
Abstract
Advances in US like high-resolution transducers, harmonic imaging and panoramic modality have overcome some of the obstacles for sonography of the small and large bowel that existed in the past. In a number of centers, bowel US is an established routine method both in adults in children. Bowel US has the distinct advantages of being widely available, relatively cheap, free of radiation and easy to perform. In addition, US of the bowel demonstrates both mural and extramural pathological changes. Patients with inflammatory bowel disease have frequent imaging studies due to disease recurrences and need of follow-up after treatment. Thus this group of pediatric patients benefits most from an optimized and standardized bowel US. This review provides a comprehensive step-by-step approach how to perform US of the bowel in children with emphasis on imaging inflammatory bowel changes. It is meant to serve like a recipe and facilitate the routine performance of US of the bowel in children.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Transabdominal US is currently a well-established method for the evaluation of the small and large bowel [1]. The traditional imaging modalities of the bowel, contrast fluoroscopic studies, are facing competition from or some are being replaced by US of the bowel [2–4]. Advances in US like high-resolution transducers, harmonic imaging, panoramic modality and contrast-enhanced US have overcome some of the obstacles in bowel sonography that existed in the past. Despite these facts the routine use of US of the small and large bowel in children has significant geographic variations, particularly when looking beyond the evaluation of the appendix. It appears to be more commonly integrated as part of the pediatric bowel imaging work-up in Europe and Canada than in the USA.
A very important application of US of the bowel in children is in the evaluation of inflammatory bowel disease (IBD), particularly Crohn disease. In this group of pediatric patients comparative studies of US of the bowel and ileocolonoscopy and histology have demonstrated the range of sensitivity and specificity to be 74–88% and 78–93%, respectively [5–8]. The combined finding of positive blood work-up and bowel wall thickening on US was found to have a positive predictive value of 99.5% in children suspected of having IBD [9]. In the last 2 years at the Children’s Hospital in Philadelphia bowel US has been increasingly integrated in the imaging work-up of children with IBD. The objective of this review is to provide, based on our experience, a comprehensive step-by-step approach how to perform US of the bowel in children and adolescents with emphasis on imaging inflammatory bowel changes. It is meant to serve like a recipe and facilitate the routine performance of bowel US in the pediatric age group.
Step-by-step approach to performing US of the bowel
A. Preparation
Basically US of the bowel can be conducted without any kind of preparation. It is known that significant gaseous distention of the bowel can be an impediment to bowel US. Lack of even very small amount of fluid in the intestine leads to completely collapsed bowel loops and reduction in peristalsis. The intake of carbonated fluid or very long duration of fasting can lead to such states [10]. Particularly, in such cases the following preparatory step may turn out to be helpful. The oral intake of non-carbonated fluid about 30 min before the US examination may be helpful to reduce the air and also slightly distend the bowel loops. Placing the child in a right lateral decubitus position will hasten the emptying of the fluid from the stomach. A partially filled bladder will assist in the evaluation of the distal sigmoid colon and rectum [11].
B. Selection of US modalities
The appropriate selection of transducers and modalities will lead to optimal results of the bowel US. After initial trial of various settings a default setting for bowel US needs to be saved for further use. For ease of annotation, where possible, the following labels should also be saved in full or abbreviated: duodenum—DUO, jejunum—JEJ, ileum—IL, terminal ileum—TI, ileocecal valve—ICV, cecum—CEC, ascending colon—AC, hepatic flexure—HF, transverse colon—TC, splenic flexure—SF, descending colon—DC, sigmoid colon—SC, rectum—REC, right upper quadrant—RUQ, right lower quadrant—RLQ, left upper quadrant—LUQ, left lower quadrant—LLQ. Having these annotations allows quick and exact labeling of the image. The body markers are less suitable for exact labeling of the different parts of the bowel. High-frequency, harmonic and panoramic imaging are important US modalities for high-quality imaging of the bowel and can be used in combination or separately.
-
1.
High-frequency imaging: This entails the use of transducers with high frequency [12]. With the advancement of US transducer technology what we regard as high frequency is shifting, too. If 10 years ago a 7.5 MHz transducer was presented as the high-frequency transducer, nowadays many pediatric diagnostic US scanners have transducers that go higher than 15 MHz. It is important to remember the inverse relationship between frequency and penetration depth of the US wave. Thus the right choice of frequency depends on the body habitus of the patient. For practical purposes it is prudent to start with the available highest-frequency transducer for abdominal imaging and switch to lower ones, if sufficient penetration and visualization is not possible. Predominantly linear, but also convex transducers are needed.
-
2.
Harmonic imaging: This is based on the non-linear propagation property of acoustic signal as it travels through the body [13]. Harmonic waves are generated within the tissue and build up with depth to a point of maximal intensity before they decrease due to attenuation. On the contrary, conventional US waves are generated at the surface of the transducer and progressively decrease in intensity as they traverse the body. The harmonic waves are selectively utilized for imaging, eliminating the fundamental frequency. The latter is achieved by high-pass filters or through pulse/phase inversion technique, or both. Harmonic frequencies are higher integer multiples of the transmitted frequency. Some US scanners only use the 2nd harmonic for imaging (narrow band), whereas others are capable of implementing a wider range of harmonics (wide band). There is image-quality difference between these two modalities, in general the wide band harmonics modality is of better quality. Harmonic imaging improves axial resolution due to shorter wavelength and lateral resolution through better focusing with higher frequencies. As the harmonic waves are produced beyond the body wall the defocusing effect of the body wall is reduced. The relatively small amplitude of the harmonic waves results in artifact reduction. In addition, side lobes are less likely to occur and degrade the image. Artifact-free, clear images with higher contrast and spatial resolution are the result. The advantage and superiority of harmonic imaging compared to conventional US for the bowel has been demonstrated in both adults and children (Fig. 1) [14, 15].
Fig. 1 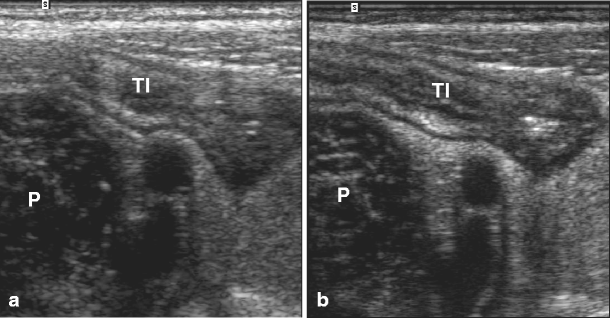
Transverse scan of the right lower quadrant of the abdomen depicting the psoas muscle (P) and iliac vessels in conventional mode (a) and wide band harmonic imaging (b). Note the terminal ileum (TI) anteriorly. The image with harmonic modality is clearer and the terminal ileum and surrounding structures are better demarcated and much more conspicuously visible
-
3.
Panoramic imaging: The bowel is a long convoluted structure. The depiction of a longer segment of the bowel by conventional US is limited. To overcome this limitation and to allow documentation of a bowel loop longer than the length of the transducer one can attempt to use a low-frequency curved-array transducer or dual display mode. These are by far less optimal than panoramic or extended field-of-view imaging [16–18]. Panoramic imaging involves acquiring multiples of successive US images. With the advanced computational capabilities of US scanners ultrafast motion detection and image processing is possible in real-time. Up to a length of 60 cm can be scanned at one time (Fig. 2). It is possible to follow the course of the bowel and make correct length measurements. Moreover, we can use smaller window to evaluate short segments within the scanned bowel.
Fig. 2 
Transverse scan in panoramic modality across the right and left lower quadrants of the abdomen. The right and also the left psoas muscles along with the iliac arteries (IA) and veins (IV) are depicted on one image. The terminal ileum (TI) and cecum (CE) on the right and the sigmoid (S) and descending colons (DC) on the left are visualized on the same image. Note the bowel wall and mesenteric thickening in this child with inflammatory bowel disease


C. Method of scanning
US of the bowel is conducted with the child in supine position. It is easier for the manual handling if the child is lying closer to the edge of the table nearer to the examiner.
-
1.
Compression techniques: The most important technique to use is graded compression. Non-performance of this maneuver is probably the most frequent reason for suboptimal US images of the bowel. Graded compression is not a technique reserved only for appendix imaging, it is also important for the rest of the bowel. It is prudent in older children to inform them that you are going to compress the abdomen and intermittently look at their facial expression to gauge the pressure exerted. Graded compression displaces disturbing air and adjacent bowel loops, shortens the distance for visualization and isolates the bowel loop of interest. An inflamed bowel is non-compressible in contrast to a normal bowel loop. An additional less known maneuver, but one that we have successfully applied is the adjuvant use of a posterior manual compression technique in combination with the graded compression [19]. The hand not holding the transducer is placed under the back. The back is pushed anteriorly at the same time the graded compression is done in the posterior direction (Fig. 3). This technique compounds the effects of the graded compression. It is most useful for depicting the terminal ileum, ileocecal valves and cecum.
Fig. 3 
The technique of graded compression sonography with adjuvant use of a posterior manual compression technique is demonstrated here for the evaluation of the right lower quadrant. An improvement in visualization of the terminal ileum, ileocecal valves and cecum may be achieved
-
2.
Scan planes: Each bowel segment is documented in both the transverse and longitudinal planes. Two planes are more important as it allows a better overview of the mesentery.
-
3.
Doppler US: The bowel wall and mesentery do not normally demonstrate significant color signals on power or color Doppler. In contrast an inflamed bowel loop or mesentery can have increased color signals (Fig. 4). Thus whenever abnormal bowel wall or mesentery is visualized color or power Doppler examination needs to done. The color Doppler is more commonly used than the power Doppler as it is less sensitive to motion, both from bowel peristalsis and patient movement. The setting of the Doppler has to be very low in order to capture small increase in hyperemia. Color Doppler US is useful for follow-up as it may be the first sign to change prior to significant reduction in bowel wall thickness [6, 20, 21]. Some US scanners have the option of color panoramic modality, too.
Fig. 4 
Color Doppler US of the bowel in a child with Crohn disease. The rectal wall is not only thickened (a) but demonstrates marked hyperemia (b). The terminal ileum and mesentery in transverse (c) and longitudinal (d) planes show bowel wall thickening and hyperemia inclusive of the mesentery. The pattern of the hyperemia of the mesentery in the longitudinal plane [d] is compatible with the so-called comb sign arrow
-
4.
US clip: The documentation of the presence, absence or relative decrease of peristalsis is done with a short clip. The respective bowel is isolated and the transducer fixed without movement of the hand. An inflamed bowel shows reduced or no peristalsis compared to a normal one.
-
5.
Measurements: If an inflamed loop is detected, two measurements need to be carried out (Fig. 5). The bowel wall thickness is measured from the hyperechogenic mucosal to the hyperechogenic serosal interfaces. A 3-mm cut-off for normal bowel wall thickness is generally applicable [6, 11]. Specifically for inflammatory bowel disease in the pediatric age group a thickness for the small and large bowels of greater than 2.5 and 2.9 mm, respectively, are regarded as abnormal [7]. The length of an inflamed bowel segment is best measured using panoramic imaging. Some scanners provide the additional feature of measurement of curved distances.
Fig. 5 
Measurements in US of the bowel. (a, b) Bowel wall thickness is measured from the hyperechogenic mucosal to the serosal interfaces (b = magnified section in a). The panoramic image (c) allows the exact measurement of the length of the inflamed terminal ileum
-
6.
“Itinerary”: Using a linear transducer we start with the depiction of the psoas muscle and iliac vessels in the right lower quadrant in the axial plane. From this point it is easy to localize the terminal ileum in its longitudinal plane. We follow the terminal ileum to the ileocecal valves. The ileocecal junction is best viewed at a more obliquely angled view (Fig. 6). This is followed by the evaluation of the cecum and ascending colon. These are the bowel loops located most laterally on the right. The transducer is moved along the ascending colon to the hepatic flexure and then turned to the transverse colon. It is important to carefully trace the path of the transverse colon as the stomach and proximal small bowel loops may be easily mistaken for the transverse colon. After that the transducer is moved to the left over the splenic flexure downward tracing the descending colon. This is the bowel loop normally found most laterally on the left. At the distal end of the descending colon the transducer is turned medially to trace the sigmoid colon. The sigmoid colon is depicted in its longitudinal plane over the axial section of the left psoas muscle and iliac vessels. Further tracing of the large bowel to the rectum with a linear transducer may be difficult. Prior to switching to a convex transducer we go on to evaluate the left upper quadrant, the left lower quadrant, the right upper quadrant and right lower quadrants for the duodenum, jejunum and proximal ileum. After a switch to a convex transducer we continue tracing the remaining sigmoid colon and rectum. The latter is best visualized behind a partially full bladder. It is important to remember that at each step the proper selection of US modality is necessary. Furthermore, at each step the use of graded compression, portrayal in axial and longitudinal planes, color Doppler, clips and measurements whenever appropriate is to be stressed. It is also important to document pathological changes of the mesentery around an inflamed bowel loop. Significant gaseous distention of the bowel and adipose body habitus may hinder depiction of all parts of the bowel. The ease of visualization of pathological findings in the different parts of the bowel is also variable, being more difficult in the more proximal small bowel loops than in the distal ones.
Fig. 6 
The ileocecal junction: the cecum (C) with normal wall thickness but thickened wall of the terminal ileum (TI) and ileocecal valves (ICV) in a child with Crohn disease
Fig. 7 
The terminal ileum scanned with a linear transducer at 14 MHz. All the five layers of the bowel wall are well visualized. A magnified view with labeling of each layer is provided: ❶ HYPERechoic mucosal interface, ❷ HYPOechoic mucosa, ❸ HYPERechoic submucosa, ❹ HYPOechoic muscularis, ❺ HYPERechoic serosal interface





There are currently emerging advanced US modalities in bowel sonography [11]. These new applications are starting to be used primarily in adults, but may have potential benefits in children, too. Hydrosonography is a method in which a contrast liquid with low echogenicity is administered orally or rectally for distending the bowel and improving the scan [22]. The specific study for the small bowel is also known under the name small-intestine-contrast-enhanced US or SICUS. An isotonic polyethylene glycol (PEG) solution is commonly used. In Crohn disease hydrosonography of the small bowel was found to be comparable to ileocolonoscopy, wireless capsule endoscopy, and small-bowel sonography in the assessment of the number, site, extension, and postoperative recurrence of small-bowel lesions [22]. In comparison to conventional US the use of oral contrast agent increased the overall sensitivity from 4% to 11%. In particular, it proved advantageous in depiction of proximal small bowel lesions, from 80% to 100%, and in the evaluation of the number and site of small bowel stenoses, increasing the detection by 11–22% [22]. It is important to realize that when we do bowel US without any bowel preparation as described previously that we are doing so with some degree of limitation. Further advanced application includes contrast-enhanced US with intravenous administration of US contrast agent for better evaluation of the blood flow to the bowel wall. US elastography or strain imagings are US applications for detecting the elasticity or stiffness of a tissue and providing a visual display. Endoscopic sonography using miniprobes is another new application.
D. Reporting findings
A prepared reporting form or a macro for dictation is helpful to standardize the reporting and provide the referring clinician with clear and consistent sonographic information. Such reporting also makes the follow-up evaluation easier. A sample of a form for reporting has been provided in Table 1. The following sample macro of a normal bowel US finding can serve as the basis for reporting the results and be modified accordingly.
REPORT:
US of the small and large bowel
HISTORY: Rule out inflammatory bowel disease
COMPARISON: None
TECHNIQUE: US study targeting only the small and large bowel loops. High-resolution US imaging combined with color Doppler.
FINDINGS: An adequate evaluation of the small and large bowel loops could be carried out. The small bowel loops—duodenum, jejunum and ileum—were visualized. There was no abnormal wall thickening or pathological color Doppler finding. Specifically, the terminal ileum was depicted and traced to the ileocecal valves. The terminal ileum also has normal bowel thickness and there is no increase in color Doppler signal. The large bowel loops—cecum, ascending colon, transverse colon, descending colon, sigmoid colon and rectum—were visualized. They did not show any evidence of abnormal wall thickening or pathological color Doppler finding. In addition, the mesenteric echogenicity was normal and there was no mesenteric thickening and hyperemia. There is normal peristalsis. No free fluid is detected.
IMPRESSION: Normal US of the small and large bowel without evidence of inflammatory bowel disease.
Sonographic finding of the normal and abnormal bowel
High-resolution US can demonstrate the multiple layers of the bowel wall (Fig. 7) [5, 7, 10, 11]. The innermost hyperechoic line corresponds to the mucosal interface with the lumen. The mucosa itself is hypoechoic and this is followed by the hyperechoic submucosa and hypoechoic muscularis. The outermost layer is hyperechoic and represents an interface echo between the surrounding structures and the serosa. We speak in US of normal stratification of the bowel wall if five layers are visible and of loss of stratification if one or more US layers are missing [10]. The jejunum demonstrates more folds and peristalsis than the ileum. The colon displays even less peristalsis and more air-filling. If the bowel loop contains gas, only the front wall may be visible while the rear wall is concealed by the shadow cone and by the gas generated reverberation artifacts.
There are a number of reports describing in detail the various sonographic findings of inflamed bowel in children [6, 11]. In the following only a summary of the findings is given. The pathological changes of the inflamed bowel can be generally divided into mural and extramural findings. The mural findings comprise the changes of the bowel wall. The bowel wall may be thickened, the echogenicity altered to be hypo- or hyperechogenic, there may be variable increases in color Doppler signals denoting bowel hyperemia, loss of the normally visible stratification of the bowel layers, relative decrease or absence in peristalsis signifying some degree of stiffness, ulceration (focal disappearance of the wall stratification) [23], disruption, phlegmon or abscess in the wall and stenosis (Fig. 8). Presence of extramural findings points to a relatively advanced state of the inflammatory bowel disease. Extramural findings comprise mesenteric changes that include an increase in echogenicity combined with thickening resulting in increased separation of the bowel loops. The increased thickening is also known as fibrofatty infiltration or creeping fat. In color Doppler increased flow in the mesentery can be demonstrated and this can have in relation to the bowel wall a specific pattern giving rise to what is known as a comb sign. In the presence of such mesenteric changes one has to be on the lookout for fistulas (Fig. 9). These can me internal fistulas i.e. enteroenteric and enteromesenteric, or external ones like enterocutaneous, enterovesical or enterovaginal. Perineal fistulas are usually difficult to depict on transabdominal US. Lymphadenopathy is another extramural finding that is difficult to relate to the existing inflammatory bowel disease unless there is significant increase in number and size of the lymph nodes, which demonstrates hyperemia on color Doppler. Inflammatory bowel conglomerates and abscesses can also be visualized. The reproducibility of bowel US in the evaluation of Crohn disease has been demonstrated [24].

Pathological US mural findings in Crohn disease. (a) polypoid type of bowel wall thickening, (b) marked bowel bowel thickening and increase in echogenicity with complete loss of stratification, (c) focal intramural disruption of the bowel wall, an ulceration and (d) focal complete disruption of the bowel wall with inflammatory extension into the mesentery (arrow). Note the dot-like echogenic band representing air bubbles in the wall (arrowhead)

Pathological US extramural finding in Crohn disease. Bowel loops with thickened bowel wall surrounded by markedly thickened and echogenic mesentery (M). Note the enteroenteric fistula (arrows)
A comprehensive step-by-step approach to performing US of the bowel in children has been presented. The illustrations will help to reinforce what findings to expect. These should serve as a recipe for introducing US of the bowel in the routine bowel imaging in the pediatric age group.
References
Maconi G, Bianci P (eds) (2007) Ultrasound of the gastrointestinal tract. Medical Radiology. Diagnostic Imaging Series. Springer-Verlag, Heidelberg
Anupindi SA, Darge K (2009) Imaging choices in inflammatory bowel disease. Pediatr Radiol 39(Suppl2):S149–S152
Hiorns MP (2008) Imaging of inflammatory bowel disease. How? Pediatr Radiol 38(Suppl 3):S512–S517
Mann EH (2008) Inflammatory bowel disease: imaging of the pediatric patient. Semin Roentgenol 43:29–38
Epifanio M, Baldisserotto M, Spolidoro JV et al (2008) Grey-scale and colour Doppler sonography in the evaluation of children with suspected bowel inflammation: correlation with colonoscopy and histological findings. Clin Radiol 63:968–978
Alison M, Kheniche A, Azoulay R et al (2007) Ultrasonography of Crohn disease in children. Pediatr Radiol 37:1071–1082
Bremner AR, Griffiths M, Argent JD et al (2006) Sonographic evaluation of inflammatory bowel disease: a prospective, blinded comparative study. Pediatr Radiol 36:947–953
Fraquelli M, Colli A, Casazza G et al (2005) Role of US in detection of Crohn disease: meta-analysis. Radiology 236:95–101
Canani RB, de Horatio LT, Terrin G et al (2006) Combined use of noninvasive tests is useful in the initial diagnostic approach to a child with suspected inflammatory bowel disease. J Pediatr Gastroenterol Nutr 42:9–15
Nylund K, Odegaard S, Hausken T et al (2009) Sonography of the small intestine. World J Gastroenterol 15:1319–1330
Cammarota T, Sarno A, Robotti D et al (2008) Us evaluation of patients affected by IBD: how to do it, methods and findings. Eur J Radiol 69:429–437
Riccabona M (2006) Modern pediatric ultrasound: potential applications and clinical significance. A review. Clin Imaging 30:77–86
Tranquart F, Grenier N, Eder V et al (1999) Clinical use of ultrasound tissue harmonic imaging. Ultrasound Med Biol 25:889–894
Schmidt T, Hohl C, Haage P et al (2005) Phase-inversion tissue harmonic imaging compared to fundamental B-mode ultrasound in the evaluation of the pathology of large and small bowel. Eur Radiol 15:2021–2030
Rompel O, Huelsse B, Bodenschatz K et al (2006) Harmonic US imaging of appendicitis in children. Pediatr Radiol 12:1257–1264
Turgut AT, Cos ZU, Kısmet K et al (2008) Comparison of extended field of view and dual image ultrasound techniques for the measurement of the longitudinal dimension of enlarged thyroid glands. J Med Ultrasound 16:150–157
Ying M, Sin MH (2005) Comparison of extended field of view and dual image ultrasound techniques: accuracy and reliability of distance measurements in phantom study. Ultrasound Med Biol 31:79–83
Tröger J, Darge K (1998) SieScape - a new dimension of ultrasound imaging in pediatric radiology. Radiologe 38:417–419
Lee JH, Jeong YK, Hwang JC et al (2002) Graded compression sonography with adjuvant use of a posterior manual compression technique in the sonographic diagnosis of acute appendicitis. AJR 178:863–866
Drews BH, Barth TFE, Haenle MM et al (2009) Comparison of sonographically measured bowel wall vascularity, histology, and disease activity in Crohn’s disease. Eur Radiol 19:1379–1386
Ripolles T, Martinex MJ, Barrachina MM (2008) Crohn’s disease and color Doppler sonography: response to treatment and its relationship with long-term prognosis. J Clin Ultrasound 36:267–272
Maconi G, Radice E, Bareggi E et al (2009) Hydrosonography of the gastrointestinal tract. AJR 193:700–708
Kunihiro K, Hata J, Haruma K et al (2004) Sonographic detection of longitudinal ulcers in Crohn disease. Scand J Gastroenterol 39:322–326
Fraquelli M, Sarno A, Girelli C et al (2008) Reproducibility of bowel ultrasonography in the evalutation of Crohn’s disease. Dig Liver Dis 40:860–866
Author information
Authors and Affiliations
Corresponding author
Additional information
Dr. Darge has indicated that he has no relevant financial relationships or potential conflicts of interest related to the material presented.
Rights and permissions
About this article
Cite this article
Darge, K., Anupindi, S., Keener, H. et al. Ultrasound of the bowel in children: how we do it. Pediatr Radiol 40, 528–536 (2010). https://doi.org/10.1007/s00247-010-1550-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-010-1550-9