
Abstract
Background
Recent reports have indicated that infants and young children have a higher sensitivity than older children and adults to radiation exposure and the potential for harmful side effects.
Objective
To determine whether the present landmarks used in film positioning result in unnecessary radiation to non-thoracic structures on chest radiographs in the pediatric and neonatal population.
Materials and methods
Chest radiographs of 195 pediatric patients and 149 neonates were analyzed for extent of radiation field to non-thoracic regions. This was accomplished by delineating the most superior and inferior portions of the body included within the boundaries of collimation on each chest radiograph. The distance between the superior and inferior aspects of the lungs was measured and compared to the long axis of the radiation field on the radiograph. Radiographic reports were reviewed to determine whether valuable data were obtained from the imaging of these non-thoracic structures.
Results
The ratio of radiation exposure to non-thoracic structures increases as the age of the patient decreases. Overall, 43% of the length of the chest radiograph was of non-thoracic structures, resulting in radiation exposure to these sites. No significant information was gained in a single case by including the neck. In 3% of the neonatal patients, a potentially significant comment was reported on the abdomen included on the chest radiograph.
Conclusion
Present positioning techniques in neonatal and pediatric chest radiography result in unnecessary radiation exposure to non-thoracic structures. New landmarks for collimation should be sought to eliminate this problem.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Standard pediatric chest radiographs are performed with the image centered at the nipple line (T6-7), with the collimated field extending from the mastoid tip to just superior to the iliac crest, as described in Merrill's Atlas of Radiographic Positions [1]. This technique can result in unnecessary radiation exposure to non-thoracic structures, most critically in younger children and infants who are at the most significant risk for radiation-induced injury. The purpose of this study was to determine whether the present landmarks used in film positioning result in unnecessary radiation to non-thoracic structures on chest radiographs in the pediatric and neonatal population.
Materials and methods
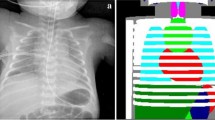
We analyzed 387 chest radiographs (195 AP and 192 lateral) in patients aged from 1 month to 12 years and 252 radiographs (149 AP and 103 lateral) in neonatal patients to determine the extent of the radiation field to non-thoracic regions. This was accomplished by delineating the most superior and inferior portions of the body included within the boundaries of collimation on each chest radiograph. The distance between the superior and inferior aspects of the lungs was measured and compared to the long axis of the radiation field on the radiograph, as illustrated in Fig. 1. This ratio is an index of the efficiency of use of the irradiated field. We documented the cervical spine level for the most superior exposure and compiled the thorax-to-radiation-field ratio and cervical level, along with patient age and film size. Radiologic reports for each examination were reviewed to determine whether any important clinical information was gained by including non-thoracic structures.

Frontal (a) and lateral (b) radiographs depict a method used to determine thorax-to-radiation field ratio as an index of the efficiency of use of the irradiated field. Arrow A indicates the length of the chest included on radiograph. Arrow B indicates the total length of the irradiated field
The radiographs were acquired between September 2001 and March 2004. The neonatal chest radiographs were all performed for assessment of the extent of surfactant deficiency disease and its potential complications. All neonatal images had been obtained with portable radiographic equipment. All radiographs performed on the pediatric population included in this study were for assessment of possible pneumonic infiltrate. Pediatric radiographs had been taken within the diagnostic department of two local hospitals. The project received ethics approval from the board of the hospitals.
Neonates were imaged in a supine position at 58 kVp, 1.2 mAs at 100 cm with no grid. Infants up to 6 months of age were imaged in an AP supine position with a 40-inch ffd at 1.25 mAs at 64 kVp. No grid was used, and exposure factor control was fixed. Patients aged 6 months to 3 years were imaged in an erect AP position with 72-inch ffd with no grid. Exposure factor control was fixed using 1.25 mAs at 90 kVp. Patients older than 3 years at one hospital were imaged using the wall bucky with automatic exposure control at 90 kVp primarily in a PA position, generally without a grid. Patients older than 6 years, at the other hospital, had chest imaging performed with a fixed time technique, with no grid, at 70 kVp and 1.2 mAs and at an approximate distance 60 inches. Film speed was 350 for images obtained in the department and 400 for portable images. The equipment used was GE Advantix or MXP (Milwaukee, Wis.) in the department and AMX4 (GE) portable system.
Results
Table 1 compares the ratio of long axis of the lungs to the radiation field for chest radiographs performed on our patient population.
A trend toward an increased ratio of the long axis of the lungs to the radiation field was evident with increasing film size. ANOVA of exposure ratio and film size demonstrated a significant difference between groups for the AP view (P=0.002) but not for the lateral view (P=0.206). The post-hoc test (Tukey's) revealed that neonates (25×20 cm film size) were almost identical (P=0.971) to non-neonates (25×20 cm film size). Neonates had the lowest ratio of long axis of lung to radiation field on AP studies, with only 55% of the exposed radiographs consisting of lung parenchyma. ANOVA of exposure ratio and age group also demonstrated a highly statistically significant trend (P<0.001): as the age group increased so did the ratio of long axis of lungs to radiation field.
Using the chi-squared test, data from Table 2 reveal a strong trend toward more inferior C-spine level (vertebral bodies 1–7) included in the radiation field with increasing age category (P<0.001). This held true for both the frontal and lateral projections.
On five chest radiographs in the neonate population, a comment was made on the visualized abdomen. Four reports questioned mild bowel dilation, suggesting follow-up radiographs that were subsequently non-specific. In the remaining case, a concern of ascites was raised and subsequent sonographs were performed and found to be normal. In no case was a radiologic finding reported within the neck.
Discussion
Recent reports have suggested that infants and young children have higher sensitivity than older children and adults to radiation exposure and the potential for harmful side effects [2–6]. Although radiographic imaging results in a dose to the individual hundreds of times smaller than CT, the vast number of radiographs obtained results in an increased risk to the population as a whole [7]. Numerous strategies to reduce patient dose have been discussed in the literature. This study focused mainly on the role of collimation in efforts to reduce patient radiation exposure to the lowest achievable level. The role of shielding, mispositioning, grid use and exposure indicator targets as discussed by previous authors [7–9] was not undertaken and is beyond the scope of this study. These factors, which play a major role in patient radiation dose, highlight the technical challenges faced by radiology staff daily.
Present collimation techniques as described by Merrill extend from the tip of the mastoid inferiorly to just above iliac crest [1]. The purpose of using the superior collimation blade level is for evaluation of the upper airway/trachea. On review of 344 patient chest radiographs in our study, there was no useful information gained from inclusion of these more superior extra-thoracic structures. In our neonatal population, 3% of the chest radiographs indicated a potential abnormality in the visualized abdomen. One infant (one of five) subsequently underwent sonography that was unremarkable. The other patients in this group (four of five) received follow-up abdominal radiographs that were non-specific.
Previous researchers have calculated an exposure to the radiation-sensitive thyroid of 6.6 mR from chest radiography of premature infants. In our study, the average superior collimation blade was at C1–2 level, from neonates up to 1 year of age. The thyroid would, therefore, be within the radiation field and at risk. Unfortunately, we did not document the lumbar spine level included in the chest collimation field; however, Merrill's guidelines are to extend the inferior collimator blade to just above iliac crest [1]. This level also results in unnecessary radiation to non-thoracic structures on the chest radiograph. A gonadal dose between 0.038 and 5.9 mRem for boys and 0.091 and 7.9 mRem for girls, also from AP chest radiographs, has been documented in studies by Aspin [11] and Poznanski [10]. It has been suggested that excluding the gonads from the exposure field can decrease the dose to this site by up to 100 times [7].
Our study demonstrates that present film collimation in pediatric chest radiography results in unnecessary radiation exposure to non-thoracic structures, with no significant clinical gain. The present collimation results in the greatest unnecessary radiation exposure to the youngest of patients (neonates), who are at the greatest risk for potential radiation-induced injury [2–5]. These are also the patients who often undergo multiple studies, compounding this risk. Defining new landmarks to use in collimation in pediatric chest radiography is necessary to satisfy the ALARA principle. Easily palpable structures can aid us in this regard. With the arms elevated (i.e., in pigostat), the superior border of the palpable AC joint generally lies above the lung apex. Inferiorly, the ribs of the infant and young child can usually be felt, which might be sufficient for the inferior collimation. Although lung parenchymal infiltrate can potentially be seen at the lung bases through the upper quadrant structures on frontal chest views, infants and young children have a relative decrease in diaphragmatic dome, making this inconsequential. Further studies are necessary to establish new collimation landmarks for pediatric chest radiography.
In conclusion, positioning techniques in neonatal and pediatric chest radiography result in unnecessary radiation exposure to non-thoracic structures. It is clear from previous studies that we should be concerned with the radiation dose to all structures, particularly the thyroid and gonads. Improvement of collimation of chest radiographs would help satisfy the ALARA principle and help eliminate the problem of overexposure.
References
Ballinger PW (2003) Merrill's atlas of radiographic positions and radiologic procedures, vol. 3. Mosby-Year Book, St. Louis, p 190
Don S (2004) Radiosensitivity of children: potential for overexposure in CR and DR and magnitude of doses in ordinary radiographic examinations. Pediatr Radiol 34(Suppl 3):S167–S172
Hall EJ (2002) Lessons we have learned from our children: cancer risks from diagnostic radiology. Pediatr Radiol 32:700–706
Hintenlang K (2002) A survey of radiation dose associated with pediatric plain-film chest X-ray examinations. Pediatr Radiol 32:771–777
Huda W, Slone RM (2003) Review of radiologic physics, 2nd edn. Lippincott Williams and Wilkins, Philadelphia
Ron E (2002) Let's not relive the past: a review of cancer risk after diagnostic or therapeutic irradiation. Pediatr Radiol 32:739–744
Willis CE (2002) Computed radiography: a higher dose? Pediatr Radiol 32:745–750
Willis CE (2004) Strategies for dose reduction in ordinary radiographic examinations using CR and DR. Pediatr Radiol 34(Suppl 3):S196–S200
Singleton EB (1981) Radiologic considerations of intensive care in the premature infant. Radiology 140:291–300
Poznanski AK (1976) Practical approaches to pediatric radiology. Year Book Medical Publishers, Chicago
Aspin N (1965) The gonadal x-ray dose to children from diagnostic radiographic technics. Radiology 85:944–951
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Soboleski, D., Theriault, C., Acker, A. et al. Unnecessary irradiation to non-thoracic structures during pediatric chest radiography. Pediatr Radiol 36, 22–25 (2006). https://doi.org/10.1007/s00247-005-0016-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-005-0016-y