
Abstract
Background
Current protocols for functional MR urography (fMRU) require long scan times, limiting its widespread use.
Objective
Our goal was to use pre-defined criteria to reduce the number of sequences and thus the examination time without compromising the morphological and functional results.
Materials and methods
The standard fMRU protocol in our department consists of eight sequences, including a 17-min dynamic post-contrast scan. Ninety-nine children and young adults (43 male, 56 female, mean age 7 years) were evaluated with this protocol. Each sequence was retrospectively analyzed for its utility and factors that affect its duration.
Results
Mean scan time to perform the eight sequences, without including the variable time between sequences, was 40.5 min. Five sequences were categorized as essential: (1) sagittal T2 for planning the oblique coronal plane, (2) axial T2 with fat saturation for the assessment of corticomedullary differentiation and parenchymal thickness, (3) coronal 3-D T2 with fat saturation for multiplanar and 3-D reconstructions, (4) pre-contrast coronal T1 with fat saturation to ensure an appropriate scan prior to injecting the contrast material and (5) the coronal post-contrast dynamic series. Functional information was obtained after 8 min of dynamic imaging in the majority of children. The coronal fat-saturated T2, coronal T1, and post-contrast sagittal fat-saturated T1 sequences did not provide additional information. Because of the effects of pelvicalyceal dilation and ureteropelvic angle on the renal transit time, prone position is recommended, at least in children with high-grade pelvicalyceal dilation.
Conclusion
Comprehensive fMRU requires approximately 19 min for sequence acquisition. Allowing for time between sequences and motion correction, the total study time can be reduced to about 30 min. Four pre-contrast sequences and a shortened post-contrast dynamic scan, optimally with the child in prone position, are sufficient.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Functional MR urography (fMRU) has proved to be a valuable tool for the evaluation of complex urinary tract anomalies. Use of this imaging modality has demonstrated improved morphological and functional evaluation of the urinary tract compared to US, CT and excretory urography [1–3]. Functional information obtained with fMRU is similar to that of scintigraphy [4–7].
The widespread use of fMRU in children is impeded not by its diagnostic capability but by ancillary issues like high cost, need for sedation and long duration of examination. Sequence acquisition time, not including breaks and additional delayed imaging, is about 45 min for many recommended fMRU protocols [4, 8]. In children requiring sedation, longer scan times also mean longer and deeper sedation. The purpose of this study was to comprehensively evaluate the standard fMRU protocol used in our department, as well as in many other centers, to determine the necessity and utility of each sequence. The goal was to create an optimized fMRU protocol that is short but still provides comprehensive morphological and functional information.
Materials and methods
Patients
This retrospective study was approved by the institutional review board and was performed in compliance with the Health Insurance Portability and Accountability Act (HIPAA). We identified fMRU studies by searching the radiology database of our department for the period between July 2008 and December 2010.
The inclusion criteria were the presence of all of our eight standard sequences, comprising six pre-contrast (sagittal and axial T2, coronal T1 and T2, coronal 3-D T1 and T2) and two post-contrast sequences (coronal and sagittal T1). A total of 99 fMRU studies met the inclusion criteria. The group consists of 43 males and 56 females with a mean age of 7.0 years (range 1.1 months–19.2 years). One subject had a single kidney. Complete duplication was present unilaterally in 17 and bilaterally in four subjects. Thus the 99 subjects had a total of 222 pelviureteral units. The indications for the fMRU studies were as follows: pelvicalyceal dilation without ureterectasis (n = 57), pelvicalyceal dilation with ureterectasis (n = 20), complicated duplex collecting system (n = 14) and ectopic ureter (n = 8).
Functional MR urography procedure and scan
Preparation for fMRU
Sedation is used for all children younger than 7 years. All children received intravenous hydration prior to imaging. In all patients bladder catheterization was performed using a Foley catheter without inflating the balloon. Initially all patients were positioned in a supine position. The catheter was connected to a urine bag and this was placed below the level of the MR table to facilitate bladder emptying. Fifteen minutes prior to the contrast agent injection, 1 mg/kg of furosemide, with a maximum dose of 20 mg, was administered intravenously [4].
Functional magnetic resonance urography
The scans were performed using a 1.5-T Avanto® platform (Siemens Healthcare, Erlangen, Germany). Either a 6- or a 9-channel body matrix coil was used in combination with a 24-channel spine coil for the acquisition of images. Table 1 includes sequence duration as documented in the scanner. The total duration was 40 min 29 s, not including additional time required for motion correction or breaks between sequences. For post-contrast imaging, gadolinium-DTPA (Magnevist®; Bayer-Schering, Berlin, Germany) was administered at a dose of 0.2 ml/kg (0.1 mmol/kg) with a minimum dose of 2 ml and a maximum dose of 20 ml at a slow rate adjusted for age. The dynamic post-contrast scan included 55 coronal 3-D fat-saturated T1-W gradient recalled echo (GRE) volumetric interpolated breath hold examination (VIBE) series that were acquired with increasing 2- to 42-s pauses between acquisitions.
Additionally, when contrast washout was not visualized in one or more ureters during the dynamic scan, we obtained additional delayed post-contrast 3-D fat-saturated T1-W GRE VIBE with the patient in (1) supine position, (2) supine and prone positions or (3) just prone position.
Functional MRU post-processing
Multiplanar reconstructions and 3-D volumetric reformats were performed from the coronal fat-saturated 3-D T2-W and coronal post-contrast dynamic sequences. For the functional analysis we used a custom-made freeware (chop-fmru, available at www.chop-fmru.com) [4]. Calyceal transit time (CTT) and renal transit time (RTT) were recorded for each pelviureteral unit. CTT is defined as the time it takes for the contrast material to get from the aorta into the calyces. RTT is defined as the time it takes for the contrast material to appear in the ureter, at a level below the lower pole of the kidney, from the time it was detected in the aorta [4].
Evaluation of duration of fMRU scan steps
The following times (hours:minutes:seconds) of the fMRU examinations were recorded from the time stamp on the images: first image of supine localizer, first image of the first coronal post-contrast dynamic sequence, last image of the last coronal post-contrast dynamic sequence without contrast enhancement of the aorta, and first image of the sagittal high-resolution fat-saturated 3-D T1-W sequence. In patients in whom delayed supine imaging was carried out, the time of the last image of the last delayed post-contrast fat-saturated 3-D T1-W sequence was recorded. In those with delayed prone imaging three additional times were recorded: last image time before changing the patient’s position to prone, first localizer image time in prone position, and last image time of the prone delayed post-contrast 3-D T1-W sequence. In patients in whom delayed supine and delayed prone images were acquired, all the former times were recorded.
The following time intervals were defined:
-
(1)
Standard protocol duration: from the first supine localizer to the last sagittal high-resolution fat-saturated T1-W image.
-
(2)
Delayed supine protocol duration: from the first supine localizer to the last delayed post-contrast 3-D T1-W GRE image.
-
(3)
Delayed prone with and without delayed supine protocol duration: from the first supine localizer to the last delayed post-contrast 3-D T1-W GRE image in prone.
-
(4)
Aortic contrast time: time taken for the contrast agent to appear in the aorta after the start of the coronal post-contrast dynamic series, i.e. duration from first coronal post-contrast dynamic image to the last coronal post-contrast dynamic image before contrast agent is detected in the aorta.
-
(5)
The time required to change the position from supine to prone position, i.e. from the last post-contrast T1-W GRE series to the first prone localizer image.
Evaluation of the utility of each sequence
The utility of each pre-contrast and post-contrast sequence was evaluated based on the following preset subjective and objective criteria and then classified as essential or non-essential.
Pre-contrast sequences
Localizer and sagittal T2: Which of the two sequences is best for planning the coronal planes? The sagittal T2 is used for planning the oblique coronal plane that goes through the renal hila, parallel to the ureters and aorta, and through the mid-portion of the bladder. We evaluated whether the localizer scan would suffice for optimal placement of the oblique coronal plane or not. It was considered adequate if both kidneys, the bladder and the aorta were depicted on the sagittal component of the localizer sequence. If one or more of these was not visualized it was labeled as inadequate.
Axial high-spatial-resolution fat-saturated T2: Are parenchymal changes frequent enough to warrant the performance of this sequence? It was reviewed for normal or decreased corticomedullary differentiation. In addition, a four-point ordinal scale was used to evaluate parenchymal thinning: grade 0 = none, grade I = focal, grade II = multifocal and grade III = diffuse.
Coronal T1: Does this sequence provide additional useful information? Images were reviewed for the presence of additional diagnostic information not provided by other sequences.
Coronal fat-saturated T2: Does this sequence have extra value? It was reviewed for the presence of additional diagnostic information not provided by the axial high-spatial-resolution fat-saturated T2 and the coronal fat-saturated 3-D T2 sequences.
Coronal fat-saturated 3-D T2: This is an obligatory sequence for multiplanar and 3-D reconstructions, thus it was not included in further evaluation.
Coronal pre-contrast fat-saturated T1 GRE: How often does this sequence help to avoid a sub-optimal post-contrast dynamic series? In the standard fMRU protocol a single coronal pre-contrast fat-saturated T1-W GRE sequence is performed. This sequence is used to help avert the acquisition of coronal post-contrast dynamic series without an appropriate field-of-view or degraded by motion. We evaluated the frequency and reason of the repetition of this sequence.
Post-contrast sequences
Coronal post-contrast dynamic: Can we set the duration of the dynamic series more objectively? This is an obligatory sequence for functional and additional morphological information. Thus this was not included in further evaluation regarding its importance. However, the duration of the dynamic scan, which was set at 15 min, was indirectly evaluated through the assessment of the transit times. To find an objective time span for the dynamic series, we documented the highest CTT or RTT of each patient in whom all CTT or RTT were available and calculated the 50th–90th percentiles in steps of ten.
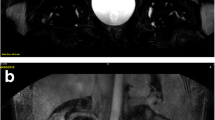
Sagittal high-resolution fat-saturated T1: Do we need this sequence to determine the need to perform delayed scans or change the position to prone? We evaluated the presence of contrast layering, which prompts the performance of delayed imaging or change in position of the patient to prone. Fluid-fluid level was present if a layer of low signal intensity, urine, was detected above a layer of high signal intensity, contrast agent or contrast agent plus urine. We also evaluated contrast layering on the last coronal post-contrast dynamic sequence (directly preceding the sagittal high-resolution fat-saturated T1). We compared the rate of contrast layering visualization between the two sequences using as reference standard the sagittal plane because the layering was easier to depict (Fig. 1).

Contrast layering in a 2-year-old boy with ureteropelvic junction obstruction is demonstrated on single sample images from the (a) sagittal high-resolution fat-saturated T1-W and (b) coronal post-contrast dynamic MR sequences
Evaluation of other variables related to patient positioning
Pelvicalyceal dilation
We qualitatively assessed the grading of pelvicalyceal dilation using an adapted version of the Society of Fetal Urology (SFU) classification by Riccabona et al. [9, 10]. This grading encompasses six grades from 0 (no pelvicalyceal dilation) to five (marked pelvicalyceal dilation with loss of the normal configuration) (Fig. 2). Grades 3 and higher were defined as high-grade pelvicalyceal dilation.

Grading of pelvicalyceal dilation adapted from Riccabona et al. [10] demonstrated with pre-contrast coronal fat-saturated T2-weighted images. The degree of dilation is graded as: (a) grade 0 (3-year-old girl), (b) grade 1 (3-year-old girl), (c) grade 2 (4-year-old girl), (d) grade 3 (7-month-old boy), (e) grade 4 (10-month-old boy) and (f) grade 5 (1-year-old girl)
Ureteropelvic junction angle
With the patient in supine position the contrast agent settles in the dependent part of the dilated renal pelvis. It takes time for the contrast agent to reach the ureteropelvic junction. The more anterior the junction, the longer it takes for the contrast agent to appear in the proximal ureter. This is an angle measurement modified for fMRU from the one used for percutaneous endopyelotomy [11]. It was measured on the axial high-spatial resolution fat-saturated T2-W sequence in non-duplicated kidneys (n = 171). The optimal axial slice demonstrating the renal hilum/ureteropelvic junction was selected, a horizontal line parallel to the MR table was drawn just above the spinal canal followed by a second line from the ureteropelvic junction to the center of the kidney. The angle between the above crossing lines, the ureteropelvic junction angle, was measured. It was defined as positive if the ureteropelvic junction was anterior to the horizontal line and negative if below the line (Fig. 3).

Ureteropelvic junction angle. Axial high-spatial resolution fat-saturated T2-weighted images demonstrate (a) positive and (b) negative ureteropelvic junction angles in a 2-year-old boy and a 14-year-old girl, respectively
Change in patient position
We evaluated whether there was ureteric contrast agent in the prone delayed post-contrast 3-D T1-W images that was not previously detected in the last dynamic sequence in the supine position. The results were either presence or absence of ureteric contrast agent on change in position.
Statistical analysis
We used descriptive statistics to describe the distribution of subjects, absence of corticomedullary differentiation, degree of parenchymal thinning, additional information provided by the coronal T1 sequence and the effect of changing the patient’s position to prone. We used the Shapiro–Wilk test to assess the distribution of data. A Mann–Whitney U test was used to find differences in the CTT and RTT related to the presence of contrast layering of each pelviureteral unit. Spearman rho tests were used to find correlations among CTT, RTT and the degree of pelvicalyceal dilation. We used linear regression to search for a relationship between CTT or RTT and the ureteropelvic junction angle. The chi-square test was performed to evaluate the relationship of fluid-fluid level with the grade of pelvicalyceal dilation. The significance level for differences was accepted at P < 0.05. Statistical analyses were performed using SPSS software (version 20; IBM Corp., Armonk, NY).
Results
Duration of fMRU scan steps
The mean duration of the different protocols is summarized in Table 2 and Fig. 4. This time reflects the sequence duration, time required for motion correction, repetition of sequences and possible breaks between sequences. Only 33.3% of the patients had a standard protocol without additional delayed imaging. The remaining 66.7% had additional post-contrast delayed imaging in supine, in prone or in both positions. The mean aortic contrast time was 1 min 35 s (±36 s). For patients who underwent prone imaging the mean time needed to change the position of the patient from supine to prone was 11 min 1 s (±3 min 8 s).

Schematic presentation of the mean time to perform the standard functional MR urography (fMRU) protocol with different procedural steps. Percentages in parentheses denote the portion of examinations out of the total 99 studies performed with the respective protocol. Sag sagittal
Evaluation of utility of each sequence
Essential sequences
The following sequences were found to be essential based on the preset subjective or objective criteria and were thus necessary to incorporate into an updated fMRU scan protocol.
-
(1)
Sagittal T2: Using the localizer, both kidneys were visualized in 50 patients (50.5%) in coronal plane, 43 patients (43.4%) in axial plane and five patients (5.1%) in sagittal plane. Therefore, the localizer as set in the scan protocol is inadequate, making the sagittal T2 sequence, which goes through the whole trunk, essential for appropriate planning of the oblique coronal planes.
-
(2)
Axial high-spatial-resolution fat-saturated T2: Corticomedullary differentiation and parenchymal thinning are best appreciated on this high-resolution sequence. These two parameters are necessary for correlation with the renal functional results [8]. We found decreased corticomedullary differentiation in 33/99 (33.3%) patients (46/222 pelviureteral units, or 20.7%). Parenchymal thinning was present in one or both kidneys in 54/99 (54.5%) patients (74/222, pelviureteral units, or 33.3%). The distribution of the degree of parenchymal thinning per pelviureteral units was as follows: 17 (7.6%) focal, 7 (3.2%) multifocal and 50 (22.5%) diffuse. The detection of a high number of pathological findings justifies the use of this scan, which is also the only one in the axial plane in the fMRU scan protocol.
-
(3)
Coronal pre-contrast fat-saturated T1 GRE: In 16/99 (16.2%) studies it was necessary to repeat this sequence. The reasons for repeating the sequence were patient motion (n = 7), incomplete field of view (n = 6) and no retrospectively apparent reasons (n = 3). If single coronal pre-contrast fat-saturated T1-W GRE scans had not been done, the subsequent coronal post-contrast dynamic scans may have turned out to be inadequate in at least 13/99 (13.1%) studies, making functional analysis and post-processing difficult or impossible. Performing this short sequence definitely averted such problems in a substantial number of studies.
-
(4)
Coronal post-contrast dynamic: This sequence is mandatory for comprehensive functional evaluation. Because of markedly reduced renal function and delayed washout into the ureters we were able to determine the CTT in 213/222 (95.9%) pelviureteral units and the RTT in 188/222 (84.7%) pelviureteral units. Ninety (90.9%) patients had CTT values in all pelviureteral units and 64/99 (64.6%) patients had RTT values in all pelviureteral units. The means and percentiles of the longest CTT and RTT per patient are summarized in Table 3. In half of the studies the longest CTT and RTT were 2.5 and 3.7 min, respectively. In 80% of the patients, the contrast agent reached the calyces in 3 min and the proximal ureter in about 6 min. The 80th percentile is just above the means for the longest CTT and RTT per patient. For the functional analysis, only the time period equivalent to the CTT is required. Our standard dynamic series lasted almost 17 min but the 80th percentile for the RTT is about 6 min. This means that in most patients the duration of the dynamic series could have been cut. To the 6.3-min RTT it is necessary to add the 80th percentile of the aortic contrast time, which was 1.8 min. Thus until the contrast agent reaches the proximal ureter the longest duration in 80% of the cases is the sum of the two time points, 6.3 min plus 1.8 min, i.e. 8.1 min. Thus we now have objective evidence for selection of the most appropriate duration for the dynamic post-contrast series.
Table 3 Patients in whom the calyceal transit times (CTTs) and renal transit times (RTTs) were possible to determine, with the means of the longest CTTs and RTTs and the 50th–90th time percentiles in minutes (min)
Non-essential sequences
The following sequences were not found to be essential according to the preset subjective or objective criteria and thus could be omitted in an updated fMRU scan protocol.
-
(1)
Coronal T1: In one patient, this sequence helped in the characterization of a Tarlov cyst. In the other 98 patients this sequence did not provide additional diagnostic information.
-
(2)
Coronal fat-saturated T2: This sequence did not provide additional diagnostic information in comparison with the axial high-spatial resolution fat-saturated T2 and coronal fat-saturated 3-D T2 sequences.
-
(3)
Sagittal high-resolution fat-saturated T1: We found contrast layering in 49/222 (22.1%) pelviureteral units on the sagittal high-resolution fat-saturated T1 sequence and in 41/222 (18.5%) pelviureteral units on the last series of the coronal post-contrast dynamic sequence. The sensitivity and specificity of the last coronal post-contrast dynamic series in comparison with the sagittal high-resolution fat-saturated T1 sequence for determining contrast layering were 97.6% (confidence interval [CI] 95%: 85.6–99.9) and 95% (CI 95%: 90.5–97.6), respectively. Consequently, for the purpose of detection of the contrast layering, the coronal post-contrast dynamic images suffice and the sagittal sequence was deemed unnecessary.
Other variables related to patient positioning
Grading of pelvicalyceal dilation
The distribution of the grades of pelvicalyceal dilation in the 222 pelviureteral units, i.e. both sides to be evaluated, and where applicable the contralateral normal sides, were as follows: 26 (11.7%) grade 0, 77 (34.7%) grade 1, 48 (21.6%) grade 2, 18 (8.1%) grade 3, 36 (16.2%) grade 4 and 17 (7.7%) grade 5. A positive correlation between RTT and the grade of pelvicalyceal dilatation was found (Spearman rho test P < 0.001, r = 0.495). Using the same test no significant correlation with the CTT was found (P = 0.27) (Fig. 5). Thus the mere increase in RTT does not necessarily mean an obstruction. With the patient in supine position this may just be the consequence of high-grade pelvicalyceal dilation. With the patient in supine position the correct interpretation of the RTT result needs to take into account the existing degree of pelvicalyceal dilation.

Grades of pelvicalyceal dilation (0 = none to 5 = marked dilation with loss of contour) in relation to (a) the median renal transit times (RTT) and (b) median calyceal transit times (CTT) in minutes
Ureteropelvic junction angle
The mean ureteropelvic junction angle for the 171 kidneys without duplicated renal collecting systems was 28.3° (range −17° to 80°). A positive angle was seen in 167 kidneys (97.7%), a negative angle in 4 (2.3%) kidneys. We found a positive correlation between ureteropelvic junction angle and RTT (linear regression: r = 0.3, P < 0.001). No significant correlation was found between ureteropelvic junction angle and CTT (P = 0.53). With the patient in supine position, the more anterior the junction between the renal pelvis and ureter the longer it takes for the contrast agent to wash out. Consequently, similar to the grade of pelvicalyceal dilation, ureteropelvic junction angle needs to be taken into consideration for the appropriate interpretation of the RTT result. With the patient in supine position the combination of high-grade pelvicalyceal dilation and high-positive ureteropelvic junction angle resulted in a longer RTT.
Assessment of contrast layering in the renal collecting system
We found contrast layering in 49/222 (22.1%) pelviureteral units. The median CTT and RTT for pelviureteral units with contrast layering were 2.5 and 5.3 min, respectively. Contrast layering was absent in 173/222 (77.9%) pelviureteral units, with a median CTT and RTT of 2.3 and 2.8 min, respectively. Using Mann–Whitney U test we found a significant difference in the RTT between patients with and without contrast layering (P < 0.001). No definite significance was found in the CTT between patients with and without contrast layering (P = 0.053). There was a significant correlation between the presence of contrast layering and the grade of pelvicalyceal dilation (chi-square test: X 2 = 117.1, P < 0.001). The pelviureteral junction angle was significantly higher in patients with contrast layering compared to patients without contrast layering (Mann–Whitney U test P < 0.001).
Change in patient position
Scans were performed in supine position followed by prone position in 27 patients (59 pelviureteral units). In this population, contrast agent was seen in the proximal ureter in 39/59 pelviureteral units (66.1%) during supine imaging. The distribution of the grades of pelvicalyceal dilation in the 20 pelviureteral units without ureteric contrast agent was as follows: three grade 0, one grade 1, three grade 2, two grade 3, seven grade 4 and four grade 5. The mean ureteropelvic junction angle in the 20 pelviureteral units without ureteric contrast agent was 34.3°. Eleven of the 20 pelviureteral units had high-grade pelvicalyceal dilation and exhibited contrast layering. In prone position contrast agent immediately appeared in the proximal ureter in 13/20 (65%) pelviureteral units. Out of these 13 pelviureteral units, high-grade pelvicalyceal dilation was present in 9/13 (69.2%). Thus scanning in prone was helpful in facilitating the contrast washout in a significant number of pelviureteral units in which contrast agent was not present in supine imaging. This is of greater importance in children with high-grade pelvicalyceal dilation.
Shorter and optimized fMRU protocol
Given these findings, the number of the fMRU sequences can be reduced to incorporate basically three pre-contrast scans, one pre-contrast test scan prior to contrast administration and one post-contrast dynamic series comprised of 39 repetitions shortened to 8 min (Table 4). Thus the total scan time without including the breaks between sequences can be reduced from 40 min 29 s to 18 min 58 s, i.e. a 53% reduction. With the dynamic series set at 8 min in 20% or fewer patients, additional single or multiple delayed fat-saturated T1 GRE sequences may be needed, at least with the patient in supine position. The mean time each patient spent on the MR table using our former protocol was 1:04 h with about 37% of the total scan time devoted to time between sequences and other technical factors. Accordingly, if we increase the duration of the optimized fMRU scan time of 19 min by a similar measure, the duration of the fMRU examination in most patients should be about 30 min. The short protocol can only be maintained by avoiding delay in contrast washout caused by patient positioning. This is best achieved by conducting the fMRU in prone position, particularly in children with high-grade pelvicalyceal dilation or high positive ureteropelvic angle.
Discussion
The purpose of this study was to optimize and shorten the fMRU protocol without affecting its diagnostic information. After analyzing each sequence according to its diagnostic value, we put together a shorter optimized protocol with a significant reduction of the total scan time. The optimized fMRU protocol should be carried out in prone position. In this way it is possible to eliminate the negative effects on the RTT of high-grade pelvicalyceal dilation and high positive pelviureteral junction angle. The gadolinium contrast agent settles in the dependent part of the pelvicalyces because it has higher specific gravity than urine. In the supine position the dependent part is usually farthest from the ureteropelvic junction. These factors contribute to a delay in appearance of contrast agent in the ureter. Performing the fMRU in prone position can not only avert the need for delayed scans but also prevent the need to later flip the patient from supine to prone position. We do get contrast layering in the prone position; however in this position the pelviureteral unit located anteriorly in 98% of the patients becomes the dependent part and thus the washout of the contrast agent is facilitated. For this reason, the contrast layering does not affect the RTT.
We found a positive correlation between RTT and grade of pelvicalyceal dilation as well as degree of ureteropelvic junction angle. This poses difficulty in interpreting the RTT results using our standard protocol in supine position. Similarly, the use of reported cut-offs for the RTT, generated with the study in supine position, in categorizing a dilated pelvicalyceal system as obstructed and non-obstructed poses challenges [11]. It has been described that the insertion of the ureter in the renal pelvis has an influence on the drainage, so the interpretation of the RTT should take this into consideration [7, 12]. Using the ureteropelvic junction angle, a more objective assessment of this relationship could be achieved. The RTT may also be affected by the position of the patient, particularly in the presence of pelvicalyceal dilation [13, 14]. Consequently, we cannot compare the values of RTTs generated in supine position to those obtained when starting the fMRU in prone position. We require new cut-offs for the RTTs for appropriate interpretation. In comparison, the CTT is not affected by the grade of pelvicalyceal dilation, the degree of ureteropelvic junction angle or the position of the patient. The absence of effect of pelvicalyceal dilation on CTT may be explained by the protective effect that compliant pelvicalyceal systems have on the nephron by reducing the pressure transmitted upward [15, 16]. Because the CTT only includes the washout of contrast agent through the renal parenchyma, this measurement is not affected by the presence of contrast layering in the pelvicalyceal system.
We have objectively demonstrated the variables that lead to a delay in contrast washout during an fMRU. We found that changing position from supine to prone helped to facilitate contrast washout in 65% of the pelviureteral units in which no contrast agent was seen in the ureter in supine imaging. In addition, it is important to realize that the repositioning from supine to prone took on average 11 min. Conduction of the fMRU in prone position appears to be the simplest way to counteract the contrast washout delaying variables. There are a number of factors to consider prior to making the decision to carry out the study with the patient prone. First, the positioning plays a role only for the post-contrast dynamic series. In the case where just a pre-contrast imaging is performed for morphological evaluation and without intravenous contrast administration, prone positioning is not necessary. Second, it also depends what technique is used for the fMRU. If the functional analysis does not incorporate a segmentation of contrasted pelvicalyces with an excretion curve, or the functional interpretation is primarily based on the CTT and other functional results and the RTT does not play an important role, a supine positioning may suffice. Third, the indication for the fMRU should also be a deciding factor in how to position the patient. Prone positioning is primarily important if there is the question of ureteropelvic junction obstruction. This may be for initial evaluation or as a follow-up for post-pyeloplasty. Other indications such as the assessment of pyelonephritis or renal scarring or renal tumor do not require prone positioning [17].
There may be concerns about the management of the airway for sedation or anesthesia in the prone position. A prone position mechanical ventilation has been used for prolonged times in pediatric patients with acute lung injury without significant differences in the rate of endotracheal tube leak, times of extubation, and episodes of transient desaturations [18, 19]. No significant hemodynamic changes have been reported [18, 19]. At our institution sedation or anesthesia is provided by a dedicated team. Each patient is evaluated prior to the procedure, taking into account the patient’s age, clinical history and examination indication, before decisions are made as to whether to use sedation or anesthesia and whether an endotracheal intubation or the use of a laryngeal mask is needed. In patients undergoing moderate-to-deep sedation with spontaneous breathing it is sometimes difficult to have appropriate ventilation. Thus in these patients changing back to supine position may be necessary. Two years after the implementation of the fMRU in prone position in our institution, it appears to be well tolerated by our patients and our anecdotal experience is that there is no increase in the complication rates related to sedation/anesthesia; nevertheless, future studies need to look into this change in further detail.
In some patients additional sequences or modification of the optimized fMRU protocol may be required. In patients with ectopic ureter or genital abnormalities a pre-contrast axial high-resolution fat-saturated T2-W sequence of the pelvis may provide important additional information. If the bladder is completely empty and a possible ectopic insertion is difficult to evaluate, clamping the bladder catheter until the start of the post-contrast series may help to distend the bladder and better localize the ureteral insertion. When a calyceal diverticulum is suspected, long delayed post-contrast scans may be necessary if contrast is not noted earlier in the cystic space [20]. In children after pyeloplasty, it might be necessary in fMRU studies to wait longer in order to compare the contrast washout in the proximal ureter or the RTT to that before surgery.
To set the dynamic scan duration we took the 80th percentile of the longest CTT and RTT per patient because these were just at the means for both values at this percentile. There is room for variation. If the radiologist is at the scanner it is easy to actively follow the dynamic scan and stop when adequate contrast is reached. Probably this would provide an individualized and highly tailored approach and lead to significant shortening of the dynamic series. In the settings where the radiologist cannot monitor the study at the scanner, protocols have to be in place with a set time for dynamic scans. As our results indicate, if we use the 50th percentile a 5-min dynamic series may suffice. If the fMRU is primarily based on the CTT it is even possible to further shorten the scan. Indications for such a short protocol may include patients coming for evaluation for pyelonephritis or renal scarring or renal tumors [17].
The study does have a number of limitations. The standard fMRU protocol from which we started as a baseline is one that is used with minor modifications by many but not necessarily all institutions. Thus the extent of the reduction in the fMRU scan duration may not apply equally to all users. Furthermore, our sequences are tailored to one specific scanner. We acknowledge the variation of the type of sequences and scan durations among scanners of different manufacturers. The evaluation of the utility of the specific sequences was based on practical criteria, but there is some subjectivity to this selection. The group that went on to have additional scans in prone position is a smaller group in comparison to the larger study cohort. Though we have clear evidence of fast and improved contrast washout in the prone position, this was not evaluated in all our patients. Nevertheless, we were able to conduct a relatively objective evaluation of our standard fMRU protocol and demonstrate that we can perform optimized, focused and shorter fMRU studies and still obtain comprehensive morphological and functional information.
The reduction by almost half of the fMRU duration has positive implications with regard to MR scanner access and sedation reduction. We anticipate further improvements in scan time and contrast washout in most children by performing fMRU studies primarily in prone position for those with high-grade pelvicalyceal dilation or high positive degree of the pelvicureteric angle. We expect that a shorter, more efficient fMRU examination will facilitate more widespread use of fMRU in pediatric uroradiologic evaluations.
References
Grattan-Smith JD, Jones RA (2006) MR urography in children. Pediatr Radiol 36:1119–1132, quiz 1228–1229
Ehammer T, Riccabona M, Maier E (2011) High resolution MR for evaluation of lower urogenital tract malformations in infants and children: feasibility and preliminary experiences. Eur J Radiol 78:388–393
Darge K, Anupindi SA, Jaramillo D (2011) MR imaging of the abdomen and pelvis in infants, children, and adolescents. Radiology 261:12–29
Khrichenko D, Darge K (2010) Functional analysis in MR urography—made simple. Pediatr Radiol 40:182–199
Rohrschneider WK, Haufe S, Wiesel M et al (2002) Functional and morphologic evaluation of congenital urinary tract dilatation by using combined static-dynamic MR urography: findings in kidneys with a single collecting system. Radiology 224:683–694
McDaniel BB, Jones RA, Scherz H et al (2005) Dynamic contrast-enhanced MR urography in the evaluation of pediatric hydronephrosis: part 2, anatomic and functional assessment of uteropelvic junction obstruction. AJR Am J Roentgenol 185:1608–1614
Perez-Brayfield MR, Kirsch AJ, Jones RA et al (2003) A prospective study comparing ultrasound, nuclear scintigraphy and dynamic contrast enhanced magnetic resonance imaging in the evaluation of hydronephrosis. J Urol 170:1330–1334
Grattan-Smith JD, Little SB, Jones RA (2008) MR urography in children: how we do it. Pediatr Radiol 38:S3–17
Fernbach SK, Maizels M, Conway JJ (1993) Ultrasound grading of hydronephrosis: introduction to the system used by the society for fetal urology. Pediatr Radiol 23:478–480
Riccabona M, Avni FE, Blickman JG et al (2008) Imaging recommendations in paediatric uroradiology: minutes of the ESPR workgroup session on urinary tract infection, fetal hydronephrosis, urinary tract ultrasonography and voiding cystourethrography, Barcelona, Spain, June 2007. Pediatr Radiol 38:138–145
Smith ADMD (2012) Smith’s textbook of endourology. Wiley-Blackwell, Chichester
Grattan-Smith JD, Little SB, Jones RA (2008) MR urography evaluation of obstructive uropathy. Pediatr Radiol 38:S49–69
Darge K, Higgins M, Hwang TJ et al (2013) Magnetic resonance and computed tomography in pediatric urology: an imaging overview for current and future daily practice. Radiol Clin North Am 51:583–598
Koff SA, Binkovitz L, Coley B et al (2005) Renal pelvis volume during diuresis in children with hydronephrosis: implications for diagnosing obstruction with diuretic renography. J Urol 174:303–307
Piepsz A (2007) Antenatally detected hydronephrosis. Sem Nucl Med 37:249–260
Koff SA (2003) The beneficial and protective effects of hydronephrosis. APMIS 2003:7–12
Cerwinka WH, Grattan-Smith JD, Jones RA et al (2014) Comparison of magnetic resonance urography to dimercaptosuccinic acid scan for the identification of renal parenchyma defects in children with vesicoureteral reflux. J Pediatr Urol 10:344–351
Fineman LD, LaBrecque MA, Shih MC et al (2006) Prone positioning can be safely performed in critically ill infants and children. Pediatr Crit Care Med 7:413–422
Kornecki A, Frndova H, Coates AL et al (2001) 4A randomized trial of prolonged prone positioning in children with acute respiratory failure. Chest 119:211–218
Mullett R, Belfield JC, Vinjamuri S (2012) Calyceal diverticulum—a mimic of different pathologies on multiple imaging modalities. J Radiol Case Rep 6:10–17
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Delgado, J., Bedoya, M.A., Adeb, M. et al. Optimizing functional MR urography: prime time for a 30-minutes-or-less fMRU. Pediatr Radiol 45, 1333–1343 (2015). https://doi.org/10.1007/s00247-015-3324-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-015-3324-x