
Abstract
Background
Post-contrast T1-weighted imaging is an essential component of a comprehensive pediatric abdominopelvic MR examination. However, consistent good image quality is challenging, as respiratory motion in sedated children can substantially degrade the image quality.
Objective
To compare the image quality of three different post-contrast T1-weighted imaging techniques—standard three-dimensional gradient-echo (3-D-GRE), magnetization-prepared gradient-recall echo (MP-GRE) and 3-D-GRE with radial data sampling (radial 3-D-GRE)—acquired in pediatric patients younger than 5 years of age.
Materials and methods
Sixty consecutive exams performed in 51 patients (23 females, 28 males; mean age 2.5 ± 1.4 years) constituted the final study population. Thirty-nine scans were performed at 3 T and 21 scans were performed at 1.5 T. Two different reviewers independently and blindly qualitatively evaluated all sequences to determine image quality and extent of artifacts.
Results
MP-GRE and radial 3-D-GRE sequences had the least respiratory motion (P < 0.0001). Standard 3-D-GRE sequences displayed the lowest average score ratings in hepatic and pancreatic edge definition, hepatic vessel clarity and overall image quality. Radial 3-D-GRE sequences showed the highest scores ratings in overall image quality.
Conclusions
Our preliminary results support the preference of fat-suppressed radial 3-D-GRE as the best post-contrast T1-weighted imaging approach for patients under the age of 5 years, when dynamic imaging is not essential.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Magnetic resonance imaging (MRI) has emerged as the imaging modality of choice in the evaluation of many pediatric conditions and is being increasingly used for abdominopelvic disease processes [1]. Body MRI in children can be challenging due to the variable extent of cooperation [2]. Motion artifacts due to patient movement can be a significant impediment to acquiring clinically relevant MRI information. While all subject populations are susceptible to such artifacts, these problems are especially prominent in young children, who frequently have difficulty remaining still during the required examination time. Almost all children in the age group of 0 to 5 years old require sedation for abdominopelvic MR imaging [2, 3].
Post-contrast T1-weighted imaging is an important component of abdominopelvic MRI examination and is usually performed using three-dimensional T1-weighted gradient-echo (3-D-GRE) sequences, which usually require a 15–20 s breath-hold. This method is sensitive to respiratory motion and can result in suboptimal images in patients who cannot adequately hold their breath [4, 5]. While sedation can help to control gross body motion artifacts, it cannot control respiratory motion artifacts, limiting the use of multislice T1-weighted GRE imaging in this age group. Common motion correction techniques, such as respiratory and navigator-triggering, tend to disturb the steady-state magnetization characteristically achieved with standard T1-weighted imaging, which can explain the ineffectiveness with most volumetric 2-D and 3-D T1-weighted spoiled GRE imaging [6]. A recent report from Young et al. [7] showed the feasibility of T1-weighted imaging with a modified 3-D-GRE sequence incorporating a small navigator flip angle, showing modest image quality improvement over free-breathing acquisitions. Furthermore, these techniques require additional steps in clinical workflow and can fail in cases of irregular respiration, which may be observed in pediatric patients [8, 9]. Previous studies [10–13] have described the development of a single-shot 2-D inversion-recovery magnetization-prepared gradient recalled echo (MP-GRE) technique. This T1-weighted imaging strategy is robust to motion and may be acquired in a free-breathing manner or using motion correction techniques. Other recent studies [6, 14–18] have described a new motion-robust free-breathing 3-D-GRE approach with radial data sampling (radial 3-D-GRE). This sequence uses the “stack-of-stars” scheme to acquire the k-space data. It performs conventional sampling in the slice direction but uses radial readouts for each partition, such that the data is acquired along overlapping spokes or radial views [19, 20]. This sequence has been requested as an adequate alternative for patients who cannot suspend respiration, with potential impact on pediatric MR imaging [6, 16].
To our knowledge, there are limited reports comparing different T1-weighted imaging schemes in pediatric patients [6, 16, 21]. Thus, our purpose was to assess and compare the image quality of three different post-contrast T1-weighted GRE imaging techniques: standard 3-D-GRE, MP-GRE and radial 3-D-GRE acquired in pediatric patients younger than 5 years of age at 1.5 T and 3 T.
Materials and methods
Population
Institutional review board approval was obtained for this retrospective Health Insurance Portability and Accountability Act (HIPAA) compliant study and informed consent was waived. A retrospective search for all pediatric patients younger than 5 years of age who underwent abdominal MR examination between Sept. 15, 2009, and June 30, 2010, was performed. Only studies that included at least one of the T1-weighted sequences: MP-GRE, Standard 3-D-GRE and radial 3-D-GRE at 1.5 T or 3 T were reviewed. During this accrual time, all of these T1-weighted sequences were used randomly.
Sixty consecutive exams performed in 51 patients (23 females, 28 males; mean age: 2.5 ± 1.4 years) fulfilled the search criteria and constituted the final study population. Five patients underwent 2 MR scans and 2 patients underwent 3 MR scans. Thirty-nine scans were performed at 3 T (17 males, 17 females; mean age: 2.4 ± 1.6 years) and 21 scans were performed at 1.5 T (11 males, 8 females; mean age: 2.6 ± 1.2 years). Ten MR exams included all three T1-weighted sequences (n = 4 at 1.5 T; n = 6 at 3 T). Twenty-four MR exams included MP-GRE and 3-D-GRE T1-weighted sequences (n = 3 at 1.5 T; n = 21 at 3 T). Six MR exams included MP-GRE and radial 3-D-GRE T1-weighted sequences at 1.5 T. Twenty MR exams included a single T1-weighted sequence: MP-GRE (n = 8 at 1.5 T; n = 10 at 3 T) or 3-D-GRE (n = 2 at 3 T).
All MR examinations were obtained for clinical evaluation. The primary indications included: neuroblastoma evaluation and post-treatment surveillance (n = 10); Wilms tumor evaluation and post-treatment surveillance for renal neoplasms (n = 10); unexplained persistent fever (n = 6); abdominal mass (n = 4); evaluation of liver lesion(s) (n = 4); renal mass evaluation (n = 3); pancreatic disease including pancreatitis or pseudocyst evaluation (n = 3); post hepatoblastoma resection surveillance (n = 2); neurofibromatosis (n = 2); post sacrococcygeal tumor resection surveillance (n = 2); liver hemangioendothelioma surveillance (n = 2); post rhabdomyosarcoma resection surveillance (n = 1); myofibrosis (n = 1); post liver laceration evaluation (n = 1); adrenal mass evaluation (n = 1); abdominal pain (n = 1); hemorrhoids (n = 1); maternal carcinomatosis (n = 1); post liver transplant surveillance (n = 1); spina bifida (n = 1); choroid plexus tumor (n = 1), neck mass (n = 1) and elevated liver enzymes (n = 1).
We tried to adjust for different scanning times on the qualitative image evaluation and comparisons were made with the contrast-enhanced interstitial phase acquisition data sets that were closest to the time of injection.
MRI technique
MR imaging was performed at 1.5 T (Avanto; Siemens Medical Systems, Malvern, PA) and 3 T (Magnetom trio; Siemens Medical Systems, Malvern, PA) MR systems using a phased-array torso coil.
All patients underwent post-contrast imaging, which was performed following intravenous administration of gadopentetate dimeglumine (0.1 mmol/kg) (Magnevist; Bayer Schering, Berlin, Germany).
Three types of post-contrast T1-weighted techniques were used in this study: Standard Cartesian 3-D-GRE, 2-D MP-GRE and radial 3-D-GRE. Detailed parameters of the sequences are shown in Table 1.
Standard Cartesian 3-D-GRE (VIBE) is a conventional and routinely used sequence with short repetition time and the shortest out-of-phase echo time in which central k-space lines can be acquired volumetrically in a segmented fashion, within the early portion of data acquisition.
Two-dimensional MP-GRE is considered a motion resistance sequence in which the center of the k-space is acquired a time TI (inversion time) after the initial non-selective 180 preparatory inversion pulse. All the lines for a given slice are acquired after a single inversion pulse with total echo-train duration of about 1 s to avoid respiratory motion artifacts. Although the inversion pulse is non-selective, and not strictly a single-shot technique from a magnetization relaxation perspective, it behaves like a single-shot sequence regarding motion artifacts. A free-breathing version with fat suppression (water excitation) was used in post-contrast acquisitions [22].
Radial 3-D-GRE sequence is a spoiled steady-state gradient sequence, in which the readout direction is altered each repetition, and every acquired line passes through the center of k-space such that the sampling pattern in k-space is not a rectangular grid, but is a set of radial spokes. K-space data are acquired along coinciding projections rather than parallel lines, as done in conventional standard Cartesian phase-encoding acquisitions, each line passing through the center of k-space with a different angle for each line [18]. This type of sampling is often known as stack of stars. In this sequence, 300 radial spokes were used. The radial data are re-gridded onto a rectangular k-space grid before standard reconstruction [23]. Radial data acquisition provides high spatial resolution with low aliasing and low motion sensitivity [24].
The primary intention for using different techniques was to assess ease of use by the technologist and tolerability by patients and for general and medical acceptability of image quality in the spectrum of pediatric population imaged for abdominal diseases.
All patients underwent sedation and the exams were performed in a free-breathing manner. Sedative drugs were prescribed at the discretion of the radiologist following clinical assessment and physical examination in accordance with our institutional sedation guidelines.
Qualitative analysis
One radiologist (A.R.) randomly uploaded the sequences on a commercially available PACS workstation (IMPAX 6.0; Agfa Healthcare®, Greenville, SC), which were then retrospectively and independently evaluated by two radiologists (V.H. and M.R.) with 4 and 5 years of experience, respectively. Both readers were blinded to sequence parameters and the patients’ clinical histories. For each data set, both readers scored seven image quality parameters. The readings were done in two sessions. Prior to conducting the evaluation, both readers reviewed a 10-patient training set, which was not used in the study, and came to agreement on scoring each of the evaluated parameters.
The readers graded each sequence for the presence and extent of artifacts (respiratory motion, misregistration, streak and shading artifacts) using a 5-point scale (1, severe; 2, moderate; 3, mild; 4, minimal; 5, absent). Sharpness (hepatic edge, pancreatic edge and hepatic vessel clarity) was rated using a 5-point scale (1, unreadable; 2, extreme blur; 3 moderate blur; 4, mild blur; 5, no blur).
Respiratory motion artifact was defined as blurring or ghosting of the image in the phase-encoding direction, if applicable, or increase in streak artifact. Spatial misregistration was defined as nonconformity of slice position evident by discontinuity or overlap between abdominal structures along the z-axis. Streak artifact arises in radial imaging when an inadequate number of planes causes breakdown in the interpolation process necessary to create correct k-space, resulting in streaking in the reconstructed image [6]. Shading artifact was defined as nonuniformity of signal intensity throughout the slice, mainly along the phase-encoding direction.
Overall image quality was graded on a 5-point scale (1, poor; 2, fair; 3, good; 4, very good; 5, excellent). Overall image quality was assessed using the following considerations: image sharpness, homogeneity of signal intensity, liver and pancreatic signal intensity, and extent of artifacts.
Statistical analysis
Kappa statistics were used to assess the interobserver agreement for the independent qualitative data analysis using a standard Landis and Koch schema [25].
For qualitative ratings of image quality, the Kruskal-Wallis nonparametric test was used to assess statistically significant differences among the three sequences at 1.5 T and 3 T. For those parameters in which a statistically significant difference in ratings was observed, a comparison between pairs of sequences was then made using the Mann–Whitney U test.
Associations were considered statistically significant if two-tailed analyses showed a P<0.05. A Bonferroni correction for multiple comparisons (three comparisons) was applied and P<0.017 were considered statistically significant.
All statistical analyses were performed using IBM SPSS Statistics for Mac OS X, Version 22; IBM Corp (Armonk, NY).
Results
Kappa values for independent qualitative data analyses were as follows: 0.41–0.60 (11%), 0.61–0.80 (33%), and >0.80 (56%), representing moderate to excellent agreement between the two readers.
The average scores of all evaluated parameters including artifacts and overall image quality in free-breathing 3-D-GRE, MP-GRE and radial 3-D-GRE acquisitions at 1.5 T and 3 T are displayed in Tables 2 and 3. Concerning respiratory motion, MP-GRE and radial 3-D GRE sequences had the highest mean score ratings at 1.5-T and 3-T systems (p < 0.0001) (Fig. 1). MP-GRE sequences displayed the minimum score ratings for misregistration (Fig. 2).

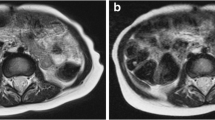
MR scan of a 3-year-old boy with history of choroid plexus tumor performed at 1.5 T. Post-contrast standard Cartesian Standard 3-D-GRE (a) shows and post-contrast radial 3-D-GRE (b) sequences. Standard 3-D-GRE (a) show substantial degradation due to respiratory motion. Post-contrast radial 3-D-GRE-image (b) quality was significantly better than free-breathing standard 3-D-GRE (a)

MR scan of a 3-year-old girl with history of renal clear cell sarcoma, post resection, performed at 1.5 T. Post-contrast MP-GRE (a) and post-contrast standard Cartesian 3-D-GRE (b) sequences. Post-contrast MP-GRE images demonstrate motion-robustness characteristics (a) with good image quality. Standard 3-D-GRE shows mild to moderate respiratory motion (b)
Streak artifacts were only present in radial 3-D-GRE sequences, with score ratings ranging from mild to absent.
At 1.5 T, radial 3-D-GRE sequences had significantly higher average image quality scores ratings compared to both 3-D-GRE (p = 0.001) and MP-GRE (p < 0.0001) sequences. At 3 T, MP-GRE and radial 3-D-GRE sequences showed the highest scores ratings in overall image quality (Fig. 3); the former, statistically significant compared to 3-D-GRE sequences (p < 0.0001).

MR scan of a 4-year-old boy with history of alpha-1 antitrypsin deficiency performed at 3 T. Post-contrast MP-GRE (a), post-contrast standard Cartesian 3-D-GRE (b), and post-contrast radial 3-D-GRE (c) sequences. MP-GRE (a) and radial 3-D-GRE (c) show less motion susceptibility; however, radial 3-D-GRE (c) images display higher image quality with almost no blur along the liver and pancreatic edges. Mild respiratory motion is noted on standard Cartesian 3-D-GRE (b) slightly degrading image quality. This inconsistent finding may be related to a more shallow respiration, without significant variations in amplitude throughout the respiratory cycle
Discussion
Our study evaluated the image quality of three types of post-contrast T1-weighted GRE sequences in sedated pediatric patients younger than 5 years of age at 1.5 T and 3 T. To our knowledge, this is the first study to evaluate three T1-weighted sequences in this age group.
Our results demonstrated that good-quality post-contrast T1-weighted imaging is achievable, and that free-breathing radial 3-D-GRE and MP-GRE sequences in sedated children constitute a comprehensive scanning approach with consistently good overall image score ratings at both 1.5 T and 3 T.
The parameters of image quality; including liver and pancreatic edge sharpness, hepatic vessel clarity, and shading were scored higher by both readers for the MP-GRE and radial 3-D-GRE sequences than those for the standard 3-D-GRE at both 1.5 T and 3 T. However, there was no significant difference between the former two. Three-dimensional imaging sequences usually demonstrate diminished organ outline delineation [11]. However, the better performance of radial 3-D-GRE sequences may be related to the diminished respiratory motion and shading effect, in addition to the use of a higher matrix resolution.
The degradation of image quality in standard 3-D-GRE sequences is related to their sensitivity to respiratory motion [4, 5]. While sedation and general anesthesia can help control gross body motion artifacts, they cannot control respiratory motion artifacts. Decreased sensitivity to motion is a clear advantage of radial k-space sampling in radial 3-D-GRE, and to the single-shot nature of MP-GRE [6, 10–18]. With radial 3-D-GRE, the radial sampling pattern, in which, the readout direction is altered each repetition, and every acquired line passes through the center of k-space, translates into decreased motion susceptibility [6, 15, 17]. The single-shot nature of MP-GRE, where each slice is acquired in less than 1 s, explains its resistance to movement [12]. These advantages have been observed in prior studies [10–13].
One advantage of radial 3-D-GRE over MP-GRE is its multislice capability without misregistration between slices. As expected, minor misregistration of slices was mainly found in MP-GRE sequences related to the single-shot type of the sequence. Interestingly, the score ratings ranged between mild and absent. We conjecture that sedated children in this age group have more shallow respiration patterns, without significant variations in amplitude throughout the respiratory cycle.
Streak artifacts are only found in radial 3-D-GRE sequences [6, 15, 23] and they have the potential to degrade image quality and obscure image details. These artifacts are caused by respiratory motion, but may also result from undersampling [26], which particularly occurs in larger patients [18]. Structures that experience motion can also appear slightly blurry with the radial acquisition scheme [16]. These streak artifacts in radial 3-D-GRE sequences had average ratings scores ranging between absent and mild, without significant reduction in image quality. This may be explained by the smaller abdominal circumference in small children compared to that of adults and by the patients’ arms remaining outside the field of view [18]. This observation concurs with previously published data by Azevedo et al. [6] and Chandarana et al. [16] representing an additional advantage of radial 3-D-GRE in pediatric imaging. For radial acquisitions of k-space, distortions of the magnetic B0 field and gradient fields distant from the isocenter can cause significant streaking artifacts [26] and degrade image quality, particularly if the excited object volume exceeds the region of linear gradient fields along the z-direction. One simple alternative may be the acquisition of axial isotropic, high-resolution images allowing high-quality multiplanar reformation [18].
The radial sampling scheme is more vulnerable to off-resonance effects than the standard Cartesian 3-D-GRE sequences. Standard 3-D-GRE sequences use different readout directions to perform k-space sampling. Strongly off-resonant signals, like fat, cause signal blurring instead of a unidirectional chemical shift; therefore, it is essential to perform radial 3-D-GRE sequences with fat saturation [16].
Despite the higher overall image quality scores of radial 3-D-GRE in comparison with MP-GRE, they were only significant at 1.5 T. The 2-D nature of MP-GRE, along with minor misregistration between slices, should favor the use of radial 3-D-GRE sequences for post-contrast evaluation.
One limitation of radial 3-D-GRE is the relatively long acquisition time (64–156 s in our study). These long acquisition times of radial 3-D-GRE sequence restrict its utility in dynamic imaging [6, 15]. Portal and equilibrium phase examinations can be performed with radial 3-D-GRE sequences. However, the acquisition of the hepatic arterial phase cannot be achieved with the conventional approach. One option may be the use of k-space weighted image contrast (KWIC) reconstruction, which provides high temporal resolution by acquiring undersampled data sets; permitting reduction in the number of projections and MR data acquisition time [27]. This approach may generate reconstructed time-resolved subframe images. However, KWIC reconstruction needs further optimization a decreasing number of views leads to streak artifacts [15] and the temporal profile of pixels near the edges of the lesions may be less accurate, particularly during the initial contrast arrival period when the signal is rapidly changing [19, 27], and also may increase image blurring [15, 27]. An additional limitation of radial 3-D-GRE is that it is not yet commercially available and only accessible under generalized manufacturer research agreement; however, due to its good image quality, our center has been using it since 2010 as the main post-contrast T1-weighted sequence in patients with breath-hold difficulties.
This study has some limitations related to the retrospective nature of the study, unavailability of all three sequences in all patients, and nonuniformity of the pediatric abdominopelvic imaging protocols related to the lack of consensus of which T1-weighted sequence performs better in this age subgroup. Another limitation is the lack of liver lesion detection and conspicuity evaluation on the tested sequences, mainly due the follow-up nature of the treated diseases in the majority of evaluated patients and the small number of lesions. Based on prior reports [11, 12, 16, 18], we anticipate that detection and conspicuity of liver lesions on pre- and post-contrast MP-GRE and radial 3-D-GRE will be satisfactory, and improved compared to free-breathing standard 3-D-GRE.
Another possible limitation is the noninclusion of controlled apnea T1-weighted imaging approach, in which high image quality is expected with standard 3-D-GRE sequences due to the arrest of the mechanical ventilation in anesthetized children during the acquisition of the sequence [28]. This approach was deliberately excluded from our study due to the paucity of patients undergoing this imaging approach and our choice to focus on sequences that can be easily translated for daily clinical practice. This choice is based on the logistical problems associated with the procedure and greater risks associated with general anesthesia compared to sedation.
Another limitation is related to the remote period of data collection, during which three different T1-weighted sequences were randomly at use at both 1.5 T and 3 T systems, including standard 3-D-GRE, radial 3-D-GRE and MP-GRE sequences. To our knowledge, these are still the same sequences currently at use and with the same level of development.
Conclusion
The improved T1-weighted image quality of MP-GRE and radial 3-D-GRE acquisitions showed that respiratory motion of sedated young children can be overcome. Our results support the preference of radial 3-D-GRE as the best post-contrast T1-weighted imaging approach for patients younger than the age of 5 years.
References
Chavhan GB, Babyn PS, Vasanawala SS (2013) Abdominal MR imaging in children: motion compensation, sequence optimization, and protocol organization. Radiographics 33:703–719
Darge K, Anupindi SA, Jaramillo D (2011) MR imaging of the abdomen and pelvis in infants, children, and adolescents. Radiology 261:12–29
Shankar VR (2008) Sedating children for radiological procedures: an intensivist’s perspective. Pediatr Radiol 38:S213–S217
Maki JH, Chenevert TL, Prince MR (1997) The effects of incomplete breath-holding on 3D MR image quality. J Magn Reson Imaging 7:1132–1139
Noterdaeme O, Gleeson F, Phillips RR et al (2007) Quantification of missing and overlapping data in multiple breath hold abdominal imaging. Eur J Radiol 64:273–278
Azevedo RM, de Campos RO, Ramalho M et al (2011) Free-breathing 3D T1-weighted gradient-echo sequence with radial data sampling in abdominal MRI: preliminary observations. AJR Am J Roentgenol 197:650–657
Young PM, Brau AC, Iwadate Y et al (2010) Respiratory navigated free breathing 3D spoiled gradient-recalled echo sequence for contrast-enhanced examination of the liver: diagnostic utility and comparison with free breathing and breath-hold conventional examinations. AJR Am J Roentgenol 195:687–691
Morita S, Ueno E, Suzuki K et al (2008) Navigator-triggered prospective acquisition correction (PACE) technique vs. conventional respiratory-triggered technique for free-breathing 3D MRCP: an initial prospective comparative study using healthy volunteers. J Magn Reson Imaging 28:673–677
McConnell MV, Khasgiwala VC, Savord BJ et al (1997) Comparison of respiratory suppression methods and navigator locations for MR coronary angiography. AJR Am J Roentgenol 168:1369–1375
Ramalho M, Herédia V, de Campos RO et al (2012) In-phase and out-of-phase single-shot magnetization-prepared gradient recalled echo: description and optimization of technique at 1.5 T. Radiologia 56:136–147
Ramalho M, Herédia V, de Campos RO et al (2012) In-phase and out-of-phase gradient-echo imaging in abdominal studies: intra-individual comparison of three different techniques. Acta Radiol 53:441–449
Ferreira A, Ramalho M, de Campos RO et al (2012) Comparison of T1-weighted in- and out-of-phase single shot magnetization-prepared gradient-recalled-echo with three-dimensional gradient-recalled-echo at 3.0 Tesla: preliminary observations in abdominal studies. J Magn Reson Imaging 35:1187–1195
Herédia V, Ramalho M, de Campos RO et al (2011) Comparison of a single shot T1-weighted in- and out-of-phase magnetization prepared gradient recalled echo with a standard two-dimensional gradient recalled echo: preliminary findings. J Magn Reson Imaging 33:1482–1490
Chandarana H, Feng L, Block TK et al (2013) Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging, and golden-angle radial sampling. Investig Radiol 48:10–16
Chandarana H, Block TK, Rosenkrantz AB et al (2011) Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Investig Radiol 46:648–653
Chandarana H, Block TK, Winfeld MJ et al (2013) Free-breathing contrast-enhanced T1-weighted gradient-echo imaging with radial k-space sampling for paediatric abdominopelvic MRI. Eur Radiol 24:320–326
Bamrungchart S, Tantaway EM, Midia EC et al (2013) Free-breathing three-dimensional gradient echo-sequence with radial data sampling (radial 3D-GRE) examination of the pancreas: comparison with standard 3D-GRE volumetric interpolated breathhold examination (VIBE). J Magn Reson Imaging 38:1572–1577
Reiner CS, Neville AM, Nazeer HK et al (2013) Contrast-enhanced free-breathing 3D T1-weighted gradient-echo sequence for hepatobiliary MRI in patients with breath-holding difficulties. Eur Radiol 23:3087–3093
Lin W, Guo J, Rosen MA et al (2008) Respiratory motion-compensated radial dynamic contrast-enhanced (DCE)-MRI of chest and abdominal lesions. Magn Reson Med 60:1135–1146
Song HK, Dougherty L (2004) Dynamic MRI with projection reconstruction and KWIC processing for simultaneous high spatial and temporal resolution. Magn Reson Med 52:815–824
Vasanawala SS, Iwadate Y, Church DG et al (2010) Navigated abdominal T1-W MRI permits free-breathing image acquisition with less motion artifact. Pediatr Radiol 40:340–344
Altun E, Semelka RC, Dale BM et al (2008) Water excitation MPRAGE: an alternative sequence for postcontrast imaging of the abdomen in noncooperative patients at 1.5 Tesla and 3.0 Tesla MRI. J Magn Reson Imaging 27:1146–1154
Dale B, Wendt M, Duerk JL (2001) A rapid look-up table method for reconstructing MR images from arbitrary k-space trajectories. IEEE Trans Med Imaging 20:207–217
Peters DC, Botnar RM, Kissinger KV et al (2006) Inversion recovery radial MRI with interleaved projection sets. Magn Reson Med 55:1150–1156
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Xue Y, Yu J, Kang HS et al (2012) Automatic coil selection for streak artifact reduction in radial MRI. Magn Reson Med 67:470–476
Kim KW, Lee JM, Jeon YS et al (2013) Free-breathing dynamic contrast-enhanced MRI of the abdomen and chest using a radial gradient echo sequence with k-space weighted image contrast (KWIC). Eur Radiol 23:1352–1360
Saleh RS, Patel S, Lee MH et al (2007) Contrast-enhanced MR angiography of the chest and abdomen with use of controlled apnea in children. Radiology 243:837–846
Conflicts of interest
The authors declare that there is no conflict of interests regarding the publication of the article entitled “Post-contrast T1-weighted sequences in pediatric abdominal imaging: comparative analysis of three different sequences and imaging approach” in Pediatric Radiology.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Roque, A., Ramalho, M., AlObaidy, M. et al. Post-contrast T1-weighted sequences in pediatric abdominal imaging: comparative analysis of three different sequences and imaging approach. Pediatr Radiol 44, 1258–1265 (2014). https://doi.org/10.1007/s00247-014-2969-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-014-2969-1