
Abstract
We report on a 4-year-old boy who presented to the ophthalmology department for assessment of convergent strabismus. Ophthalmic examination showed a left morning glory optic disc anomaly and retinal detachment. Plain films obtained for investigation of short stature prior to ophthalmic examination revealed delayed bone age. Ophthalmological findings prompted CT and MRI imaging and angiographic investigations. Midline cranial defects and abnormal carotid circulation were identified. These findings may be associated with morning glory optic disc anomaly, and their association is often under-recognized. It is important that clinicians and radiologists be aware of this spectrum of disorders, as the vascular abnormalities may predispose the patient to transient ischemic attacks and strokes. Growth delay may result from hypopituitarism.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
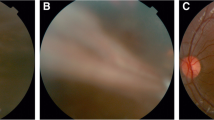
Morning glory disc anomaly is a usually unilateral, congenital funnel-shaped excavation of the posterior fundus that incorporates the optic disc. In this condition the optic disc resembles the morning glory flower, hence the name. Serous retinal detachment can occur in the affected eye (Fig. 1).

Fundus photograph of left eye. a Morning glory disc anomaly with radial pattern of emergence of retinal vessels and retinal detachment. b Scan imaging of retinal detachment associated with optic nerve coloboma.
Case report
A 4-year-old boy who had been recently adopted from an orphanage was found to have left convergent strabismus (inward deviation of the left eye). Ophthalmic examination revealed Snellen visual acuity of 6/6 in the right eye and counting fingers at near in the left eye. He had a left relative afferent pupillary defect (RAPD). Binocular indirect ophthalmoscopy showed morning glory disc anomaly with total serous retinal detachment in the left eye, demonstrated on B scan US examination (Fig. 1). The right eye was normal.
Medical history indicated there was perinatal encephalopathy with associated hypotonia. Moderate delay in psychomotor development and expressive speech development was noted. Neurological assessment did not identify any focal abnormality of the nervous system. There were no obvious dysmorphic features. The boy’s weight was between the 10th and 25th percentiles, and his height was at the third percentile. Parental heights and growth records were unavailable. A significant finding on general examination was bruits over both carotid arteries, which was further investigated by angiography after CT and MRI scan.
Imaging findings
Plain film findings revealed a delayed bone age. CT imaging of the orbits confirmed morning glory disc anomaly and retinal detachment (Fig. 2). Skull-based views on CT demonstrated absence of the left internal carotid artery bony canal, partial absence of the nasal septum and persistence of the sphenopharyngeal foramen (Fig. 2). MR imaging of the orbits showed the deformity of the distal optic nerve and retinal detachment associated with the morning glory disc anomaly (Fig. 3). Sagittal views on MRI demonstrated ectopia of the pituitary gland into the persistent sphenopharyngeal foramen (Fig. 3). MRA and catheter selective angiography confirmed absence of the left internal carotid artery and demonstrated focal stenosis of the right distal internal carotid artery and right middle cerebral artery (Fig. 4). Angiograghic features were classified according to the Suzuki classification as an early stage of moyamoya [1].

CT scan utilizing bone algorithm, a coronal scan shows dilated optic nerve sheath complex (black arrow). Also shown is partial absence of the nasal septum (white arrow). b Axial CT scan demonstrates presence of the right internal carotid artery bony canal (ICA) and absence of the left canal. White arrows are on the right ICA canal and on the expected position of the left ICA canal. Additionally noted is a persistent sphenopharyngeal foramen (black arrow). c Persistent sphenopharyngeal foramen is shown by white arrow on this coronal scan.

Orbital and pituitary abnormalities. a Axial T1-weighted SE (600/20) MRI image of the orbits with fat saturation with contrast administration shows funnel-shaped deformity of the distal optic nerve associated with retinal detachment. b Sagittal T1-weighted MR SE (600/20) shows abnormal axis of the pituitary gland with ectopia of the gland into the persistent sphenopharyngeal foramen (white arrow). The posterior pituitary bright spot is present (black arrow).

MR angiogram. “3D time-of-flight ” demonstrates total lack of flow within the left internal carotid artery (a) (black arrow is on right internal carotid artery). White arrow shows focal stenosis of the proximal right middle cerebral artery. b An oblique view of a select catheter angiogram of right internal carotid artery shows stenosis of the distal internal carotid artery (black arrow). c Select catheter injection of left common carotid artery shows filling of the external carotid artery and its branches. The left internal carotid artery is not seen.
Endocrine assessment
Investigation of the endocrine system at the time of presentation confirmed normal thyroid stimulating hormone, free thyroxin and prolactin levels. An ACTH stimulation test demonstrated normal cortisol response.
Radiograph of the left hand and wrist demonstrated a bone age of 1.5 years, significantly delayed compared to the chronological age of 4 years. Provocative growth hormone (GH) testing demonstrated low GH levels (peak GH <8 mcg/l). The patient spontaneously exhibited improved growth velocity prior to the initiation of growth hormone therapy, so treatment was deferred. After 5 years of follow-up, he continues to demonstrate normal growth velocity without GH therapy and is tracking at the 75th percentile for age.
Discussion
The abnormalities of carotid circulation—which have been described in some patients with morning glory disc anomaly as carotid stenoses or aplasia and in others as progressive vascular obstruction with collateralization (moyamoya)—may lead to ischemia, stroke, and seizures [2–7]. In our patient, there was aplasia or hypoplasia of one carotid artery and its bony canal. Additionally, there were focal stenoses of the distal contralateral internal carotid artery (ICA) and of the contralateral middle cerebral artery. Distal ICA stenosis, prior to the appearance of collateralization, is considered to be an early stage of moyamoya [1]. Our patient has had no symptoms related to vascular insufficiency, but follow-up MRA is planned to evaluate for progressive vascular changes.
This case demonstrates the association between morning glory disc anomaly, midline cranial defects and abnormal carotid circulation. Patients with this spectrum of disorder might suffer from transient ischemic attacks or seizures caused by carotid insufficiency [2, 5]. Endocrinological abnormalities such as hypopituitarism can also occur and present as delayed bone age and reduced growth [5].
In this patient the short stature, significantly delayed bone age, morning glory anomaly and abnormal pituitary morphology on MRI led to growth hormone testing. Although this patient tested low by provocative GH testing, he exhibited spontaneous catch-up growth that coincided with an improved socioeconomic environment. Thus, in this case, it is likely his initial poor growth and low GH testing was a function of a poor nutritional and social situation and was not reflective of hypopituitarism. Nonetheless, the clinician and radiologist should be aware of the spectrum of endocrine and developmental anomalies associated with morning glory disc and assess the patient accordingly.
References
Suzuki J, Takaku A, Kodama N, et al (1975) An attempt to treat cerebrovascular ’moyamoya’ disease in children. Child’s Brain 1:193–206
Bakri SJ, Siker D, Masaryk T, et al (1999) Ocular malformations, moyamoya disease, and midline cranial defects: a distinct syndrome. Am J Ophthalmol 127:356–357
Goldhammer Y, Smith JL (1975) Optic nerve anomalies in basal encephalocele. Arch Ophthalmol 93:115–118
Hanson MR, Price RL, Rothner AD, et al (1985) Developmental anomalies of the optic disc and carotid circulation—a new association. J Clin Neuro-ophthalmol 5:3–8
Komiyama M, Yasui T, Sakamoto H, et al (2000) Basal meningoencephalocele, anomaly of optic disc and panhypopituitarism in association with moyamoya disease. Pediatr Neurosurg 33:100–104
Krishnan C, Roy A, Traboulsi E (2000) Morning glory disk anomaly, choroidal coloboma, and congenital constrictive malformations of the internal carotid arteries (moyamoya disease). Ophthalmic Genet 21:21–24
Massaro M, Thorarensen O, Liu GT, et al (1998) Morning glory disc anomaly and moyamoya vessels. Arch Ophthalmol 116:253–254
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Quah, B.L., Hamilton, J., Blaser, S. et al. Morning glory disc anomaly, midline cranial defects and abnormal carotid circulation: an association worth looking for. Pediatr Radiol 35, 525–528 (2005). https://doi.org/10.1007/s00247-004-1345-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-004-1345-y