
Abstract
Background
Much has been written regarding the incidence, types, importance and management of abdominal CT incidental findings in adults, but there is a paucity of literature on incidental findings in children.
Objective
We sought to determine the prevalence and characteristics of extra-appendiceal and incidental findings in pediatric abdominal CT performed for suspected appendicitis.
Materials and methods
A retrospective review was performed of abdominal CT for suspected appendicitis in a pediatric emergency department from July 2010 to June 2012. Extra-appendiceal findings were recorded. Any subsequent imaging was noted. Extra-appendiceal findings were divided into incidental findings of doubtful clinical significance, alternative diagnostic findings potentially providing a diagnosis other than appendicitis explaining the symptoms, and incidental findings that were abnormalities requiring clinical correlation and sometimes requiring further evaluation but not likely related to the patient symptoms.
Results
One hundred sixty-five children had abdominal CT for suspected appendicitis. Seventy-seven extra-appendiceal findings were found in 57 (34.5%) patients. Most findings (64 of 77) were discovered in children who did not have appendicitis. Forty-one of these findings (53%) could potentially help explain the patient’s symptoms, while 30 of the findings (39%) were abnormalities that were unlikely to be related to the symptoms but required clinical correlation and sometimes further work-up. Six of the findings (8%) had doubtful or no clinical significance.
Conclusion
Extra-appendiceal findings are common in children who undergo abdominal CT in the setting of suspected appendicitis. A significant percentage of these patients have findings that help explain their symptoms. Knowledge of the types and prevalence of these findings may help radiologists in the planning and interpretation of CT examinations in this patient population.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
As the utilization of imaging technology has increased in recent decades and as imaging resolution has improved, there has been a concomitant increase in the number of incidental findings or detected abnormalities that were not suspected and are not related to the primary purpose of the examination. In this investigation, we recorded extra-appendiceal findings, some of which can be designated as alternative diagnostic findings that may help explain patient symptoms, and others of which are purely incidental findings that were not in the appendix (the primary target of the examination), that were not suspected by the emergency physician before the exam was performed and that were unlikely to be related to the acute symptoms.
Such incidental findings can lead to further diagnostic testing and increased costs that do not always result in patient benefit, bringing about efforts to create management algorithms of incidental findings [1]. On the other hand, the alternative diagnostic findings potentially explain the symptoms and guide patient management.
Many studies have investigated the frequency and effects of incidental findings, predominantly related to CT examinations [2–4]. Some investigators have focused more specifically on abdominal CT and its related incidental findings, with various strategies utilized to subdivide the incidental findings into levels of importance or other subcategories [5–10].
These studies have focused entirely or primarily on adults undergoing abdominal CT. There is a paucity of data regarding incidental findings in children undergoing abdominal CT.
Our purpose was to assess the prevalence and characteristics of extra-appendiceal and incidental findings detected on multidetector CT performed in children in the emergency department with right lower quadrant abdominal pain suspected of having acute appendicitis.
Materials and methods
This retrospective descriptive study was Health Insurance Portability and Accountability Act-compliant with institutional review board approval. Informed consent was waived. A total of 165 children (80 male, 85 female) with a mean age of 12.1 years (range: 2.5–18 years) were referred from the emergency department from July 2010 to June 2012 for evaluation of right lower quadrant pain and suspected acute appendicitis.
This relatively low number likely reflects the fact that, at our institution, appendiceal sonography is the primary method of evaluation in the setting of suspected appendicitis. Such appendiceal sonography at our institution is focused and targeted to the appendix, without formal evaluation of other areas such as the uterus and ovaries or the kidneys.
CT of the abdomen and pelvis was performed with a Somatom Sensation 64-slice CT scanner (Siemens, Erlangen, Germany) with two techniques based on weight, dividing patients into those weighing 55 lb. or less and those weighing more than 55 lb. The first group was scanned with a technique of 68 mAs, 100 kVp, pitch 1.0, slice reconstruction thickness 3 mm. The second group was scanned with 140 mAs, 120 kVp, pitch 0.8, slice reconstruction thickness 5 mm.
Oral contrast medium Gastrografin (Bracco, Princeton, NJ, USA) diluted with juice was administered. Patients ages 2–5 years received 8 ml contrast medium with 240 ml juice. Patients 6–10 years old received 12 ml contrast medium and 360 ml juice. Patients older than 10 years of age received 16 ml contrast medium and 540 ml juice.
Intravenous contrast medium (Omnipaque 300; GE Healthcare, Waukesha, WI, USA) was administered with a dose of 1–2 ml/kg (varies by age and size of intravenous line in place), infused by a Medrad power injector (Bayer Healthcare, Wayne, NJ, USA) through a peripheral intravenous line (22 gauge or larger).
All studies were retrospectively reviewed by a pediatric radiologist with 40 years of experience (S.M.) and evaluated for the presence or absence of extra-appendiceal findings. The patients were subdivided by age into preschool-age children (2–5 years, n = 10), middle childhood (5–12 years, n = 64) and adolescents (12–18 years, n = 91).
The extra-appendiceal findings were categorized into incidental findings of doubtful or no clinical significance including anatomical variants (group 1), unexpected abnormalities potentially explaining the patient’s symptoms (group 2) that could be labeled alternative diagnostic findings, and incidental findings probably unrelated to the patient symptoms that require clinical correlation and sometimes require further diagnostic evaluation or management (group 3). Some of the alternative diagnostic findings may not have actually been related to the patient symptoms, in which case they could be thought of as truly incidental. It is not always possible to definitively distinguish between alternative diagnostic findings and incidental findings.
The extra-appendiceal findings were divided by system into the following subgroups: cardiovascular, musculoskeletal (MSK), gastrointestinal (GI), renal, pulmonary and female reproductive. The rates of appendicitis and incidental findings were calculated for the total number of patients and for each age group.
Results
A total of 77 extra-appendiceal findings of various types were found in 57 (34.5%) of the 165 children (Table 1). The majority of these findings could not have been found before the CT, as the appendiceal sonography performed before CT at our institution would not have evaluated the areas in which these findings were discovered and/or would not have had the ability to demonstrate the finding discovered on CT. Some of the extra-appendiceal findings could have been found on appendiceal US in addition to CT, such as terminal ileitis in the right lower quadrant. Our CT cases represent patients in whom such findings were not found before the CT. At our institution, this is sometimes because the patient had the CT at an outside institution before transfer, although we would have started with appendiceal sonography had the patient come first to our institution.
In patients with at least one extra-appendiceal finding, the mean number of findings per patient was 1.35 (range: 1–5). According to organ system, the distribution of extra-appendiceal findings was: GI in 35 (45.4%), female reproductive in 12 (15.6%), MSK in 9 (11.7%), renal in 8 (10.4%), pulmonary in 7 (9.1%), and cardiovascular in 6 (7.8%). Incidental findings were discovered in 3 of 10 preschool-age children (30%), 21 of 64 middle childhood patients (32.8%) and 33 of 91 adolescents (36.2%).
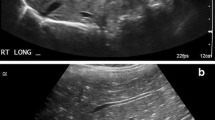
Six (7.8%) of the extra-appendiceal findings (group 1) represented observations that were not likely to have immediate clinical significance, such as a single or horseshoe kidney or anatomical variations like a retroaortic left renal vein. Some of these findings have only potential medical relevance, such as a left sided IVC that would be important to be aware of in the setting of IVC filter placement but was not relevant to the acute problem and may never have clinical significance in the life of the patient. Figure 1 demonstrates examples of group 1 findings.

Examples of group 1 extra-appendiceal findings. a Axial contrast-enhanced CT image in a 12-year-old boy demonstrates a horseshoe kidney with an isthmus of renal parenchymal tissue (arrow) connecting the two kidneys. b Coronal contrast-enhanced CT image in a 12-year-old girl shows congenital absence of the right kidney
Forty-one (53.2%) of the findings (group 2) provided a possible alternative diagnosis that could potentially explain the patient’s symptoms, such as an omental infarction, pelvic inflammatory disease, mesenteric adenitis, an ovarian cyst, pneumonia, enteritis/colitis or vaginal distention. Figure 2 demonstrates examples of group 2 findings.

Examples of group 2 incidental findings. a Axial contrast-enhanced CT in a 10-year-old boy demonstrates a focal region of omental fat (arrow) with heterogeneous inflammatory fat stranding consistent with an omental infarct treated with pain control medications until spontaneous resolution. b Axial contrast-enhanced CT in a 15-year-old girl with right lower quadrant pain demonstrates marked thickening of the terminal ileum (arrow). She was given a diagnosis of Crohn disease and eventually required partial bowel resection. Pathology showed a transmural acute and chronic inflammatory cell infiltrate and marked serositis consistent with Crohn disease. c Coronal contrast-enhanced CT in a 16-year-old girl with acute abdominal pain eventually thought to be due to Dietl’s crisis (acute flank pain due to sudden onset obstruction) after discovery of moderate right pelvicaliectasis without ureteral dilation. The girl underwent laparoscopic pyeloplasty. d Coronal contrast-enhanced CT in a 15-year-old girl with lower abdominal pain. A large mass (arrows) containing mixed areas of calcific, soft tissue and fat attenuation was discovered in the pelvis consistent with an ovarian teratoma. A salpingo-oophorectomy was performed, with pathology showing marked vascular congestion, hemorrhage and ischemic necrosis in the left ovarian parenchyma consistent with torsion
Thirty (39%) of the findings (group 3) represented true abnormalities but were findings were unlikely to explain the acute symptoms. These incidental findings require clinical correlation. For example, the observation of air trapping should be correlated with any clinical suspicion of asthma or viral airway disease. Some of these findings were probably benign and are not likely to require further attention such as a small, solitary lung nodule in a child without a history of malignancy. Other findings in this group could trigger further evaluation of some kind (imaging, specialist consultation, etc.) such as a duplex renal collecting system that might lead to a urology consultation and a voiding cystourethrogram to evaluate for the possibility of reflux in the duplex kidney. Other findings in this group are abnormal but so nonspecific that they may not be helpful in the clinical evaluation of the child, such as isolated splenomegaly. Other findings in this group are not likely related to the acute presentation but might have clinical relevance, such as a pars defect in a child who also had chronic back pain.
Seventy-two of the 165 patients (43.6%) were diagnosed with appendicitis on CT. The rate of appendicitis by age group was 9/10 (90%) in preschool-age patients, 37/64 (57.8%) in middle childhood patients and 26/91 (28.6%) in adolescents.
Thirteen of the extra-appendiceal findings occurred in children with appendicitis. Sixty-four of these findings occurred in children without appendicitis.
All of the group 1 findings occurred in children who did not have appendicitis.
Three of the 41 (7.3%) group 2 findings were discovered in children who had appendicitis, one with gallstones and two with enlarged mesenteric lymph nodes (which could be related to the appendicitis). Thirty-eight out of the 41 (92.7%) group 2 findings were discovered in children who did not have appendicitis.
Ten of the 30 (33.3%) group 3 findings occurred in children with appendicitis.
In 14 of the 57 cases (24.5%) that had extra-appendiceal findings, further imaging was obtained. Further imaging studies were varied and included MRI, MR venography, MR enterography, abdominal US, pelvic US and fluoroscopic upper gastrointestinal series with small bowel follow-through.
Discussion
Ultrasound of the right lower quadrant and CT of the abdomen and pelvis are routinely performed for evaluation of abdominal pain in children [11–15]. At our institution, we perform US first in patients with right lower quadrant pain and in girls with possible gynecological pain. If US is inconclusive and further evaluation is clinically indicated, we perform CT with oral and intravenous contrast administration. Appendicitis is often diagnosed, and we found that in patients who do not have appendicitis, CT often shows another source of abdominal pain.
As image quality improves and CT provides better visualization of abdominal organs, there is a higher probability of incidental findings. In our study, for example, 34.5% of the CT examinations had extra-appendiceal findings, a significant number of which are truly incidental, both unexpected and unrelated to the clinical presentation.
About half of the extra-appendiceal findings were potentially relevant to the clinical presentation of the patient. These group 2 findings have a significant chance of influencing patient management in the acute setting. Some of these findings would do so because they would trigger a medical intervention not previously considered, such as anticoagulation for unsuspected deep venous thrombosis. Other findings would trigger a surgical intervention other than appendectomy, such as the presence of an ovarian dermoid. Still others would terminate the consideration of a surgical intervention, such as the discovery of an omental infarct.
There has been discussion in the past of performing a limited CT for appendicitis with a smaller field of view focused only on the level of the right lower abdominal quadrant [16–18]. In our series, if a more limited field of view CT had been performed, some of the extra-appendiceal findings providing alternative diagnoses to explain the patient’s symptoms would have been missed, such as an unexpected lung base pneumonia or some of the renal findings. This does not necessarily imply a justification for scanning the entire abdomen and pelvis in every case of suspected appendicitis, but knowing the types and frequency of extra-appendiceal findings that potentially change patient management may be helpful to radiologists planning the field of view of CT examinations in this patient population.
Our study is also limited in its scope, as this patient population was selected by the evaluating physician in the emergency department for suspected appendicitis.
This study does not attempt to establish the most cost-effective strategy for the further evaluation and management of pediatric incidental CT findings. Such cost-effectiveness studies are lacking, and research on that issue would be helpful to guide the management of these patients.
Another limitation of the study is that the CT examinations were reviewed by only one pediatric radiologist. We did not attempt to establish the level of concordance between radiologists in the discovery and interpretation of these findings.
Conclusion
There is a relatively high rate of extra-appendiceal findings on CT performed in children with suspicion of acute appendicitis. A significant number of these findings provides an alternative diagnosis potentially explaining the patient’s symptoms. Radiologists should be aware of the potential extra-appendiceal findings, particularly those that may provide an alternative diagnosis other than appendicitis. More research is needed on the most cost-effective strategy for management of pediatric abdominal CT incidental findings.
References
Berland LL, Silverman SG, Gore RM et al (2010) Managing incidental findings on abdominal CT: white paper of the ACR incidental findings committee. J Am Coll Radiol 7:754–773
Lumbreras B, Donat L, Hernandez-Aguado I (2010) Incidental findings in imaging diagnostic tests: a systematic review. Br J Radiol 83:276–289
Thompson RJ, Wojcik SM, Grant WD et al (2011) Incidental findings on CT scans in the emergency department. Emerg Med Int 2011:624847
Paluska TR, Sise MJ, Sack DI et al (2007) Incidental CT findings in trauma patients: incidence and implications for care of the injured. J Trauma 62:157–161
Pickhardt PJ, Hanson ME, Vanness DJ et al (2008) Unsuspected extracolonic findings at screening CT colonography: clinical and economic impact. Radiology 249:151–159
Hellstrom M, Svensson MH, Lasson A (2004) Extracolonic and incidental findings on CT colonography (virtual colonoscopy). AJR Am J Roentgenol 182:631–638
Berland LL (2009) Incidental extracolonic findings on CT colonography: the impending deluge and its implications. J Am Coll Radiol 6:14–20
Berland LL (2011) The American College of Radiology strategy for managing incidental findings on abdominal computed tomography. Radiol Clin North Am 49:237–243
Green DE, Woodward PJ (2005) The management of indeterminate incidental findings detected at abdominal CT. Semin Ultrasound CT MR 26:2–13
Ekeh AP, Walusimbi M, Brigham E et al (2010) The prevalence of incidental findings on abdominal computed tomography scans of trauma patients. J Emerg Med 38:484–489
Phillips GS, Parisi MT, Chew FX (2011) Imaging diagnosis of right lower quadrant pain in children. AJR Am J Roentgenol 196:W527–534
Purysko AS, Remer EM, Filho HM et al (2011) Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. Radiographics 31:927–947
Klein MD (2007) Clinical approach to a child with abdominal pain who might have appendicitis. Pediatr Radiol 37:11–14
Sivit CJ, Applegate KE (2003) Imaging of acute appendicitis in children. Semin Ultrasound CT MR 24:74–78
Sivit CJ, Applegate KE, Myers MT et al (2000) Evaluation of suspected appendicitis in children and young adults: helical CT. Radiology 216:430–433
Federle MP (1997) Focused appendix CT technique: a commentary. Radiology 202:20–21
Fefferman NR, Roche KJ, Pinkney LP et al (2001) Suspected appendicitis in children: focused CT technique for evaluation. Radiology 220:691–695
Ashraf K, Ashraf O, Bari V et al (2006) Role of focused appendiceal computed tomography in clinically equivocal acute appendicitis. J Pak Med Assoc 56:200–203
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Halverson, M., Delgado, J. & Mahboubi, S. Extra-appendiceal findings in pediatric abdominal CT for suspected appendicitis. Pediatr Radiol 44, 816–820 (2014). https://doi.org/10.1007/s00247-014-2894-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-014-2894-3