
Abstract
We present a case of multiple vertebral metastases, with multiple fluid-fluid levels, from a moderately to poorly differentiated carcinoma of unknown origin. We suggest that fluid-fluid levels in multiple vertebral lesions are highly suggestive of bone metastases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fluid-fluid levels in bone lesions are a non-specific finding. They are commonly encountered in aneurysmal bone cysts but, since the first descriptions, have been described in other benign and malignant bone lesions [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11].
We present a case of multiple fluid-fluid levels in the vertebrae. Bone biopsy confirmed the diagnosis of metastases of a moderately to poorly differentiated carcinoma. No primary tumor could be found.
Fluid-fluid levels in metastatic bone lesions are extremely rare and have been reported on magnetic resonance imaging (MRI) only three times in the world literature [4, 5, 6]. The primary tumor was breast carcinoma in two patients and a small cell neuroendocrine tumor in one patient. To our knowledge, based on a search of the world literature, fluid-fluid levels in multiple vertebrae have not previously been reported.
Case report
A 74-year-old woman presented with low back pain, cauda equina syndrome and decreasing strength in both legs. She complained of decreased sensation in the perineum and stress incontinence. Clinical examination revealed a decreased sphincter tonus.
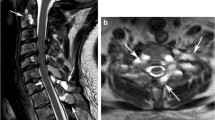
Radiographs of the lumbosacral spine showed a compression fracture of L1. MRI of the spine demonstrated multiple fluid-fluid levels in the vertebrae at the thoracic, lumbar and sacral levels on the T2-weighted images. The upper fluid level was strongly hyperintense compared with the signal of muscle while the lower level was moderately hyperintense (Fig. 1). On T1-weighted images the fluid-fluid levels were less clearly seen due to the isointense appearance of the upper level of the cystic lesion and the slightly hyperintense appearance of the lower level. There was a diffuse low marrow signal on T1-weighted images, reflecting marrow replacement (Fig. 1). The lesions in the sacrum were expansive and caused spinal stenosis. There was bulging of the posterior wall of Th10, Th11 and Th12 without significant dural compression. There was uniform contrast enhancement of the marrow. Several focal vertebral lesions were seen at the cervical level, but it was difficult to demonstrate fluid-fluid levels because T2-weighted images were not obtained at this level.

Sagittal T2-weighted TSE sequence (A, B), T1-weighted SE sequences before (C) and after (D) gadolinium enhancement. Multiple fluid-fluid levels are seen in the thoracic, lumbar and sacral vertebrae (A-C, arrows). The fluid-fluid levels are best seen on T2-weighted images (B, arrow). Following the intravenous injection of gadolinium, there was a uniform enhancement of the bone marrow, probably indicating carcinomatosis (D). The focal lesions with the fluid-fluid levels were less clearly seen
The differential diagnosis included cystic angiomatosis and metastases. Bone biopsy confirmed the diagnosis of metastatic localization of moderately to poorly differentiated carcinoma probably of stomach, kidney, liver or lung origin. Immunohistochemically, the epitheloid cells expressed prekeratin (Fig. 2). They were negative for CK7 and CK20. No primary tumor was found. The patient died 2 months later.

High-power magnification of a bone marrow biopsy showing a solid tumor rest (H&E) (A, arrow) and strong immunohistochemical keratin expression by the neoplastic cells (B, arrows)
Discussion
Fluid-fluid levels have been demonstrated in aneurysmal bone cysts, simple bone cysts, giant cell tumors, chondroblastoma, osteoblastoma, brown tumors, fibrous dysplasia, Langerhans cell histiocytosis, intraosseous ganglion, hemangioma and osteomyelitis [1, 2, 3, 5]. Fluid-fluid levels may also be identified in malignant osseous lesions such as telangiectatic osteosarcoma, malignant fibrous histiocytoma, fibrosarcoma, plasmacytoma and bone marrow metastases [4, 5, 6, 8, 10].
Although fluid-fluid levels can be detected both by radiographs and by computed tomography (CT), MRI is the most useful technique [4]. Depending on the sequence and the stage of the intralesional hemorrhage, a series of signal changes occur both on T1- and on T2-weighted images due to the oxidative denaturation of hemoglobin. In malignant bone lesions, fluid-fluid levels represent tumorous, hemorrhagic and liquefaction necrosis with layers of different weight densities [7, 9]. The high signal on T1-weighted images in aneurysmal bone cysts is thought to be caused by the sedimentation of non-coagulated blood components [2]. Aneurysmal bone cysts and osteoblastoma may contain multiple fluid-fluid levels and do occur in the vertebrae but they usually are solitary lesions. There have been reports of multifocal osteoblastoma and aneurysmal bone cyst but without fluid-fluid levels [12].
To our knowledge this is the first report of multiple fluid-fluid levels in multiple vertebrae. Kickuth et al. have recently reported fluid-fluid levels in bone marrow metastases from a small cell neuroendocrine carcinoma of the urinary bladder in the L4 and L5 vertebral bodies [5]. In our patient the fluid-fluid levels were best seen on the T2-weighted images and were barely visible on T1-weighted images. This has also been reported in giant cell tumors and soft tissue synovial sarcoma [7,11]. The high signal in the upper level was thought to correspond to serous fluid.
The MR changes reflecting marrow replacement are non-specific and are most likely due to carcinomatosis, although the presence of increased fibrovascular tissue with an infiltrate of lymphocytes and plasma cells could not be excluded [13].
Because of the cystic appearance of the focal lesions we included cystic angiomatosis in the differential diagnosis. This is a benign vascular proliferative disease with multiple cystic intramedullary lesions, but fluid-fluid levels have never been reported in this entity [14].
In conclusion, fluid-fluid levels are a non-specific finding, suggesting only the presence of hemorrhagic alterations. Although they cannot be considered diagnostic of any particular type of tumor, it is useful to know that diffuse bone marrow metastases can present with multiple fluid-fluid levels. When multiple fluid-fluid levels are encountered in the vertebrae, metastases is the most likely diagnosis.
References
Hudson TM, Hamlin DJ, Fitzsimmons JR. MR imaging of fluid levels in aneurysmal bone cyst and anticoagulated human blood. Skeletal Radiol 1985; 13:267–270.
Beltran J, Simon DC, Herman L, et al. Aneurysmal bone cyst: MR imaging at 1.5 T. Radiology 1986; 158:689–690.
Woertler K. Benign bone tumours and tumor-like lesions: value of cross-sectional imaging. Eur Radiol 2003; 13:1820–1835.
Nguyen BD, Westra WH, Kuhlman JE. Bone metastasis from breast carcinoma with a fluid-fluid level. Skeletal Radiol 1996; 25:189–192.
Kickuth R, Laufer U, Pannek J, Adamietz IA, Liermann D, Adams S. Magnetic resonance imaging of bone marrow metastasis with fluid-fluid levels from small cell neuroendocrine carcinoma of the urinary bladder. Magn Reson Imaging 2002; 20:691–694.
Sone M, Ehara S, Sasaki M, et al. Fluid-fluid levels in bone and soft tissue tumors demonstrated by MR imaging. Nippon Igaku Hoshasen Gakkai Zasshi 1992; 52:1110–1115.
Tsai JC, Dalinka MK, Eallon MD, Zlatkin MB, Kressel HY. Fluid-fluid level: a nonspecific finding in tumors of bone and soft tissue. Radiology 1990; 175:779–782.
Harter SB, Nokes SR. Plasmacytoma of the sacrum: fluid-fluid levels on MR images. AJR Am J Roentgenol 1995; 165:741–742.
Vilanova JC, Maestro de Leon JL, Aparicio A, Capdevila A. MR imaging of a malignant schwannoma and an osteoblastoma with fluid-fluid levels. Report of two new cases. Eur Radiol 1998; 8:1359–1362.
Jones BC, Sundaram M, Kransdorf MJ. Synovial sarcoma: MR findings in 34 patients. AJR Am J Roentgenol 1993; 161:827–830.
Ilaslan H, Sundaram M, Unni KK, Shives JC. Primary vertebral osteosarcoma: imaging findings. Radiology 2004; 230:697–702.
Adler CP. Multifocal osteoblastoma of the hand. Skeletal radiology 2000; 29:601–604.
Kroon HM, Bloem JL, Holscher HC, Van Der Woude H-J, Reijnierse M, Taminaiau AHM. MR imaging of edema accompanying benign and malignant bone tumors. Skeletal Radiol 1994; 23:261–269.
Clayer M. Skeletal angiomatosis in association with gastro-intestinal angiodysplasia and paraproteinemia. J Orthop Surg 2002; 10:85–88.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bladt, O., Demaerel, P., Catry, F. et al. Multiple vertebral fluid-fluid levels. Skeletal Radiol 33, 660–662 (2004). https://doi.org/10.1007/s00256-004-0819-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-004-0819-1