
Abstract
Background
The use of ultrasound to diagnose appendicitis in children is well-documented but not universally employed outside of pediatric academic centers, especially in the United States. Various obstacles make it difficult for institutions and radiologists to abandon a successful and accurate CT-based imaging protocol in favor of a US-based protocol.
Objective
To describe how we overcame barriers to implementing a US-based appendicitis protocol among a large group of nonacademic private-practice pediatric radiologists while maintaining diagnostic accuracy and decreasing medical costs.
Materials and methods
A multidisciplinary team of physicians (pediatric surgery, pediatric emergency medicine and pediatric radiology) approved an imaging protocol using US as the primary modality to evaluate suspected appendicitis with CT for equivocal cases. The protocol addressed potential bias against US and accommodated for institutional limitations of radiologist and sonographer experience and availability. Radiologists coded US reports according to the probability of appendicitis. Radiology reports were compared with clinical outcomes to assess diagnostic accuracy. During the study period, physicians from each group were apprised of the interim US protocol accuracy results. Problematic cases were discussed openly.
Results
A total of 512 children were enrolled and underwent US for evaluation of appendicitis over a 30-month period. Diagnostic accuracy was comparable to published results for combined US/CT protocols. Comparing the first 12 months to the last 12 months of the study period, the proportion of children achieving an unequivocal US result increased from 30% (51/169) to 53% (149/282) and the proportion of children undergoing surgery based solely on US findings increased from 55% (23/42) to 84% (92/109). Overall, 63% (325/512) of patients in the protocol did not require a CT. Total patient costs were reduced by $30,182 annually.
Conclusion
We overcame several barriers to implementing a US protocol. During the study period our ability to visualize the appendix with US increased and utilization of CT decreased. Our overall diagnostic accuracy with the US-based protocol was comparable to other published results and remained unchanged throughout the study.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ultrasound (US) is the primary imaging tool to diagnose suspected appendicitis outside the United States and at some pediatric medical centers within the United States [1]. However where CT is used to diagnose appendicitis, widespread access to CT and a proven record of accurate diagnosis are compelling reasons to perpetuate this practice [2]. In our region of the western United States, hospitals that treat both adults and children are twice as likely to use CT for diagnosing appendicitis as our facility, a dedicated children’s hospital (according to a survey of CPT [Current Procedural Terminology] codes and diagnosis codes for appendicitis at five regional hospitals within the same health care system as our hospital). Several pediatric centers in the United States have reported favorable results using US for diagnosing appendicitis [3–5], but none has described the process of moving from a CT-based protocol to a US-based protocol.
Two major advantages of US over CT are lower cost and avoidance of ionizing radiation. A direct link between childhood radiation exposure from diagnostic CT scans and an increased cancer risk has been explicitly demonstrated for leukemia and brain tumors [6]. Ultrasound’s major disadvantage is decreased diagnostic accuracy compared to CT, even when practiced optimally [7].
Overall CT use in the United States increased significantly between 1996 and 2010 [8], and CT use during pediatric emergency department visits in the United States increased fivefold from 1995 to 2008 [9]. CT-based imaging protocols for suspected appendicitis persist for reasons including a low level of confidence in the accuracy of a US report, the assumption that using US is equivocal to delaying the diagnosis, and concern about increased costs for patients who require both US and CT. Radiologists and sonographers may be concerned about their level of proficiency or they may perceive 24-h coverage of a US practice as undesirable or impossible.
Our institution is an urban, privately owned, free-standing children’s hospital in the United States with mostly university-employed pediatric academic physicians on staff. The surgeons and emergency medicine physicians are fellowship-trained in pediatrics and practice exclusively in a pediatric setting. The pediatric radiology group is nonacademic and private practice. At our institution we encountered each of the obstacles described above. This paper describes our implementation, during a 30-month study period, of a successful and accurate US-based protocol for diagnosing appendicitis.
Materials and methods
We obtained IRB approval to review a new imaging protocol for appendicitis.
Protocol design and implementation
A protocol incorporating US as a first-line modality and CT as a secondary modality, as described at other institutions [5], was proposed by pediatric radiologists. Physicians from pediatric surgery and pediatric emergency medicine were invited to participate in designing the protocol, and two physician representatives from each department attended meetings to discuss how the protocol would be modified for our institution. We discussed potential obstacles such as diagnostic mistakes, increased time required to achieve an imaging diagnosis, increased patient cost for two imaging studies rather than one, radiologist and sonographer inexperience, and lack of overnight staffing.
Surgeons and emergency medicine physicians agreed that each child suspected of having appendicitis would be examined by an attending-level physician prior to imaging. All providers agreed the US protocol would be initially offered only during daytime hours when pediatric sonographers were available in-house. The written protocol was distributed to all physicians from radiology, pediatric surgery and pediatric emergency medicine and to the pediatric sonographers for their approval prior to implementation.
The radiologists and sonographers, recognizing their inexperience with this diagnostic technique, held several didactic lectures and hands-on training sessions with live volunteers. Radiologists agreed to review early cases with as many sonographers and radiologists as possible to increase diagnostic confidence.
Imaging protocol
The study group comprised pediatric patients presenting with abdominal pain to an urban pediatric emergency department who were suspected of having appendicitis and who consented to participate. Children were examined by a pediatric emergency medicine attending physician. Children with compelling clinical evidence of appendicitis (e.g., focal tenderness/peritonitis in the right lower quadrant, generally with leukocytosis and fever) were then evaluated by a pediatric surgery attending physician and admitted for surgery without imaging. Children who presented with right lower quadrant abdominal pain but with a history and physical exam equivocal for appendicitis underwent sonography of the right lower quadrant.
Sonography was performed by a pediatric sonographer. The procedure continued for at least 15 min or until a confident diagnosis was reached. Images were reviewed at the time of acquisition with a pediatric radiologist, who sometimes performed additional sonography.
If the sonogram was unequivocally positive, the child was referred to the surgical service. If the sonogram was unequivocally negative, the child returned to the Emergency Department with further evaluation at the discretion of the treating physician. If the US was equivocal, the child underwent pelvic CT.
CT was performed on either a 64-slice or 16-slice scanner (GE Healthcare, Waukesha, WI). Intravenous and rectal contrast media were administered according to a weight-based protocol. As the protocol progressed and clinicians became more confident in US findings, some children were not sent to CT even after an equivocal US result.
Ultrasound interpretation
Every US report included a numerical designation by the interpreting radiologist of the likelihood of appendicitis: (1) unequivocally positive, (2) probably positive, (3) probably negative or (4) unequivocally negative. These are described below.
Unequivocally positive for appendicitis
The appendix was visualized with certainty in both longitudinal and transverse sections, meaning the blind-ending tip of the appendix was seen in both planes (in the absence of a perforation). At least one of the following features was present: (1) the diameter of the appendix was >6 mm, (2) the appendix was noncompressible, (3) there was increased echogenicity of the periappendiceal fat. In the case of appendiceal rupture, the remnant of the appendix was identified in proximity to a phlegmon or abscess.
Probably positive for appendicitis
The appendix was visualized with a lesser degree of certainty than described above or not visualized at all. If visualized, the appendix measurements were variable and inconsistently >6 mm. Most cases in this category had either periappendiceal echogenic fat or hypervascularity. Some cases in this category demonstrated an enlarged appendix but no periappendiceal fluid or echogenic fat. In some cases, the appendix was not visualized, but an inflammatory mass was identified in the right lower quadrant without other apparent etiology.
Probably negative for appendicitis
The appendix was visualized with a lesser degree of certainty than described above for unequivocally positive cases, or it was not visualized at all. If visualized, the appendix measured ≤6 mm. Many cases in this category had a normal-caliber appendix that was partly visualized but the tip of the appendix was not seen with certainty. There was no echogenic fat or focal (loculated) periappendiceal fluid. If the appendix was not visualized there were no secondary findings to suggest a right lower quadrant inflammatory process. Small amounts of anechoic fluid in the right lower quadrant were sometimes seen in these children.
Unequivocally negative for appendicitis
The appendix was completely visualized with certainty in both longitudinal and transverse planes, including its blind end. It measured ≤6 mm and there was no periappendiceal echogenic fat or hypervascularity.
CT interpretation
For positive cases, the appendix was visualized in its entirety and was enlarged (>6 mm) or hyperenhancing. Strandy density in the periappendiceal fat, free fluid, free air and an appendicolith were considered supportive findings. If the appendix was not visualized but an inflammatory process or abscess in the right lower quadrant was identified without another cause, appendicitis was diagnosed. If the appendix was visualized and was ≤6 mm in size, or if the appendix was not visualized, the study was considered negative if none of the supportive findings mentioned above were present.
Clinical outcome
Patients’ electronic medical records were reviewed, including the Emergency Department record, surgical report and pathology reports. Children who underwent surgery were considered to have appendicitis if the surgical and pathology reports were concordant and positive for appendicitis. Children who did not undergo surgery were considered to be negative for appendicitis if there was no subsequent Emergency Department visit or surgical evaluation within 2 weeks of the initial encounter, either at our institution or any other institution within the same health care system. Based on established regional referral patterns, it is unlikely children went elsewhere for treatment of appendicitis missed at our institution.
Cost accounting
Except where otherwise described, costs presented are the cost to the hospital to provide imaging services and do not include associated professional fees. The hospital activity-based cost accounting system assigns unit costs to each activity that is charged to an individual patient’s account. The unit cost is derived from a methodology that takes total operating expenses and allocates them to units for all chargeable services provided. This allocation methodology is reconciled annually with actual operating expenses. The unit costs are connected to the hospital charge master. With the identified patient population, we can see actual cost for providing care across the continuum, rather than estimating the cost from the charge master charge and cost-to-charge ratio.
Sonographer experience
Pediatric sonographers who participated in the protocol were surveyed about their experience. Each sonographer reported his or her personal experience with sonography of the appendix (as a number of studies performed) before the study. Each sonographer was asked to grade his or her personal comfort level with sonography of the appendix using a five-point scale. We compared results for this comfort scale from before and after the study period.
Results
We included 512 children who were evaluated for appendicitis in the Emergency Department and consented to participate in the study during the 30-month study period. All 512 children had sonography. Of these, 187 also underwent CT. CT was avoided in 63% of patients. During the study period, of all children who underwent appendectomy, 47% had either US, CT or both prior to surgery. Fifty-three percent had no cross-sectional imaging prior to appendectomy.
Of the 512 children enrolled in the study, 176 (34%) went to surgery. Of these, 2 went to surgery for other pathology correctly diagnosed on imaging and 174 went to surgery for appendicitis suspected on imaging. Of the children who went to surgery for suspected appendicitis, 167 of 174 (96%) had appendicitis confirmed by operative findings and pathology. Seven children of 174 without appendicitis at surgery, one had an appendiceal carcinoid tumor at pathology (intraoperative diagnosis was acute appendicitis) one had a corpus luteum cyst, and five had a normal appendix without other pathological findings. The negative appendectomy rate was 4.0% (7/174). The perforation rate was 25% (41/167). Of the children who left the Emergency Department without surgery, none returned with appendicitis within 2 weeks to our institution or to any institution within the same health care system.
Ultrasound results
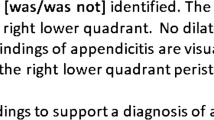
The US designations of “unequivocally positive” and “probably positive” were lumped together for data analysis (165 patients total) and considered to be US-positive (Fig. 1). US designations of “unequivocally negative” or “probably negative” (347 patients) were considered to be US-negative (Fig. 2). Using this convention, US alone had a sensitivity of 87% (145/167), specificity of 94% (325/345), positive predictive value of 88% (145/165), and negative predictive value of 94% (325/347) for diagnosing appendicitis.

Flowchart shows all children with a positive US study or a probably positive US study. Note children in each category who avoided CT

Flowchart shows all children with a probably negative US study or a negative US study. Note children in each category who avoided CT
Combined US and CT results
A combined imaging positive or negative was defined by a combination of the US and CT (when performed) results, with the CT diagnosis prevailing in cases where the US and CT reports offered discrepant opinions. Sensitivity for combined imaging was 96% (161/167), specificity 97% (334/345), positive predictive value 94% (161/172), and negative predictive value 98% (334/340).
Early and late periods
In order to compare changes in sonographer and radiologist proficiency, patient results were grouped into two 12-month periods (the first and last 12 months, excluding the middle 6 months). During the first 12-month period, the combined imaging had a sensitivity of 95% (37/39), specificity of 98% (132/135), positive predictive value of 93% (37/40), and negative predictive value of 99% (132/134). The prevalence of appendicitis during the first 12 months was 22% (39/174). During the last 12 months of the study the sensitivity was 97% (95/98), specificity was 95% (166/174), positive predictive value 92% (95/103), and negative predictive value 98% (166/169). The prevalence of appendicitis during the last 12 months was 36% (98/272). There was no statistically significant difference in these values comparing the early and late periods (Table 1). There was no statistically significant difference (P = 0.11) in the negative appendectomy rate comparing the first 12 months (4/44) to the last 12 months (3/102) of the study.
Sonographer confidence
On average, each sonographer had performed 16 US studies of the appendix (range 3–50) before the protocol change in 2009. The average self-described confidence-level score prior to the study period was 1.2, and no score was higher than 2 (range 1–5, with the lowest being least confident and highest being most confident). After the 30-month study period, the average score was 4.8, and no score was lower than 4.
Changes in use of CT
Among children undergoing advanced imaging for suspected appendicitis at our institution, the rate of CT utilization dropped from almost 90% to less than 35% during the course of the study (Fig. 3).

Graph shows utilization trends for US and CT at our facility for diagnosing appendicitis
Overall diagnostic accuracy
Throughout the transition, diagnostic accuracy remained unchanged and was comparable to other published results [7]. According to our own unpublished data, our CT-only protocol had a sensitivity of 97% (150/154) and a sensitivity of 96% (379/394) for a 1-year period in 2008–2009 (Table 2).
Cost impact
Using our hospital’s activity-based cost accounting system we estimated the annual cost to the facility (excluding professional fees) for children who presented with suspected appendicitis, comparing the year 2012 to a baseline period of 2007–2008. With a cost of $102 per US study and $245 per CT study, in 2012 US replaced CT for 241 children and US was added as an additional study for 43 children. The cases where US eliminated a need for CT reduced the cost incurred by the hospital by $34,559 annually. For the cases where both CT and US were required, the cost increase to the hospital was $4,377 annually. The US protocol resulted in a net annualized cost savings to the facility of $30,182 comparing the baseline period to 2012.
Discussion
Obstacles
Diagnostic error
Pediatric surgeons who prefer CT over US for suspected appendicitis may mandate, on the presumption of greater accuracy, that CT be performed prior to appendectomy. We addressed this concern by reviewing our US protocol results after the first 30 children (Fig. 4). Radiologists met with pediatric surgeons and with pediatric emergency medicine physicians to share data, images and problematic cases. We sought to encourage continued protocol compliance by demonstrating the diagnostic accuracy of US. Our argument was bolstered by no false-positives or false-negatives in these first 30 children and avoidance of CT in almost one-third.

Flowchart for first 30 patients in the protocol. Numbers in parentheses are patients in each category who underwent CT. Nine patients had an unequivocal US diagnosis. There were no US diagnostic errors in these patients. Eleven patients avoided CT. Note that two patients with unequivocal US diagnosis underwent CT, and four patients with equivocal US diagnosis avoided CT
Increased time
For emergency medicine physicians the prospect of a CT to follow an equivocal US examination translates into longer patient stays. Although this may be an unavoidable liability of a US protocol in its early stages, we attempted to minimize delays by asking the emergency medicine physician to order both US and CT in all children with suspected appendicitis. Children with an equivocal US went directly to CT without returning to the Emergency Department. If the CT was not necessary it was cancelled. US scanning time was limited to 15 min, and many US studies achieved an unequivocal diagnosis in less than 15 min.
Cost
In the early months of our US protocol most children underwent both US and CT. The combined cost of these studies is a legitimate concern. But over time our protocol reduced patient costs. The hospital cost accounting system revealed a $30,182 annual savings to the hospital to provide advanced imaging for patients suspected of appendicitis using the US protocol.
We often reminded our referring physician colleagues that for a few individual children who undergo both tests, the US-based protocol will result in greater imaging costs. We believed that when all practitioners participating in the US protocol understand that the patient group as a whole and the hospital are experiencing lower costs, the protocol is more likely to succeed.
Inexperience of radiologists and sonographers
In 2009 at our facility, the pediatric radiologists’ post-training work experience ranged 1–25 years. Those who had completed fellowships more recently were more likely to have received US training for suspected appendicitis. Some had worked at centers where US had been used as a primary modality for appendicitis, some had not, and none had used the technique regularly in recent practice. The pediatric sonographers’ post-training work experience ranged 2–31 years. In 2009 our least experienced sonographer had performed three right lower quadrant US studies. Our most experienced sonographer had performed approximately 50.
The pediatric radiologists and sonographers attended several 1-h didactic sessions on US technique, including hands-on practice scanning with volunteer patients, before starting the US protocol. Ongoing training for radiologists and sonographers during the protocol included review conferences on missed cases or cases where the appendix was not seen. These review conferences were initially held weekly and then every 2 months over the first year of the protocol.
Because our radiology department is relatively compact, radiologists not specifically assigned to US imaging were asked to briefly interrupt their workflow and come to the US suite to observe the critical portion of each appendicitis study. Although this required flexibility from radiologists and sonographers, the interruptions were brief and of such utility as to be generally considered worthwhile rather than a nuisance. We encouraged multiple sonographers to scan each patient, we retrospectively shared both positive and negative studies, and we held inclusive, open discussions about the protocol. These actions helped to rapidly increase individual sonographer and radiologist confidence and proficiency.
Overnight staffing
A common challenge for many nonacademic centers is the non-availability of sonographers or radiologists at certain hours when US is desired, whereas CT is often immediately available and more easily interpreted by a radiologist at a remote location [10]. In 2009 at our institution, US imaging was immediately available only during weekday daytime hours. Night and weekend US coverage was on-call and was offered only for emergent cases. Our private practice radiology group does not involve the residents and fellows we train in overnight call. Both pediatric radiologists and sonographers knew that a successful US protocol would likely result in extension of their hospital coverage hours.
The protocol was initially offered only during weekday daytime hours and for a few hours on Saturday mornings. After initial success we gradually expanded its availability. After the first year of the protocol the pediatric radiologists expanded their in-house coverage to 24/7. Institutional commitment to the protocol allowed us to extend sonographer coverage, first by extending availability hours into the evening and later by hiring sonographers to cover a late-evening shift. These staffing changes were unpopular and therefore were not mandated at the beginning of the study. Instead, we allowed the US protocol to prove itself and offered extended staff coverage only when it made sense. At the end of the study period US was available at our hospital 24/7 as the primary imaging modality for suspected appendicitis.
Collaborative approach
Underutilization of US for diagnosing appendicitis has been described [11, 12]. The obstacles to US we describe above are not unique to our institution or region. The success of our protocol was dependent on a healthy working relationship between pediatric radiologists, pediatric sonographers, pediatric emergency medicine physicians and pediatric surgeons. All these providers were involved in writing the initial protocol and were committed to participation before the study began. Because our primary motivation was the ALARA principle (making radiation dose as low as reasonably achievable), obstacles we encountered became topics for discussion rather than a way to rationalize non-participation. We recognized emergency medicine physicians would need to (initially) compromise efficiency, surgeons would need to accept an unequivocal US result as equivalent to an unequivocal CT result, and radiologists and sonographers would need to increase their proficiency and availability. Because we accepted these liabilities at the outset we did not have to renegotiate compliance with the US protocol at every patient encounter.
To encourage durable compliance with the protocol we reviewed our results frequently with pediatric surgeons and pediatric emergency medicine physicians. Although children imaged in the first 12 months of the protocol were more likely to require both CT and US compared to children in the last 12 months, we experienced an immediate decrease in CT use. Our referring physicians were uncomplaining when we made occasional diagnostic errors with US.
Our sonographer survey included this open-response question: “What factors were most influential in helping you improve your ability and confidence finding the appendix with ultrasound?” Nearly unanimous was this response: “the team approach to learning.” We sought to share every US examination with as many radiologists and sonographers as possible at the time of imaging and interpretation. Moreover, frequent review sessions provided an additional opportunity for collaborative sharing that accelerated learning for radiologists and sonographers. Although workflow patterns and geography of other imaging departments may not allow real-time, in-person dialogue about US cases, case-sharing may be applied in an online or PACS-based format. This would be particularly important wherever a relative paucity of cases presents an additional barrier to achieving proficiency.
Radiation reduction
We have documented the success of our US-based protocol for diagnosing appendicitis in terms of diagnostic accuracy [3] and hospital costs saved [4]. At least one group has also attempted to quantify radiation risk, cancer induction, and fiscal impact on future health and productivity into a cost assessment of an appendicitis imaging protocol [13]. At our pediatric institution we benefit from virtually unanimous commitment to the ALARA principle among treating physicians. With this as the fundamental principle informing our decisions about imaging children with suspected appendicitis, small obstacles such as an occasional US diagnostic error, prolonged Emergency Department stay, and overnight coverage were much easier to overcome. Our avoidance of CT in 64% of children is undeniably the most noteworthy measure of our success.
Conclusion
We demonstrate that even outside of the academic radiology setting, implementing a successful US-based imaging protocol for diagnosing appendicitis is possible. We demonstrate a preservation of diagnostic accuracy, even in the early stages of such a protocol, and an immense benefit in cost and radiation reduction.
References
Holscher H, Heij H (2009) Imaging of acute appendicitis in children: EU versus US … or US versus CT? A European perspective. Pediatr Radiol 39:497–499
Hryhorczuk A, Mannix R, Taylor G (2012) Pediatric abdominal pain: use of imaging in the emergency department of the United States from 1999 to 2007. Radiology 263:778–785
Sivit C, Applegate K, Stallion A et al (2000) Imaging evaluation of suspected appendicitis in a pediatric population: effectiveness of sonography versus CT. AJR Am J Roentgenol 175:977–980
Garcia Pena B, Taylor G, Fishman S et al (2000) Costs and effectiveness of ultrasonography and limited computed tomography for diagnosing appendicitis in children. Pediatrics 106:672–676
Krishnamoorthi R, Ramarajan N, Wang N et al (2011) Effectiveness of a staged US and CT protocol for the diagnosis of appendicitis in children: reducing radiation exposure in the age of ALARA. Radiology 259:231–239
Pearce M, Salotti J, Little M (2012) Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumors: a retrospective cohort study. Lancet 380:499–505
Doria A, Moineddin R, Kellenberger C et al (2006) US or CT for diagnosis of appendicitis in children and adults: a meta-analysis. Radiology 241:83–94
Smith-Bindman R, Miglioretti D, Johnson E (2012) Use of diagnostic imaging studies and associated radiation exposure for patients enrolled in large integrated health care systems, 1996–2010. JAMA 307:2400–2409
Larson D, Johnson L, Schnell B et al (2011) Rising use of CT in child visits to the emergency department in the United States, 2005–2008. Radiology 259:793–801
Burr A, Renaud E, Manno M et al (2011) Glowing in the dark: time of day as a determinant of radiographic imaging in the evaluation of abdominal pain in children. J Pediatr Surg 46:188–191
Hernandez JA, Swischuk LE, Angel CA et al (2005) Imaging of acute appendicitis: US as the primary imaging modality. Pediatr Radiol 35:392–395
Saito J, Yan Y, Evashwick T et al (2013) Use and accuracy of diagnostic imaging by hospital type in pediatric appendicitis. Pediatrics 131:e37–e44
Wan M, Krahn M, Ungar W (2009) acute appendicitis in young children: cost-effectiveness of us versus ct in diagnosis — a Markov decision analytic model. Radiology 250:378–386
Acknowledgments
We express our thanks to the pediatric sonographers whose expertise and dedication to pediatric imaging made this manuscript possible: Sandi Arnberg, RDMS; Carly Durrant, RDMS; Sasha Gordon, RDMS, RVT; Kandus Johnson, RDMS; Marie Newton, RDMS, RVT; Kim Nowicki, RDMS, RVT; Jeremy Olson, RDMS, RVT; Brad Watts, RDMS.
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
van Atta, A.J., Baskin, H.J., Maves, C.K. et al. Implementing an ultrasound-based protocol for diagnosingappendicitis while maintaining diagnostic accuracy. Pediatr Radiol 45, 678–685 (2015). https://doi.org/10.1007/s00247-014-3220-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-014-3220-9