
Abstract
It is unclear if neonatal tetralogy of Fallot repair offers better outcomes compared to repair later in infancy. We therefore conducted a meta-analysis comparing outcomes of neonatal and non-neonatal repair. Manuscripts were identified and reviewed for quality and bias with favorably scored manuscripts being included in the final meta-analysis. Several perioperative and postoperative variables were compared. A total of 8 studies with 3858 patients were included in the analysis. Of these patients, 19% underwent neonatal repair. Neonatal repair was associated with increased mortality, longer intensive care unit stays, and longer total hospital length of stay.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Despite the vast experience and great success achieved with the surgical repair of tetralogy of Fallot, it is still unclear which management strategy is optimal for symptomatic neonates: complete repair in the neonatal period or placement of a palliative shunt followed by complete surgical repair in the non-neonatal period. The approach taken is often based on individual and institutional experience and bias, as there are no large prospective, randomized reports addressing this issue. Results of previous retrospective studies provide inconsistent conclusions and often include only limited outcomes. Thus, this study was conducted to identify published data regarding complete repair of tetralogy of Fallot in the neonatal and non-neonatal periods, evaluate the data, and pool the data to provide a summary of the outcomes associated with the two approaches.
Methods
Endpoints
A systematic review of the literature was performed to identify manuscripts describing comparisons between patients with tetralogy of Fallot who underwent complete repair in the neonatal period and those who underwent repair later in infancy (non-neonatal repair) after a neonatal systemic to pulmonary artery shunt. This was a newly conducted review with no previous review protocol having been established for it. The meta-analysis was conducted per the PRISMA checklist. The aim of the study was to compare outcomes associated with complete repair in the neonatal or non-neonatal period. The continuous variables assessed include bypass time, cross-clamp time, deep hypothermic circulatory arrest time, hospital length of stay, intensive care unit length of stay, and duration of ventilation. The dichotomous variables assessed were need for transannular patch, need for homograft or conduit, delayed sternal closure, postoperative extracorporeal membrane oxygenation (ECMO), postoperative arrhythmias requiring pharmacologic therapy or external pacing, postoperative pacemaker implantation for atrioventricular block, need for catheterization during follow-up, need for reoperation during follow-up, and mortality during follow-up.
Manuscript Search and Identification Strategy
Manuscripts were identified using electronic databases including PubMed, EMBASE, and Ovid which were queried using the following search terms: “tetralogy of fallot” in conjunction with “repair,” “neonatal,” “palliation,” or “surgery.” Only studies in English language were included for analysis. No specific restriction on year of publication was used. Resulting studies were then screened by title and abstract with manuscripts describing repairs of tetralogy of fallot retrieved in their entirety. References of these studies were then hand searched for additional relevant manuscripts. No direct contact with manuscript authors was made to obtain full text manuscripts or data in case they were not available online.
The full text manuscripts were then reviewed and assessed for quality. The Cochrane Handbook for Systematic Review of Interventions was used for quality evaluation. Published manuscripts available in full text were included in this review if they presented data from studies comparing neonatal and non-neonatal repair of tetralogy of Fallot. Studies were included in this analysis if they included at least one of the outcomes identified above.
Data Extraction
Data regarding baseline patient characteristics and outcomes were extracted from the manuscripts identified for inclusion. Trial level data were extracted with use of a data collection form. The data extraction was repeated twice to ensure integrity of the resulting data.
Bias Analysis
Bias in the included studies was assessed using the Tool to Assess Risk of Bias in Cohort Studies. Specifically, patient selection, exposure assessment, and outcome assessment were assessed using this scale in addition to other elements.
Data Analysis
Numeric data are presented as means with standard deviations or medians with ranges. Categorical data are presented as frequencies with absolute numbers as well as percentages. Meta-analysis and forest plot creation were done using RevMan 5.3(Cochrane Collaboration, Oxford, UK). A Mantel–Haenszel model was used for dichotomous outcomes and standardized mean difference for continuous outcomes. Results are presented as pooled odds ratios with 95% confidence intervals or as mean difference where appropriate. Heterogeneity between studies was identified using χ 2 and I 2 tests. For outcomes with no significant heterogeneity present, a fixed effects model was used. Otherwise a random effects model was used if either the p value was significant or the I 2 statistics was >50%. p values of ≤0.05 were considered statistically significant.
In the situation where a patient underwent placement of a systemic to pulmonary artery shunt before complete repair, data from the shunt was not taken into consideration. All durations and outcomes are reported with respect to the hospital admission associated with complete repair.
Sensitivity analyses was performed based on study weight. Metaregression was performed based on study size, age at surgery, ductal dependency, presence of symptoms, and presence of a syndrome. These were conducted on each endpoint separately except for deep hypothermic circulatory arrest time, need for homograft or conduit, and postoperative need for ECMO as these had few included studies.
Publication bias was assessed quantitatively using the Egger test. Outcomes for which the 95% confidence interval of the Egger test did not include 0 were deemed to have publication bias present.
Results
Study Characteristics
Initial search yielded 2876 manuscripts after duplicates were removed. After reviewing the study titles and abstracts, full text manuscripts were obtained for 37 studies. Of these 37 studies, 29 studies were excluded because either they did not report data regarding the outcomes of interest or they did not compare neonatal to non-neonatal repair. Eight studies were included in the final analysis (Fig. 1) [1–8]. There were a total of 3858 patients across these studies with 724 (19%) having undergone neonatal repair and 3134 (81%) having undergone non-neonatal repair (Fig. 1).

Study methodology
Baseline characteristics were not uniformly reported across all studies. For example, gender was only reported in one study. Age at neonatal repair was 8–10 days compared to 60–220 days in the non-neonatal group. A majority of those undergoing neonatal repair were ductal dependent, and nearly all of them were classified as being symptomatic. Approximately 20–40% of patients in both groups had an underlying syndrome (Table 1).
Low level of bias was found in all studies as determined by the Tool to Assess Risk of Bias in Cohort Studies (Table 2).
Bypass Time
There was no significant difference in bypass times between the two groups (standard mean difference 0.004, 95% confidence interval −0.208 to 0.215). This was based on a total of 5 studies with 203 patients in the neonatal group and 251 in the non-neonatal group [1–3, 6, 7]. An I 2 value of 37% demonstrated insignificant heterogeneity, and thus a fixed effects model was used. Publication bias was not present (Egger intercept −9.58, 95% confidence interval −25.36 to 6.21, p value 0.149) (Fig. 2).

Forest plot demonstrating results of continuous variables in the meta-analysis
Cross-Clamp Time
There was no significant difference in cross-clamp times between the two groups (standard mean difference 0.118 min, 95% confidence interval −0.106 to 0.355). Data from 4 studies with 157 patients in the neonatal group and 231 in the non-neonatal group were pooled for the analysis of cross-clamp time [1, 2, 6, 7]. An I 2 value of 45% demonstrated insignificant heterogeneity, and thus a fixed effects model was used. Publication bias was not present (Egger intercept −0.87, 95% confidence interval −12.13 to 10.40, p value 0.822) (Fig. 2).
Deep hypothermic Circulatory Arrest Time
There was no significant difference in the deep hypothermic circulatory arrest time (standard mean difference 0.084, 95% confidence interval −0.266 to 0.435). Data on deep hypothermic circulatory arrest time were available from two studies [3, 7]. While this does not allow for a meaningful pooled analysis, the data are presented to characterize this outcome. An I 2 value of 67% demonstrated significant heterogeneity, and thus a random effects model was used. Due to presence of only two studies, publication bias could not be assessed (Fig. 2).
Duration of Ventilation
There was no significant difference in duration of ventilation between the two groups (standard mean difference 0.833, 95% confidence interval −0.351 to 2.017). Data from 5 studies with 506 patients in the neonatal group and 516 in the non-neonatal group were pooled for the analysis of ventilation time [1, 2, 5–7]. An I 2 value of 98% demonstrated significant heterogeneity, and thus a random effects model was used. Publication bias was present (Egger intercept −13.66, 95% confidence interval −27.17 to −0.015, p value 0.048) (Fig. 2).
Intensive Care Unit Length of Stay
There was a significant difference in duration of intensive care unit length of stay between the two groups (standard mean difference 1.181, 95% confidence interval 0.329–2.032). Data from 5 studies with 506 patients in the neonatal group and 516 in the non-neonatal group were pooled for the analysis of intensive care unit length of stay [1, 2, 5–7]. An I 2 value of 95% demonstrated significant heterogeneity, and thus a random effects model was used. Publication bias was not present (Egger intercept −6.38, 95% confidence interval −19.04 to 6.29, p value 0.207) (Fig. 2).
Total Length of Hospital Stay
There was a significant difference in length of hospital stay between the two groups (standard mean difference 1.466, 95% confidence interval 0.368–2.563). Data from 5 studies with 506 patients in the neonatal group and 516 in the non-neonatal group were pooled for the analysis of total length of stay [1, 2, 5–7]. An I 2 value of 97% demonstrated significant heterogeneity, and thus a random effects model was used. Publication bias was not present (Egger intercept −9.58, 95% confidence interval −25.36 to 6.21, p value 0.149) (Fig. 2).
Use of Transannular Patch
There was a significant difference in need for transannular patch between the two groups (odds ratio 3.078, 95% confidence interval 1.265–7.493). Data from 5 studies with 289 patients in the neonatal group and 2817 in the non-neonatal group were pooled for the analysis of need for transannular patch [1–3, 6, 8]. An I 2 value of 74% demonstrated significant heterogeneity, and thus a random effects model was used. Publication bias was not present (Egger intercept −0.70, 95% confidence interval −6.69 to 5.29, p value 0.734) (Fig. 3).

Forest plot demonstrating results of dichotomous variables in the meta-analysis
Use of Homograft or Conduit
There was no significant difference in the odds of needing a homograft or conduit between the two groups (odds ratio 1.059, 95% confidence interval 0.536–2.094). Data from 2 studies with 198 patients in the neonatal group and 2716 in the non-neonatal group were pooled for the analysis of need for homograft or conduit [1, 8]. An I 2 value of 0% demonstrated no significant heterogeneity and thus a fixed effects model was used. Publication bias could not be assessed (Fig. 3).
Delayed Sternal Closure
Data from only 3 studies with 55 patients in the neonatal group and 90 in the non-neonatal group were pooled for the analysis of delayed sternal closure [2, 4, 6]. While this does not allow for a meaningful pooled analysis, the data are presented to simply characterize the endpoint. An I 2 value of 0% demonstrated no significant heterogeneity and thus a fixed effects model was used. There was a significant increase in the odds of delayed sternal closure associated with neonatal repair (odds ratio 3.580, 95% confidence interval 1.002–12.785). Publication bias was not present (Egger intercept −1.92, 95% confidence interval −26.66 to 22.82, p value 0.504) (Fig. 3).
Postoperative Extracorporeal Membrane Oxygenation (ECMO)
There was no significant increase in the odds of postoperative extracorporeal membrane oxygenation associated with neonatal repair (odds ratio 1.968, 95% confidence interval 0.849–4.564). Data from only 8 studies with 562 patients in the neonatal group and 2556 in the non-neonatal group were pooled for the analysis of need for postoperative ECMO [1–8]. An I 2 value of 20% demonstrated no significant heterogeneity, and thus a fixed effects model was used. Publication bias could not be quantified as only 2 of the 8 included studies had non-zero values (Fig. 3). Overall, 4% of those in the neonatal group required extracorporeal membrane oxygenation compared to 0.3% in the non-neonatal group.
Significant Postoperative Arrhythmias
There was a significant difference in the odds of postoperative arrhythmias between the two groups (odds ratio 1.777, 95% confidence interval 1.265–7.493). Data from 4 studies with 289 patients in the neonatal group and 2817 in the non-neonatal group were pooled for the analysis of postoperative arrhythmias requiring pharmacologic therapy or external pacing [3–6]. An I 2 value of 74% demonstrated significant heterogeneity, and thus a random effects model was used. Publication bias was not present (Egger intercept −0.70, 95% confidence interval −6.69 to 5.29, p value 0.734) (Fig. 3).
Postoperative Pacemaker Implantation for Atrioventricular Block
There was no significant difference in the odds of postoperative pacemaker implantation for atrioventricular block between the two groups (odds ratio 1.838, 95% confidence interval 0.628–5.382). Data from 8 studies with 562 patients in the neonatal group and 2556 in the non-neonatal group were pooled for the analysis of pacemaker implantation for atrioventricular block [1–7]. An I 2 value of 0% demonstrated significant heterogeneity, and thus a fixed effects model was used. Publication bias was not present (Egger intercept 0.48, 95% confidence interval −0.54 to 1.51, p value 0.105) (Fig. 3).
Cardiac Catheterization During Follow-Up
There was no significant difference in the odds of need for cardiac catheterization during follow-up between the two groups (odds ratio 1.312, 95% confidence interval 0.927–1.856). Data from 4 studies with 101 patients in the neonatal group and 71 in the non-neonatal group were pooled for the analysis of need for cardiac catheterization during follow-up [3–6]. An I 2 value of 44% demonstrated no significant heterogeneity, and thus a fixed effects model was used. Publication bias was not present (Egger intercept 0.54, 95% confidence interval −4.39 to 5.48, p value 0.682) (Fig. 3).
Reoperation During Follow-Up
There was no significant difference in the odds of need for reoperation between the two groups (odds ratio 1.588, 95% confidence interval 0.669–3.773). Data from 6 studies with 213 patients in the neonatal group and 260 in the non-neonatal group were pooled for the analysis of need for reoperation during follow-up [1–4, 6, 7]. An I 2 value of 74% demonstrated significant heterogeneity and thus a random effects model was used. Publication bias was not present (Egger intercept −2.66, 95% confidence interval −5.62 to 0.30, p value 0.067) (Fig. 3). Overall, 16% required reoperation in the neonatal group and 12% in the non-neonatal group.
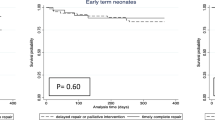
Mortality During Follow-Up
There was a significant difference in the odds of mortality between the two groups (odds ratio 3.201, 95% confidence interval 1.060–9.664). Data from 6 studies with 612 patients in the neonatal group and 2589 in the non-neonatal group were pooled for the analysis of mortality. This included mortality during the entirety of follow-up not simply the hospitalization for the index surgery [2–6, 8]. An I 2 value of 52% demonstrated significant heterogeneity, and thus a random effects model was used. Publication bias was present (Egger intercept −2.14, 95% confidence interval −3.47 to −0.80, p value 0.010) (Fig. 3). Overall mortality was 6% in the neonatal group and 1.1% in the non-neonatal group.
Meta-regression and Sensitivity Analysis
None of the variables entered into the meta-regression significantly impacted the pooled analyses for any of the endpoints.
Comment
This analysis demonstrates significant differences in the outcomes of complete repair of tetralogy of Fallot in the neonatal period versus the non-neonatal period. Neonatal repair was associated with a threefold increase in mortality and a 47% longer hospital stay, including an 18% longer intensive care unit stay. While most studies did not report the hospitalization cost, increased lengths of stay were likely associated with increased cost and potentially morbidity. Neonatal repair was also associated with a marked increase in the use of a transannular patch. This finding is not unexpected, but highlights the potential long-term morbidity associated with neonatal repair, eg increased need for reoperation, shorter time to reoperation, and right ventricular dilation [9, 10].
Postoperatively, delayed sternal closure, arrhythmias requiring treatment, pacemaker implantation for atrioventricular block, ECMO, and need for catheterization and/or reoperation were also found to occur in a higher percentage of patients with neonatal repair; however, none of these comparisons demonstrated statistical significance.
The results of our analysis support avoiding neonatal repair when feasible. The definition of feasible remains confined to the institutional level and is based on the individual patient. Common experience indicates that certain patients unambigously require intervention to improve pulmonary blood flow; certain patients will clearly do well without intervention until later in infancy; and certain patients will present management dilemmas based either on a tenuous appearing right ventricular outflow tract despite apparently adequate oxygen saturation, borderline oxygen saturations, branch pulmonary stenosis, and/or outpatient geographic distance from the major treatment center. Unfortunately, our analysis was not capable of addressing the important question—if neonatal intervention is required, which intervention offers the best long-term outcome? Data for this context and either ductal stenting or outflow tract stenting are limited. Other than repair, a systemic to pulmonary artery shunt is the most commonly used alternative. Although typically a very straightforward procedure done without cardiopulmonary bypass, shunting has been associated with appreciable cumulative mortality (hospital or discharge mortality plus mortality in the interim period prior to definitive repair) ranging from 6 to 12% [11–20]. Our bias in this context is to do complete repair, and do a shunt only in extenuating circumstances.
It is possible that the significant findings of this study are due to selection bias. Also, we were unable to add surgeon experience or center volume into our regression to determine the impact of these variables on outcomes. In addition, some endpoints were reported in a small number of studies, and publication bias was present in some of the endpoints as well.
A large, prospective, multicenter study would be helpful in determining the underlying mechanisms of noted associations and allow for a more objective allocation of patients into different strategies of treatment. Such a study with 300 patients in each group would allow for detection of a 5% change in dichotomous outcomes with 90% power.
An important limitation was the lack of data pertaining to the shunt procedure—our data was limited to outcomes of the repair. Therefore, we could not comprehensively compare the two treatment strategies from the time of diagnosis to follow-up after repair. Any prospective, randomized study should include a randomization scheme to address this important issue.
References
Woldu KL, Arya B, Bacha EA, Williams IA (2014) Impact of neonatal versus nonneonatal total repair of tetralogy of fallot on growth in the first year of life. Ann Thorac Surg 98:1399–1404
Kanter KR, Kogon BE, Kirshbom PM, Carlock PR (2010) Symptomatic neonatal tetralogy of Fallot: repair or shunt? Ann Thorac Surg 89:858–863
Kolcz J, Pizarro C (2005) Neonatal repair of tetralogy of Fallot results in improved pulmonary artery development without increased need for reintervention. Eur J Cardiothorac Surg 28:394–399
Reddy VM, Liddicoat JR, McElhinney DB, Brook MM, Stanger P, Hanley FL (1995) Routine primary repair of tetralogy of Fallot in neonates and infants less than three months of age. Ann Thorac Surg 60:S592–S596
Steiner MB, Tang X, Gossett JM, Beam BW, Malik S, Prodhan P, Angtuaco MJ (2015) Alternative repair strategies for ductal-dependent tetralogy of fallot and short-term postoperative outcomes, a multicenter analysis. Pediatr Cardiol 36:177–189
Tamesberger MI, Lechner E, Mair R, Hofer A, Sames-Dolzer E, Tulzer G (2008) Early primary repair of tetralogy of fallot in neonates and infants less than four months of age. Ann Thorac Surg 86:1928–1935
Pigula FA, Khalil PN, Mayer JE, del Nido PJ, Jonas RA (1999) Repair of tetralogy of Fallot in neonates and young infants. Circulation 100: II157–161
Al Habib HF, Jacobs JP, Mavroudis C, Tchervenkov CI, O’Brien SM, Mohammadi S, Jacobs ML (2010) Contemporary patterns of management of tetralogy of Fallot: data from the Society of Thoracic Surgeons Database. Ann Thorac Surg 90:813–819 (discussion 819–820)
Ylitalo P, Nieminen H, Pitkanen OM, Jokinen E, Sairanen H (2015) Need of transannular patch in tetralogy of Fallot surgery carries a higher risk of reoperation but has no impact on late survival: results of Fallot repair in Finland. Eur J Cardiothorac Surg 48:91–97
Kim H, Sung SC, Kim SH, Chang YH, Lee HD, Park JA, Lee YS (2013) Early and late outcomes of total repair of tetralogy of Fallot: risk factors for late right ventricular dilatation. Interact Cardiovasc Thorac Surg 17:956–962
Kirklin JW, Blackstone EH, Kirklin JK, Pacifico AD, Aramendi J, Bargeron LM Jr (1983) Surgical results and protocols in the spectrum of tetralogy of Fallot. Ann Surg 198:251–265
Vobecky SJ, Williams WG, Trusler GA, Coles JG, Rebeyka IM, Smallhorn J, Burrows P, Gow R, Freedom RM (1993) Survival analysis of infants under age 18 months presenting with tetralogy of Fallot. Ann Thorac Surg 56:944–949 (discussion 949–950)
Selmonosky CA, Farhangian D, Folger GM, Ellison RG (1972) Palliative shunting operations in tetralogy of Fallot. Effects upon the results of total correction. Ann Thorac Surg 14:16–23
Bove EL, Kohman L, Sereika S, Byrum CJ, Kavey RE, Blackman MS, Sondheimer HM, Rosenthal A (1987) The modified Blalock-Taussig shunt: analysis of adequacy and duration of palliation. Circulation 76: III19–23
Chopra PS, Levy JM, Dacumos GC Jr, Berkoff HA, Loring LL, Kahn DR (1976) The Blalock-Taussig operation: the procedure of choice in the hypoxic infant with tetralogy of Fallot. Ann Thorac Surg 22:235–238
Gladman G, McCrindle BW, Williams WG, Freedom RM, Benson LN (1997) The modified Blalock-Taussig shunt: clinical impact and morbidity in Fallot’s tetralogy in the current era. J Thorac Cardiovasc Surg 114:25–30
Blalock A, Taussig HB (1984) Landmark article May 19, 1945: the surgical treatment of malformations of the heart in which there is pulmonary stenosis or pulmonary atresia. By Alfred Blalock and Helen B. Taussig. JAMA 251:2123–2138
Brock R (1948) Pulmonary valvotomy for relief of congenital pulmonary stenosis. Report of 3 cases. Br Med J 1:1121
Lillehei CW, Cohen M, Warden HE, Read RC, Aust JB, Dewall RA, Varco RL (1955) Direct vision intracardiac surgical correction of the tetralogy of Fallot, pentalogy of Fallot, and pulmonary atresia defects; report of first ten cases. Ann Surg 142:418–442
Kirklin J, DuShane J, Patrick R, Donald D, Hetzel P, Harshbarger H, Wood E (1955) Intracardiac surgery with the help of a mechanical pump-oxygenator system (Gibbon type): report of eight cases. Mayo Clin Proc 30:201
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There are no financial disclosures or conflicts of interest for any of the authors.
Rights and permissions
About this article

Cite this article
Loomba, R.S., Buelow, M.W. & Woods, R.K. Complete Repair of Tetralogy of Fallot in the Neonatal Versus Non-neonatal Period: A Meta-analysis. Pediatr Cardiol 38, 893–901 (2017). https://doi.org/10.1007/s00246-017-1579-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-017-1579-8