
Abstract
Primary hydatidosis of muscle is very rare and can cause a variety of diagnostic problems, especially in the absence of typical radiologic findings. This is the report of a case of primary intramuscular hydatid cyst in a 35-year-old woman, who presented with a 1-year history of a painless lump in the distal left thigh. The authors document the pathognomonic water-lily sign that has not previously been reported in a case of intramuscular hydatid disease.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Human hydatid disease is an infestation most commonly caused by the larval stage of Echinococcus granulosus and is prevalent in the Mediterranean region, Central Asia, East Africa, Australia, New Zealand and the southern part of South America [1, 2, 3]. It generally presents as a slowly growing cystic mass [4]; the liver and lungs are frequently affected [1], accounting for approximately 90% of cases [1, 4]. Involvement of other parts of the body such as the kidneys, brain, spleen, thyroid, pancreas, bones, peritoneum, muscles and soft tissues is uncommon [4, 5]. Soft tissue hydatid disease is unusual even in endemic areas [2] and primary hydatidosis of the skeletal muscle is extremely rare [2, 3, 4].
Magnetic resonance (MR) imaging findings of muscle hydatidosis have already been reported in a number of cases [1, 2, 6, 7, 8]. Here, we report an unusual case of a primary intramuscular hydatid cyst that on MR imaging demonstrated the water-lily sign, which is established as pathognomonic in pulmonary and hepatic hydatid disease [9], as well as several other characteristic radiologic features. To the best of our knowledge, based on a search of the world literature, the water-lily sign has not previously been reported in an intramuscular hydatid cyst.
Case report
A 35-year-old woman presented with a 1-year history of a painless mass in her distal left thigh. The patient had previously been referred to several physicians, who had performed a number of needle aspirations. The mass had reportedly reduced in size for a short time after each aspiration, but no definitive diagnosis had been made. Medical, family and surgical history was otherwise unremarkable. On physical examination, there was a 10×7×6 cm, non-tender, smoothly outlined mass on the posteromedial aspect of the distal left thigh. A full range of knee movement was present and there were no signs of an inflammatory process or lymphadenopathy. Hematologic indices, including eosinophil count, were normal.
Radiographs showed a soft tissue mass at the distal left thigh without any calcification. The femur was normal. On MR imaging, a cystic mass was seen in the sartorius muscle. The mass was hypointense on T1-weighted spin echo sequences and hyperintense on T2-weighted gradient echo and fat-saturated images, and it contained smaller cysts, which were hypointense to the surrounding portions of the mass, on all pulse sequences (Fig. 1). The non-enhancing collapsed cyst membrane, which was hypointense on all pulse sequences, was seen in the most dependent part of the mother cyst producing the water-lily sign (Fig. 2). Compared with the rim of daughter cysts, the collapsed membrane was slightly hypointense on T1-weighted spin echo sequences, but of low signal intensity on T2-weighted gradient echo and fat-saturated images. The thin wall surrounding the mother cyst was of low signal intensity on T1-weighted spin echo images, whereas T2-weighted gradient echo axial images showed the rim to consist of two layers: an inner hypointense layer and a peripheral hyperintense layer. Non-homogeneous reticular intensities that were of low signal intensity on T1-weighted spin echo images and of high signal intensity on T2-weighted gradient echo and fat-saturated images, representing edema or inflammation, were present in the soft tissues surrounding the cyst. After intravenous contrast administration the surrounding soft tissues showed enhancement, whereas the internal cysts and matrix did not enhance. The MR imaging characteristics of the lesion were regarded as diagnostic for a hydatid cyst.

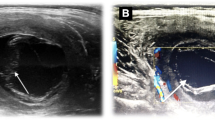
MR images of hydatid cyst within sartorius muscle containing daughter cysts. A T1-weighted spin echo axial image demonstrates multiple daughter cysts showing lower signal intensity than the mother cyst. B On the T2-weighted gradient echo axial image, the daughter cysts are hypointense compared with the mother cyst. There is a layer of high signal intensity (white arrow) around the hypointense component of the rim (black arrow)

MR images of the thigh demonstrating the water-lily sign. A Coronal T2-weighted fat-saturated image of the posterior distal portion of the left thigh and B axial T2-weighted gradient echo image show the hypointense collapsed cyst membrane (arrows) at the most dependent part of the mother cyst, producing the water-lily sign. Note the peripheral non-homogeneous high-intensity soft tissue, representing edematous or inflammatory infiltration. C, D Sagittal T1-weighted spin echo images of the medial aspect of distal left thigh, before (C) and after (D) gadolinium-DTPA enhancement. On the pre-contrast image, inhomogeneous reticular intensities that are low in signal are seen around the mother cyst (arrowheads). After injection of gadolinium-DTPA, the surrounding edematous or inflammatory infiltration shows enhancement (arrowheads), while the collapsed cyst membrane and the mother and daughter cysts do not enhance
Abdominal ultrasonography and radiographs of the chest showed no evidence of hepatic or pulmonary involvement, and the diagnosis of a primary muscular hydatid disease was made. At operation, complete surgical resection of the cystic mass was performed. The patient tolerated surgery well and postoperative recovery was uneventful. Histopathologic examination of the specimen confirmed the existence of mother and daughter cysts of hydatid disease. Postoperatively, the patient was discharged in good general condition.
Discussion
In hydatid disease, muscles, apart from myocardium, are generally only involved as a result of spread from hepatic or pulmonary foci [2]. Primary hydatidosis of skeletal muscle is therefore rare, with reported prevalences of 0.5–4.7% [10]. Muscles are an unfavorable site for this infestation because of their contractility and high lactic acid levels [1, 3, 10].
Primary intramuscular hydatidosis, involving exclusively the sartorius muscle, has been reported previously and our case is the third in the English-language literature [11, 12]. In an endemic region, where there is familiarity with this condition, the occurrence of hydatid disease in common sites makes for a straightforward diagnosis, but when it occurs in unusual sites (and in uncommon regions), the diagnosis may be difficult not only due to a low prevalence and unusual location, but also because complicated cysts may resemble solid or complex lesions such as soft tissue tumors [3, 5, 10]. On the other hand, the preoperative diagnosis or suspicion of this disease is of paramount importance to avoid percutaneous needle or open biopsy and improper handling during surgery, as these procedures can lead to inadvertent cyst rupture with the consequent risks of anaphylaxis and dissemination to other organs [3, 13]. Our patient had undergone several needle aspirations prior to a radiologic examination, but fortunately none of the above-mentioned complications had occurred.
The diagnosis was straightforward in our patient because of the characteristic and pathognomonic imaging findings. MR imaging showed not only a cystic mass, typically containing multiple vesicles (cyst or cysts within a cyst) and surrounded by a rim of low- and high-signal intensity layers on T2-weighted images, but also a collapsed cyst membrane in the inferior portion of the cyst, suggestive of the water-lily sign. The presence of the rim and multicystic appearance are regarded as typical features of hydatid disease [7]. These internal cysts (daughter cysts) have low signal intensity on T1-weighted images and low or high signal intensity on T2-weighted images, when compared with the mother cyst [1]. In our case, the daughter cysts were hypointense in comparison with the mother cyst on all pulse sequences. The rim, which is composed of parasitic membranes (germinal or endocystic layer and ectocystic layer) and a vascularized membrane that is formed as a response of the host (pericyst) [1, 2, 7], was described as a characteristic sign for hydatidosis of the liver and lungs [1]. It was pointed out that the rim is usually of low signal intensity on non-contrast MR imaging [2]. However, the rim was seen to contain two layers in our case, similar to the two cases in Memis et al.'s report [7] and we considered (as did Memis et al.) that the hypointense inner layer of the rim on T2-weighted images represented fibrous tissue (this, however was not histologically correlated), while the outer hyperintense layer represented the pericyst [7]. The non-homogeneous reticular intensities surrounding the mother cyst, which were of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images and demonstrated contrast enhancement, were regarded as edema or inflammation caused by compression or allergic reaction of soft tissues surrounding the cyst. García-Díez et al. [1] stated that this finding is not common in soft tissue hydatidosis.
The water-lily sign was established as a pathognomonic sign in hepatic and pulmonary hydatid disease and was also described in cerebral and orbital hydatid cysts [9, 14]. This sign in an intramuscular hydatid cyst has not previously been reported. In our case, one of the needle aspirations was thought to have caused separation of one or both of the parasitic membranes from the pericyst and then complete collapse of the membrane at the inferiormost part of the cyst, resulting in a water-lily sign as in the case reported by Gomori et al. [14]. When compared with the daughter cysts, the collapsed membrane was hypointense relative to the matrix on all pulse sequences and slightly lower in signal intensity on T1-weighted images, but with low signal on T2-weighted images. It did not enhance after infusion of contrast medium and for this we do not have an explanation.
The possibility of hydatid disease, especially in endemic areas, should always be considered in the differential diagnosis of soft tissue masses and therefore such cases should initially be evaluated with a cross-sectional imaging technique in order not to increase the likelihood of recurrent or disseminated infection and anaphylactic shock with iatrogenic procedures, because the propensity for recurrence and dissemination mortality is about 70% [1, 2, 3, 15]. MR imaging is an accurate method for preoperative diagnosis and surgical planning [1, 3, 4, 7] and the pathognomonic water-lily sign may occur in muscular hydatid cysts that have previously been punctured.
References
Garcia-Diez AI, Ros Mendoza LH, Villacampa VM, Cozar M, Fuertes MI. MRI evaluation of soft tissue hydatid disease. Eur Radiol 2000; 10:462–466.
Guthrie JA, Lawton JO, Chalmers AG. Case report: The MR appearances of primary intramuscular hydatid disease. Clin Radiol 1996; 51:377–379.
Tatari H, Baran O, Sanlidag T, Gore O, Ak D, Manisali M, Havitcioglu H. Primary intramuscular hydatidosis of supraspinatus muscle. Arch Orthop Trauma Surg 2001; 121:93–94.
Bayram M, Sirikci A. Hydatic cyst located intermuscular area of the forearm: MR imaging findings. Eur J Radiol 2000; 36:130–132.
al-Sayed M, al-Mousa M, al-Salem AH. A hydatid cyst at an unusual site. Trop Geogr Med 1992; 44:275–277.
Salai M, Apter S, Dudkiewicz I, Chechik A, Itzchak Y. Magnetic resonance imaging of hydatid cyst in skeletal muscle. J Comput Assist Tomogr 1999; 23:331–332.
Memis A, Arkun R, Bilgen I, Ustun EE. Primary soft tissue hydatid disease: report of two cases with MRI characteristics. Eur Radiol 1999; 9:1101–1103.
Tarhan NC, Tuncay IC, Barutcu O, Demirors H, Agildere AM. Unusual presentation of an infected primary hydatid cyst of biceps femoris muscle. Skeletal Radiol 2002; 31:608–611.
Malde HM, Gadkari SS, Chadha D, Gondhalekar N. Water lily sign in an orbital hydatid cyst. J Clin Ultrasound 1993; 21:458–459.
Tacal T, Altinok D, Yildiz YT, Altinok G. Coexistence of intramuscular hydatid cyst and tapeworm. AJR Am J Roentgenol 2000; 174:575–576.
Rask MR, Lattig GJ. Primary intramuscular hydatidosis of the sartorius. Report of a case. J Bone Joint Surg Am 1970; 52:582–584.
Vietri F, Illuminati G, Palumbo P, Guglielmi R. Recurrent primary hydatidosis of sartorius muscle. Case report. Acta Chir Scand 1988; 154:535–536.
Dudkiewicz I, Salai M, Apter S. Hydatid cyst presenting as a soft-tissue thigh mass in a child. Arch Orthop Trauma Surg 1999; 119:474–475.
Gomori JM, Cohen D, Eyd A, Pomeranz S. Water lily sign in CT of cerebral hydatid disease: a case report. Neuroradiology 1988; 30:358.
Unal AE, Ulukent SC, Bayar S, Demirkan A, Akgul H. Primary hydatid cyst of the axillary region: report of a case. Surg Today 2001; 31:803–805.
Acknowledgement
The authors thank Dr. Orhan Macit Ariyurek for his help with this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Comert, R.B., Aydingoz, U., Ucaner, A. et al. Water-lily sign on MR imaging of primary intramuscular hydatidosis of sartorius muscle. Skeletal Radiol 32, 420–423 (2003). https://doi.org/10.1007/s00256-003-0661-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-003-0661-x