
Abstract
In order to evaluate physicians’ willingness to seek legal action to mandate surgery when parents refuse surgery for various congenital heart lesions, we surveyed pediatric cardiologists and cardiovascular surgeons at 4 children’s hospitals. We asked whether physicians would support parental refusal of surgery for specific heart defects and, if not, whether they would seek legal action to mandate surgery. We then analyzed associations between physicians’ willingness to mandate surgery and national operative mortality rates for each lesion. We surveyed 126 cardiologists and 9 cardiac surgeons at four tertiary referral centers. Overall response rate was 77%. Greater than 70% of physicians would seek legal action and mandate surgery for the following lesions: ventricular septal defect, coarctation of the aorta, complete atrioventricular canal, transposition of the great arteries, tetralogy of Fallot, and unobstructed total anomalous pulmonary venous return. Surgery for all of these lesions has reported mortality rates of < 5%. Physicians were less likely to seek legal action when parents refused surgery for Shone complex, any single ventricle lesion, or any congenital heart disease accompanied by Trisomy 13 or Trisomy 18. Among experts in pediatric cardiology, there is widespread agreement about the appropriate response to parental refusal of surgery for most congenital heart lesions, and these lesions tended to be heart defects with lower surgical mortality rates. Lesions for which there was greater consensus among experts were those with the best outcomes. There was less consensus for lesions with higher mortality rates. Such surveys, revealing disagreement among expert professionals, can provide an operational definition of the current professional “gray zone” in which parental preferences should determine treatment.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Over the last 40 years, survival for children with congenital heart disease (CHD) has improved significantly due to strides in diagnosis, medical management, and surgical technique and the standard of care for most critical CHD is surgical repair in the neonatal period [1]. Decisions regarding the acceptability of comfort care for CHD require interpretation of limited data regarding short- and long-term mortality and morbidities of various forms of CHD and consideration of the severity of associated anomalies. It may also require balancing what is thought best for the child including effects of treatment on families. Balancing all of these considerations leads different doctors to different conclusions [2,3,4,5,6,7,8].
Doctors sometimes disagree with each other about the acceptability of parental refusals of potentially life-saving interventions [9]. For example, in children with hypoplastic left heart syndrome, one doctor wrote “palliative treatment is a reasonable choice for an infant with HLHS [2]” while another is of the opinion that “nonintervention should no longer be offered” [3].
Pediatric cardiologists and cardiothoracic surgeons, like all child health professionals, have an ethical obligation to do what is best for the children in their care. In some situations, this requires doctors to seek legal intervention to override a parent’s refusal of a treatment that the doctor believes is medically necessary. It is not always clear whether parental refusal of a medically recommended treatment should be considered neglect or when, by contrast, it should be considered an appropriate exercise of parental decision-making. Ultimately, that determination is up to the courts. But courts can only adjudicate cases if doctors report them.
Most pediatric cardiology centers have no established policies about when to allow parental preferences to prevail and when to report cases to child protection. Thus, individual specialists are left to decide when to offer the option of comfort care to parents or to accept parental requests for such care. There are little data on opinions of pediatric cardiologists and congenital cardiothoracic surgeons regarding the acceptability of comfort care for a wide range of CHD, and there are no data comparing specialists’ attitudes with likelihood of reported surgical mortality.
Therefore, we aimed to (1) describe the opinion of pediatric cardiologists and congenital cardiothoracic surgeons from various institutions about overriding parental refusal of surgery for various types of CHD; and (2) compare these results to nationally reported neonatal surgical mortality rates. We hypothesized that cardiologists and surgeons would generally agree in the cases of the lowest risk lesions, and that agreement would be lower for higher risk lesions.
Methods
Pediatric cardiologists and cardiothoracic surgeons were surveyed at four tertiary care children’s hospitals between 2016 and 2018. Only limited demographic (cardiologist/surgeon) information was elicited to maintain anonymity. The survey asked participants to rate their level of comfort in supporting comfort care for various specific CHDs. Cardiac lesions were stated to be isolated lesions unless otherwise specified. Physicians were given four choices: (1) Agree and I would support parents who choose to not pursue surgical intervention; (2) Disagree but I could still support parents who choose not to purse surgical intervention; (3) Disagree, would not support parents who choose not to purse surgical intervention, but would not interfere with the decision; and, (4) Disagree, completely opposed to parents who choose not to pursue surgical intervention, seek legal action to remove child from parental custody to pursue surgery. For sub-analysis, responses 1–3 were combined as “would not go to court”. Chi-square or Fischer’s exact tests were used, as appropriate, to compare each outcome between the four institutions.
Surgical mortality data were gathered from the Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database Executive Summary for January 2014 to December 2017 [10]. When considering CAVC, a different STS data publication was used to differentiate expected mortality for children with and without trisomy 21 [11]. Mortality data for the most common surgical repair for each CHD were used, and data reported are post-surgical mortality until discharge from the hospital or up to 28 days post-operative. Spearman’s correlation coefficient was calculated to determine correlation between threshold to seek legal action and short-term surgical mortality rate for each cardiac lesion. This survey was approved by all centers’ institutional review boards.
Results
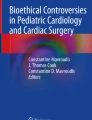
Descriptors of the survey participants are recorded in Table 1 with a response rate of 77% (135/176). Table 2 shows physician level of comfort in supporting parental choice. Table 3 contains the STS mortality rate for each CHD and the percent of physicians surveyed who would pursue legal action to mandate surgery overall and by each institution. No statistically significant differences in responses were found for any lesion when comparing the 4 institutions overall. Figure 1 shows a scatter plot with a regression line to demonstrate the strength of correlation between surgical mortality and physician willingness to go to court.

Likelihood physicians would seek legal action to mandate surgery for CHD compared to surgical mortality. Data displayed are for 15 lesions represented in Table 2 with mortality data
Most physicians would seek protective custody if parents refused surgery for most lesions with an anticipated surgical mortality of less than 4.5%, as in cases with a ventricular septal defect, coarctation of the aorta, compete atrioventricular canal defect (not associated with Trisomy 21), tetralogy of Fallot, transposition of the great arteries, and interrupted aortic arch. When mortality rates are higher, as in cases of HLHS with a published mortality rate of 14.4%, few physicians would seek legal action to mandate surgery. Doctors were also influenced in their decisions by the presence of associated genetic abnormalities. 84% of respondents would seek a court order mandating surgery in a child with CAVC and no genetic abnormality while only 54% of physicians would mandate surgery for a child with CAVC and trisomy 21. This is despite a CAVC surgical mortality rate that is actually lower for children with trisomy 21 (4.4% mortality for CAVC with no genetic abnormality versus 2.6% for CAVC with trisomy 21) [10].
Discussion
This is an exploratory survey-based study to evaluate physician opinion towards supporting parental refusal for cardiac surgery. There is generally professional consensus for the vast majority of CHDs. Consensus lessens for lesions associated with higher mortality risk. At the highest mortality categories, most pediatric cardiology specialists consider comfort care to be an acceptable management option. This includes neonates with any form of single ventricle physiology, forms of CHD with low likelihood of survival through infancy, and for CHD in a child with a severe genetic syndrome. Doctors’ willingness to pursue legal action generally increased as the child’s chances of operative survival increased.
This study revealed that most doctors would not go to court to override parental refusal of surgery for HLHS despite short-term survival of up to 85% at some institutions. This may be because the short-term surgical mortality rate captures survival only through the first heart surgery. Children with HLHS require two subsequent open-heart surgeries over the first few years of life, are at risk of neurodevelopmental delay, may need multiple non-surgical interventions and hospitalizations, and possibly heart transplantation [12,13,14,15]. Physician support for comfort care in HLHS may highlight the influence of overall long-term burden of medical treatment and anticipated quality of life on decision-making.
Cardiology specialists may also consider whether comfort care is predicted to be associated with a relatively quick neonatal death. In the setting of ductal-dependent pulmonary or systemic circulations, non-intervention usually results in death within days after birth. However, many CHD circulations do not require the ductus arteriosus for survival, as in the case of a complete atrioventricular canal defect. Forgoing surgery for children with these forms of CHD results in profound and progressive cardiac symptoms, irreversible pulmonary vascular disease, medical frailty, physical limitations during childhood, and likely demise before adulthood. This may explain why physicians in the survey were more likely to support comfort care for a child with obstructed total anomalous pulmonary venous return (TAPVR) compared to children with unobstructed TAPVR; TAPVR obstruction is more likely to result in neonatal death. Physicians may also be more likely to assent to parental desire for comfort care when the outcome has more uncertainty, as in the case of Shone’s syndrome. Thus, physicians may be more likely to disagree with parental desire for comfort care and pursue legal action in cases in which the outcome is almost universally favorable with intervention, or when non-intervention would result in undue and prolonged suffering for the child.
Genetic abnormalities also influence physicians’ attitudes; physicians typically factor in comorbidities associated with trisomy 21 and other genetic syndromes when counseling families about treatment. The importance of an associated genetic syndrome may also factor into responses for interrupted aortic arch. Surgical outcomes for this lesion are quite favorable and compare to those of isolated coarctation of the aorta. However, respondents were more likely to support comfort care in this lesion compared to coarctation. This may be due to the well-known association between interrupted aortic arch and 22q11 deletion syndrome, a genetic condition with a variable phenotype which can include developmental delay, learning problems, frequent infections, renal abnormalities, hearing loss, and autoimmune disorders [16].
Limitations of the study include that this is a descriptive study of four institutions and not powered to detect statistically significant differences. Other institutions may have different approaches. We utilized the STS Database because the majority of US institutions submit their cardiothoracic surgical post-operative mortality statistics; however, it does not include data on patient characteristics or long-term mortality and morbidities. We were able to map procedures onto specific lesions in most cases, although STS data does not, for instance, differentiate between obstructed verses unobstructed TAPVR.
Conclusion
As the field of pediatric cardiology evolves and short-term mortality decreases, the question of acceptability of parental refusal of surgical intervention becomes more salient. Given the complexities of such decisions and difficulties in prediction of long-term outcomes, it is not surprising to encounter disagreement between physicians in some situations. These differences in opinion can lead to moral conflict among staff and distress for parents. This study provides contemporary data on what CHDs may fall into a “zone of parental discretion” based on a lack of consensus among physicians about the appropriateness of legal action when parents refuse surgical treatment. These data can begin the conversation to help guide institutional policies on when it might be permissible to override parental refusals of treatment. Future studies are needed to examine how physicians balance best interest of the child in the short term against considerations of longer-term outcomes and family preferences. Further work is also needed to provide guidelines and standardize professional policies to ensure that children and families are offered similar medical options, regardless of the individual beliefs of the doctor who is providing care.
Data Availability
Data are available.
References
Oster ME, Lee KA, Honein MA et al (2013) Temporal trends in survival among infants with critical congenital heart defects. Pediatrics 131(5):1502–1508
Kon AA (2008) Healthcare providers must offer palliative treatment to parents of neonates with hypoplastic left heart syndrome. Arch Pediatr Adolesc Med 162(9):844–848
Wernovsky G (2008) The paradigm shift toward surgical intervention for neonates with hypoplastic left heart syndrome. Arch Pediatr Adolesc Med 162(9):849–854
Rychik J (2012) What does palliative care mean in the prenatal diagnosis of congenital heart disease? World J Pediatr Congenit Heart Surg 4(1):80–84
Mavroudis CD, Farrell RM, Jacobs ML, Jacobs JP, Kodish ED (2011) Informed consent, bioethical equipoise, and hypoplastic left heart syndrome. Cardiol Young 21(S2):133–140. https://doi.org/10.1017/s1047951111001715
Prsa M, Holly CD, Holly FA, Carnevale JH, Rohlicek CV (2010) Attitudes and practices of cardiologists and surgeons who manage HLHS. Pediatrics. https://doi.org/10.1542/peds.2009-1678
Kon AA, Patel A, Leuthner S, Lantos JD (2016) Parental refusal of surgery in an infant with tricuspid atresia. Pediatrics 138(5):1730
Kon AA, Ackerson L, Lo B (2004) How pediatricians counsel parents when no "best-choice" management exists: lessons to be learned from hypoplastic left heart syndrome. Arch Pediatr Adolesc Med 158:436–441. https://doi.org/10.1001/archpedi.158.5.436
Gerdes H, Lantos J (2020) Differing thresholds for overriding parental refusal of life-sustaining treatment. HEC Forum 32(1):13–20
STS Congenital Heart Surgery Database Fall 2018 Harvest for Infants and Neonates. https://www.sts.org/registries-research-center/sts-national-database/sts-congenital-heart-surgery-database
St. Louis JD, Upinder J, Jacobs JP et al (2014) Contemporary outcomes of complete atrioventricular septal defect repair: analysis of the Society of Thoracic Surgeons Congenital Heart Surgery database. J Thorac Cardiovasc Surg 146(6):2526–2531
Kane JM, Canar J, Kalinowski V, Johnson TJ, Hoehn KS (2016) Management options and outcomes for neonatal hypoplastic left heart syndrome in the early twenty-first century. Pediatr Cardiol 37(2):419–425
Downing TE, Allen KY, Glatz AC et al (2017) Long-term survival after the Fontan operation: twenty years of experience at a single center. J Thorac Cardiovasc Surg 154(1):243–253
Pundi KN, Johnson JN, Dearani JA et al (2015) 40 year follow-up after the Fontan operation: long-term outcomes of 1,052 patients. J Am Coll Cardiol 66(15):1700–1710
Newburger J, Sleeper L, Bellinger D et al (2012) Early developmental outcome in children with hypoplastic left heart syndrome and related anomalies: the Single Ventricle Reconstruction Trial. Circulation 125:2081–2091
Peyvandi S, Lupo PJ, Garbarini J, Woyciechowski S, Edman S, Emanuel BS, Mitchell LE, Goldmuntz E (2013) 22q11.2 Deletions in patients with conotruncal defects: data from 1,610 consecutive cases. Pediatr Cardiol. 34:1687–1694
Funding
None.
Author information
Authors and Affiliations
Contributions
TS—Dr. Swanson designed the study, collected data, reviewed the manuscript and approved the final version. AB—Austin performed data analysis on the collected hospital data, conceptualized and drafted the initial manuscript, and approved the final manuscript as submitted. AP—Dr. Patel collected the data from Lurie Children’s Hospital, performed the data analysis, and approved the final manuscript as submitted. SM—Dr. Maskatia collected the data from Lucile Packard Children’s Hospital and approved the final manuscript as submitted. SM—Dr. Morris collected the data from Texas Children’s Hospital and approved the final manuscript as submitted. JL—Dr. Lantos designed the study, collected data, reviewed the manuscript and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
All the authors declared that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Swanson, T.M., Patel, A., Baxter, A.J. et al. Pediatric Cardiology Specialist’s Opinions Toward the Acceptability of Comfort Care for Congenital Heart Disease. Pediatr Cardiol 41, 1160–1165 (2020). https://doi.org/10.1007/s00246-020-02367-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-020-02367-2