ratio based on the RE and EE angles:
Discussion
In preceding studies the association between a retroverted acetabulum and a higher incidence of early onset osteoarthritis of the hip due to femoroacetabular impingement has been emphasized [1–3, 6, 11, 12]. Efforts have been made to identify retroverted acetabula on AP pelvic radiographs. Reynolds et al. [6] described the cross-over sign as a radiological parameter associated with the aforementioned morphologic anomaly. Several investigations followed to validate this sign. Siebenrock et al. [8] evaluated the effect of pelvic tilt on acetabular retroversion. They could show an increase in the number of hips with signs of retroversion with increasing pelvic inclination. With increasing reclination, the signs of retroversion disappeared. Those results emphasize the importance of the use of standardized pelvic radiographs for correct interpretation of acetabular retroversion. Jamali et al. [7] validated the cross-over sign and declared it to be an extremely reliable parameter to predict a cranial acetabular version of fewer than 4°. To calculate the acetabular version from AP pelvic radiographs a modified version of the method proposed by Meunier et al. [13] was used. They could show a quite constant relationship between the central and the cranial acetabular version. A central anteversion of fewer than 10° was highly correlated with a negative cranial angle, while a central angle of more than 20° was associated with a positive cranial angle. With a central anteversion between 10° and 20°, more than one-third of the acetabula were cranially retroverted. In addition, the authors found significantly lower RE and EE angles in hips with a positive cross-over sign than in hips with no cross-over sign. The cut-off value of 4° to predict a cranial retroversion was determined by the divergence of the X-ray beam.
So far, no studies have been performed to correlate the overlap ratio of the COS with the actual version measured on CT scans. Finding such a relationship would enable one to estimate the version of the acetabulum using an AP pelvic radiograph. Our study was designed to search for such a relationship.
The mean value in our study for the RE angle was 9°, and the EE angle was 19°. These values are in accordance with those presented by Jamali et al. [7]. We then differentiated between the measurements of patients with a positive cross-over sign and those with a negative one. We found a mean RE angle in acetabula with a negative cross-over sign of 14°, which was higher than the 5° presented by Reynolds et al. [6]. A possible explanation for this is the slight methodological difference in determining the plane where the RE angle is measured: Reynolds et al. [6] derived a roof-edge line from a contour map constructed from tracings of the outlines of consecutive 2 mm CT slices, laid over each other. The RE angle was the angle which this line subtended with the sagittal plane. In our study, the RE angle was determined directly from the CT slice showing the most proximal opening of the acetabulum. This adapted method was used to simplify the measurements. The EE angle in cross-over negative hips reached a mean value of 21°, which was comparable to the 20° in the investigation by Reynolds et al. Without a cross-over sign, the mean value for the RE angle was approximately 4°, as opposed to the −17° indicated by Reynolds et al. The EE angle in cross-over positive acetabula was 17°, while Reynolds et al. found 13°. Since Reynolds et al. [6] calculated their angles exclusively from symptomatic patients, more extensive retroversion could be expected. This would also explain the difference between the RE angles with a positive COS found by Reynolds et al. [6] and the values measured in our study. Since we measured the angles in a mixed patient population (unknown whether symptomatic or not), many hips with a slightly positive cross-over sign were identified which might only have had a minimal retroverted acetabular dome. This was reflected in the higher mean RE angles in our investigation.
Based on these findings, we speculate that symptomatic hips have a higher degree of retroversion than asymptomatic hips.
We found that, without a cross-over sign, 91% of the RE angles were positive. Interestingly, the RE angles of 69% of the hips with a positive cross-over sign were still positive, meaning that a positive cross-over sign does not automatically include a retroverted acetabulum. This is in contrast to the results of previous studies [6, 7]. Again, the low threshold to call very small overlap ratios (>1%) ‘positive’ might be an explanation for this.
Although a statistically significant correlation (P < 0.0001) between the overlap ratio of the COS and the RE angle and the EE angle, respectively, was found, the correlation coefficient was only −0.486 for the RE angle and −0.395 for the EE angle, i.e., both correlations were weak. According to the results of previously presented studies, we had expected a stronger relationship between these values. This means that an estimation of the retroversion angle based on the overlap ratio of the COS is possible but remains not very accurate. The resulting r2 values for linear regression ranged between 0.16 and 0.20 and showed that the angles can only be calculated with a very low accuracy. The initially intended nomogram to determine the angles directly from AP pelvic radiographs could, therefore, not be created. Although RE and EE angles decrease with increasing overlap ratio of the COS, a CT scan is still necessary if the exact amount of retroversion is to be determined. For patients with hip pain and a negative pelvic radiograph, magnetic resonance imaging (MRI) is generally used as the second-step imaging modality in the clinical work-up. The CT measurements used in this study are potentially applicable to MRI. Since no data concerning such measurements on MR images are available, further studies are needed to confirm the applicability.
Preceding studies [7] have calculated RE and EE angles from AP radiographs from pelvic specimens and did not measure the angles directly from CT slices. This methodological difference might be another explanation as to why our study did not always agree with preceding studies.
A theoretical weakness of this study is the number of radiograph reviewers. Four different investigators were involved in evaluating the images. To minimize the effect of this confounding factor, they were all carefully instructed by the same physician and were supervised until they were very comfortable with the measurements. Based on 100 radiographs randomly selected for inter-rater comparison, an inter-rater reliability of r = 0.92 with a restricted maximum variance estimation of 0.06% for these measurements could be shown in another part of the study [9].
One additional confounding factor in the determination of acetabular version on computed tomography images could not be eliminated. CT scans at the roof area of the acetabular dome cut the rim obliquely or tangentially. This makes it difficult for one to identify the prominences accurately. The measured angles are therefore less meaningful [14]. To measure the angles more accurately, the above-mentioned method used by Reynolds et al. [6] would have been an option. However, the reconstruction of the acetabulum from contour maps is very time consuming and therefore not (yet) applicable to clinical use. Since we were looking for a readily available way to evaluate the acetabular version, the adopted method was used despite the aforementioned problems.
In summary, this study showed a negative correlation between the overlap ratio of the COS and the RE angle as well as between this ratio and the EE angle measured on CT scans. An increasing overlap ratio of the COS indicated a more retroverted acetabulum. The exact values, however, cannot be calculated with high accuracy if they are based on the overlap ratio.
References
Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop. 2003;417:112–20.
Giori NJ, Trousdale RT. Acetabular retroversion is associated with osteoarthritis of the hip. Clin Orthop. 2003;417:263–9.
Kim WY, Hutchinson CE, Andrew JG, Allen PD. The relationship between acetabular retroversion and osteoarthritis of the hip. J Bone Joint Surg Br. 2006;88:727–9.
Leunig M, Beck M, Dora C, Ganz R. Femoroacetabular impingement: trigger for the development of coxarthrosis. Orthopade. 2006;35:77–84.
Leunig M, Ganz R. [Femoroacetabular impingement. A common cause of hip complaints leading to arthrosis]. Unfallchirurg. 2005;108:9–10, 12–17.
Reynolds D, Lucas J, Klaue K. Retroversion of the acetabulum. A cause of hip pain. J Bone Joint Surg Br. 1999;81:281–8.
Jamali AA, Mladenov K, Meyer DC, Martinez A, Beck M, Ganz R, et al. Anteroposterior pelvic radiographs to assess acetabular retroversion: high validity of the “cross-over-sign”. J Orthop Res. 2007;25:758–65.
Siebenrock KA, Kalbermatten DF, Ganz R. Effect of pelvic tilt on acetabular retroversion: a study of pelves from cadavers. Clin Orthop. 2003;407:241–8.
Werner CML, Copeland CE, Ruckstuhl T, Stromberg J, Seifert B, Turen CH. Prevalence of acetabular dome retroversion in a mixed race adult trauma patient population. Acta Orthop Belg. 2008;74:766–72.
Tannast M, Zheng G, Anderegg C, Burckhardt K, Langlotz F, Ganz R, et al. Tilt and rotation correction of acetabular version on pelvic radiographs. Clin Orthop. 2005;438:182–90.
Banks KP, Grayson DE. Acetabular retroversion as a rare cause of chronic hip pain: recognition of the “figure-eight” sign. Skeletal Radiol. 2007;36 Suppl 1:S108–11.
Jaberi FM, Parvizi J. Hip pain in young adults: femoroacetabular impingement. J Arthroplasty. 2007;22(7 Suppl 3):37–42.
Meunier P, Lefevre C, Le Saout J, Kerboul B, Riot O, Meriot P, et al. A simple method for measuring anteversion of the acetabulum from a frontal radiograph of the hip. J Radiol. 1987;68:799–804.
Tönnis D. Ueber die Aenderung des Pfannendachwinkels der Hüftgelenke bei Dreh- und Kippstellungen des kindlichen Beckens. Z Orthop Grenzgeb. 1962;96:462–78.
Acknowledgements
The authors acknowledge the help given by Prof. Dr. Burkhardt Seifert (Biostatistics Unit, Institute of Social and Preventive Medicine, University of Zurich) with the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Werner, C.M.L., Copeland, C.E., Stromberg, J. et al. Correlation of the cross-over ratio of the cross-over sign on conventional pelvic radiographs with computed tomography retroversion measurements. Skeletal Radiol 39, 655–660 (2010). https://doi.org/10.1007/s00256-009-0854-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-009-0854-z