
Abstract
Hypertrophic osteoarthropathy is a well-documented paraneoplastic phenomenon in adults. It is a rare, but important finding in children with malignant disease as it can indicate prognosis. We present a case of hypertrophic osteoarthropathy associated with primary liver rhabdomyosarcoma in a 14-year-old boy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hypertrophic osteoarthropathy (HOA) is usually encountered in adults, being a rare finding in children. A primary form exists, which has autosomal dominant inheritance. Secondary HOA has numerous associations. Classically, it is considered a paraneoplastic phenomenon with tumours being the cause of over 90% of cases in adults. Non-neoplastic causes of secondary HOA include cystic fibrosis, congenital heart disease, liver disease, biliary atresia and inflammatory bowel disease. It is characterised by nail clubbing, arthritis and periosteal new bone formation of the limbs, which may be painful. First described by Bamberger in 1889 [1], and Marie in 1890 [2], most cases are associated with intrathoracic lesions [3]. The underlying mechanism of pathogenesis has yet to be elaborated.
Neoplasia is an unusual cause of HOA in children, accounting for 12% of cases [3]. We report a 14-year-old boy with primary liver rhabdomyosarcoma (RMS) and secondary HOA.
Case report
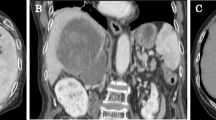
A 14-year-old Caucasian boy was admitted to hospital with a 5-week history of lethargy, fever, pallor and abdominal pain. On examination, he looked pale and tired. He was tachypnoeic, tachycardic and hypoxic. Blood indices showed iron-deficiency anaemia. Abdominal US showed a large solitary intrahepatic mass in the right lobe of the liver with echo-free spaces. CT showed a generally hypodense lesion with strand-like enhancement. MRI of the lesion showed high signal intensity with heterogeneous enhancement (Fig. 1). The left lobe of the liver appeared normal. Percutaneous biopsy confirmed the diagnosis of RMS.

T2-weighted single-shot fast spin-echo axial MRI showing the tumour in the right lobe of the liver
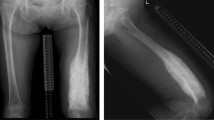
The patient developed long bone and back pain. A radionuclide bone scan showed unusual symmetrical uptake in the distal humeri, radii and ulnae, as well as the tibiae and fibulae (Fig. 2). MRI of the long bones showed diffuse periosteal high signal around the shafts of the long bones, but with normal bone marrow signal. Plain radiographs confirmed HOA (Fig. 3).

Radionuclide bone scan showing increased uptake in the peripheral skeleton (arrows)

Detail of lateral radiograph of the left tibia and fibula showing hypertrophic osteoarthropathy
The patient is currently undergoing systemic chemotherapy with carboplatin, etoposide and vincristine (CEV) therapy and is being considered for tumour resection.
Discussion
Most cases of HOA in children are associated with benign conditions, such as cystic fibrosis and congenital heart disease. In 1990, Staalman and Umans [3] reviewed 25 cases of HOA as a paraneoplastic phenomenon in children. There was 80% male preponderance, and only 8% of patients were less than 10 years of age. Most of the children were known to have primary malignancy (almost 50% had cancer of the nasopharynx), but the appearance of HOA heralded the discovery of recurrence or metastasis in 15 of the 25 patients. In 80% of the patients, pathological changes, such as lymph node involvement or pulmonary metastases, were visible on chest radiographs.
Conclusions
Both primary liver RMS and HOA with malignancy are rare occurrences in childhood. None of the previous reported cases associated HOA with RMS.
References
von Bamberger E (1889) Veränderungen der Röhrenknochen bei bronchiektasie. Wien Klin Wochenschr 2:226
Marie P (1890) De l’osteo-arthropathie hypertrophiante pneumique. Rev Med Paris 10:1–36
Staalman CR, Umans U (1993) Hypertrophic osteoarthropathy in childhood malignancy. Med Pediatr Oncol 21:676–679
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Geary, T.R., Maclennan, A.C. & Irwin, G.J. Hypertrophic osteoarthropathy in primary liver rhabdomyosarcoma. Pediatr Radiol 34, 250–252 (2004). https://doi.org/10.1007/s00247-003-1000-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-003-1000-z