
Abstract
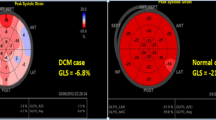
Guidelines for diagnosis and grading of diastolic dysfunction (DD) in children have not been established. The applicability of adult parameters of DD to children has been questioned by recent studies. Although normal diastolic parameters in children have been published, the data to support application of these indices for the non-invasive diagnosis of DD and quantifying its degree are still being developed. Restrictive cardiomyopathy (RCM) is the only recognized disease entity in children that presents with isolated, irreversible DD as the predominant finding. The aim of this study was to investigate the applicability of current diastolic indices used for assessment of diastolic function in adults as reliable indicators of DD in children with established RCM. Retrospective review of institutional clinical database for the period of 2002–2010 was performed to identify patients with RCM who had had a comprehensive echocardiographic assessment of diastolic function. The following parameters were obtained from apical four chamber view: mitral valve (MV) inflow Doppler early filling velocity (E), late filling velocity (A), deceleration time (DT), color M-mode flow propagation from MV to apex (Vp), Doppler tissue imaging derived early diastolic velocity E′ and late diastolic velocity A′ at the LV lateral wall at MV annulus, RV at the tricuspid valve annulus, septum, and LA area. All parameters were compared to age and gender matched controls using student t test. : LA area/BSA was significantly larger in RCM group than the control group, median 22.8 cm2/m2 (range 16.9–28.6) versus 10.3 cm2/m2 (range 8.3–12.3), p value <0.001. MV inflow E and A were lower, and DT was shorter in the RCM group (p = 0.04, 0.02, and 0.005, respectively). A wave was absent in 3 of 9 patients in the RCM group. Ratio of E to A (E/A) was not different between the two groups. E′ was significantly lower at all three sites in RCM group; however, there was some overlap between the two groups. E/septal E′ ratio was statistically significantly higher in RCM group. A′ was absent either at lateral wall or at septum in five patients. 7 of 9 patients in RCM group had L′ wave (at lateral wall or septum) defined as negative deflection during diastasis. Vp was higher in RCM group than in the control group 81.4 ± 44.5 versus 52.9 ± 10.9, p value <0.01. Combination of increased left atrial size, septal E/E′, and lack of A wave and presence of mid-diastolic L′-wave are the noted abnormalities in this group. Individual cut-offs for Doppler indices have very poor sensitivity in identifying restrictive physiology. These findings suggest that poor LV compliance is the hallmark of restrictive cardiomyopathy in children even in the presence of normal early relaxation and ventricular filling. These findings support the need for development of guidelines for diagnosis and physiologic grading of diastolic dysfunction in children.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Guidelines on diagnosis and grading of diastolic dysfunction (DD) in children have not been established. Application of adult paradigms of DD to children has been questioned by recent studies [3]. Although normal diastolic parameters in children have been published [4, 14], non-invasive diagnosis of pediatric DD continues to be a challenge. It is possible that isolated diastolic dysfunction may be under recognized and not routinely diagnosed in children. Restrictive cardiomyopathy (RCM) is one of very few clinical entities in pediatric population that presents with irreversible severe diastolic dysfunction as the predominant finding with preserved systolic function in most cases. The aim of this study was to investigate the applicability of current diastolic indices used for assessment of diastolic function in adults as reliable indicators of irreversible severe DD in children with RCM.
Methods
Study Population
Retrospective review of a single institution (Mount Sinai Medical Center, New York) clinical database from 2002 to 2010 was performed to identify pediatric patients with RCM. Patients with a diagnosis of RCM confirmed by cardiac catheterization and with comprehensive echocardiographic diastolic assessment per institutional protocol were included for analysis. They were compared to 27 age- and gender-matched controls that had undergone echocardiographic evaluation for various reasons including investigation of innocent murmurs and chest pain. The cardiac catheterization data and biopsy results of RCM patients were also reviewed. The study was approved by the institutional review board.
Echocardiographic Examination
Echocardiography was performed on Siemens (Sequoia C512, Mountainview, CA) and GE (Vivid 7, Milwaukee, WI) with probe frequencies appropriate for patient size. The following echocardiographic parameters were measured either directly from online measurements or from EchoPAC (GE, Milwaukee, WI) from apical four chamber view: mitral valve (MV) inflow Doppler early filling velocity (E), late filling velocity (A), deceleration time (DT), color M-mode flow propagation from MV to apex (Vp), Doppler tissue imaging (DTI) derived early diastolic velocity E′ and late diastolic velocity A′ at the LV lateral wall and septum. The ratios of E to averaged or mean of E′ of LV lateral wall and septum were also calculated. Myocardial velocities were recorded using a standard pulse wave Doppler technique; high frequency signals were filtered by adjusting Nyquist limit to a velocity range of 15–20 cm/sec. Gain was optimized to get a clear signal. Left atrial (LA) area was also measured from apical four chamber view at end-systole. Myocardial performance index (MPI) which represents both systolic and diastolic function was calculated using mitral inflow spectral Doppler as well as DTI.
Reproducibility
Interobserver variability was assessed by comparing measurements done by a senior sonographer and a clinical fellow (NS). Variability was calculated as the mean percent error, derived as the difference between the two sets of measurements, divided by the mean of the observations.
Statistics
Student t test was used to compare the two groups. Spearman rank correlation coefficient was used to assess the correlation between various diastolic parameters and pulmonary capillary wedge pressure (PCWp) or left atrial pressure (LAp). Statistical analysis was performed using commercially available software (Microsoft Office Excel 2007, Microsoft Corporation, Seattle, WA and StataCorp LP, College Station, TX). A p value <0.05 was considered as statistically significant.
Results
Patient Demographics
Of the 12 identified patients with a diagnosis of restrictive cardiomyopathy, two who did not have DTI data and one patient with isolated right ventricular disease were excluded. Nine patients aged 3–17 years (median 9.3 years) were included in the study. These patients met the diagnostic criteria for RCM; severe diastolic dysfunction as evidenced by elevated left, right, or biventricular end-diastolic pressures, [4] normal or near normal left ventricular systolic function, absence of significant left ventricular hypertrophy or dilation, and no evidence of pericardial disease [13].
Mean right atrial (RA) pressure was 11 mmHg (range 2–18), and pulmonary capillary wedge pressure (PCWP) was 22 mmHg (range 16–28). Histology of the patients’ myocardium was available either from right ventricular endomyocardial biopsy or from the explanted heart. Seven showed myocyte hypertrophy and fibrosis, one showed rhabdomyomata, and histology was not available in one patient. Amyloidosis was not present in any of the specimens.
LA Area
LA area/BSA was significantly larger in RCM group than the control group as expected, median 22.8 cm2/m2 (range 16.9–28.6) versus 10.3 cm2/m2 (range 8.3–12.3), p value <0.001. LA size had the least overlap with the controls (Table 1).
MV Inflow Doppler Indices
Comparisons of E, A and DT are shown in Table 2. E and A were lower, and DT was shorter in the RCM group (p < 0.04, 0.02, and 0.0001, respectively). However, there was significant overlap between RCM and controls. A was absent in 3 of 9 patients in the RCM group. Ratio of E to A (E/A) was not different between the two groups. A wave duration time was not available for analysis. MPI was higher in RCM 0.59 ± 0.17 versus 0.44 ± 0.1, p value <0.001; however, significant overlap between the two groups was again observed (Fig. 2).
Pulmonary Vein Doppler
Peak A wave reversal velocity was higher in the RCM group, 0.28 ± 0.14 versus 0.20 ± 0.05, p 0.02.
DTI Derived Indices
Comparisons of E′ and ratio E/E′ are shown in Table 3. Lateral annulus and septum E′ were significantly lower in RCM group; however, there was some overlap between the two groups (Fig. 2). LV lateral wall, septum E/E′, and the E/mean of septal and lateral annulus E′ were all higher in RCM group with the least overlap in the ratio noted for the septum (Fig. 2). Unlike the adult data, a “cut-off” value for these ratios and indices could not be established. If the published adult cut-off value of eight was used for E/E′ in our population, the sensitivity and specificity would be 22 and 100 % for E/E′ lateral annulus and 44 and 96 % for E/E′septum, respectively. A′ was absent either at lateral wall or at septum in five patients. Additionally, seven patients had L′ wave defined as negative deflection during diastasis (Fig. 1). L′ was absent in the control. The sensitively and specificity of having L′ at either at lateral wall or at septum are 78 and 100 %, respectively. MPI at lateral wall and septum were both higher in RCM group (Table 3).

Abnormal DTI in RCM patient. Note the L′ wave in mid-diastole and absence of A′
Flow Propagation Velocity (Vp)
Vp was higher in RCM group than in the control group 81.4 ± 44.5 versus 52.9 ± 10.9 cm/sec, p value <0.001, and the ratio E/Vp was lower in RCM group 0.75 ± 0.34 versus 1.91 ± 0.48, p value <0.001; however, there was significant overlap with the controls (Fig. 2).

a LA area, b E/A ratio, c DT, d MPI, e E′ at LVF, f E′ at septum, g E/E′ ratio at LVF, h E/E′ ratio at septum, i E/mean E′ ratio, j Vp, k E/Vp ratio
Correlation with PCWp/LAp
There was no significant correlation between LAp and septal E/E’ (r = −0.14, p = 0.71), E/E′mean (r = −0.008, p = 0.98), Vp (r = 0.29, p = 0.46), and indexed LA area (r = −0.008, p = 0.98) (Fig. 3).

Correlation between PCWp/LAp (mmHg) and various diastolic parameters
Reproducibility
Interobserver variability for each parameter was; E 6.5 %, A 12 %, DT 1.3 %, pulmonary vein peak A reversal velocity 13.1 %, A duration 0.8 %, lateral E′ 3 %, lateral A′ 21.8 %, septal E′ 2.9 %, and septal A′ 3.5 %.
Discussion
In this study, we sought to assess the validity of the various parameters that have been used to assess diastolic function in adults by testing whether they could reliably characterize severe DD in pediatric patients with RCM. RCM is a well-described disease process known to primarily present with severe irreversible DD without significant systolic dysfunction. There were several interesting findings observed in our study. (1) Left atrial size distinguished the two groups most significantly with the least overlap. (2) Mitral inflow Doppler did not demonstrate a typical “restrictive” pattern. (3) E′ was lower in RCM group; however, there were RCM patients with normal E′ values for their age. (4) Septal E/E′ was significantly different in RCM compared to E/E′ for MV annulus. (5) In about half of RCM patients, late diastolic velocity or A wave and A′ was absent in either mitral inflow Doppler or in DTI, and in the rest, the velocity was decreased. (6) L′ wave was not seen in any controls but observed in 7 out of 9 RCM patients suggesting that there is antegrade flow across the atrioventricular valve during diastasis. (7) Vp was higher in RCM group, contrary to previously published adult and pediatric data [1, 2, 8, 9]. (8) There was no correlation between catheterization derived LAp and various diastolic parameters in this small sample of patients.
Normal pediatric LA volume values have been published, and the indexed LA volume to body surface area has been shown to reflect chronic LV volume overload as well as increased LV filling pressures [15]. In our study, we also demonstrated that increased LA size reflected the increased filling pressure in patients with RCM.
In adults patients, stages of DD have been described with impaired relaxation diagnosed by decreased E/A and E′ at the lateral annulus and septum in stage one, and these patients are the least symptomatic while increased E/A ratio or restrictive filling pattern, increased E/E′ and E/Vp characterize advanced DD [8]. Even though all of our patients had elevated left atrial or PCWp, they did not have restrictive filling pattern on the MV inflow Doppler. Although as a group, RCM patients had impaired relaxation indicated by decreased E′, there were patients (n = 6 at lateral wall and n = 4 at septum) who had normal E′ or early relaxation. The continuum of severity of progression of DD starting with impaired relaxation and progressing to irreversible loss of ventricular compliance and elevated left atrial pressures seen in adults may not be seen in children. Leonardi et al. evaluated 24 children with transfusion dependent thalassemia. None of the patients had heart failure symptoms at the time of evaluation; however, all showed restrictive filling pattern defined by E/A > 1.5 and DT < 140 ms and normal relaxation [6]. Dragulescu et al. assessed the adequacy of current adult diastolic dysfunction guidelines in pediatric cardiomyopathy. They defined failure to classify diastolic dysfunction when there was discordance between E′ and LA size. The severity of diastolic dysfunction could not be classified in as many as 37 % of patients with cardiomyopathy [3].
Gewillig et al. reported six cases of pediatric RCM who had increased E/A ratio to greater than four and prominent mid-diastolic mitral L wave [5]. By cardiac catheterization, the LV pressure curve showed a steady decline during diastasis and concluded that restrictive hemodynamics were most likely result from dysfunction and delay of active relaxation and not caused by increased intrinsic stiffness. We did not observe prominent L wave in the inflow Doppler; however, we did observe L′ wave in DTI tracings. Lack of atrial contribution to the filling in some patients with RCM- absence of late diastolic velocity supports the pathophysiology of restriction in some.
Vp has been shown to negatively correlate with time constant of LV pressure decay (Tau) in adults with coronary artery disease and cardiomyopathy [2], systolic and diastolic dysfunction [16], and hypertrophic cardiomyopathy [9]. It has also been validated in pediatric population [1]. In our patient population, Vp was higher than in the normal group, not decreased. Increased Vp is often seen in constrictive pericarditis [12]. One can also hypothesize that there may be a role of increased pericardial constraint in children with RCM; however, the fact that Vp is increased in these children with restrictive physiology warrants more investigation. Diastolic heart failure is a well-described disease entity in the adult population comprising approximately half of adults with newly diagnosed heart failure, and its prevalence has steadily increased over the past decade [11].Because of the clinical implications of heart failure with normal ejection fraction in adults, non-invasive assessment of diastolic function has advanced significantly. On the other hand, isolated diastolic heart failure is rare in children, and applicability of the echocardiographic diastolic indices in assessment of DD in children needs further examination. Our study suggests that children may not exhibit all stages of DD, and the mechanisms of DD may be variable. Dilated LA and elevated E/E′ septum correlate well with the physiology of poor LV compliance and elevated LA pressures in children with RCM. The findings of normal E′, absence of A′, and presence of L′ suggest that early active relaxation may be preserved and probably delayed with associated absence of late passive filling. Based on these findings, we suggest that a comprehensive diastolic function evaluation should incorporate careful evaluation of all indices and left atrial size. Very often incongruence is noted between MV inflow, pulmonary vein Dopplers, and DTI indices. Additionally, significant variability within the indices is noted with respect to patient age and size. We suggest characterizing diastolic dysfunction by either presence of impaired relaxation or compliance or both rather than extrapolating from adult criteria for defining different stages and degree of DD in children.
Limitations
We were only able to enroll nine patients in our study. A protocol mandating universal DTI acquisition was introduced in 2000 in our echocardiography laboratory. Thus, patients seen prior to that date did not have DTI data. We were unable to calculate left atrial volume as most of our RCM patients had limited orthogonal views of the left atrium; thus, only the area of the left atrium obtained from the apical 4 chamber view could be calculated for comparison to the normal control.
The interobserver variability for each parameter was acceptable. The only exception was lateral A′ where the mean percent error was 21.8 %. This likely resulted from measuring the L′ velocity as A′ by one of the observers in some patients who had absence of A′ (Fig. 1).
Restrictive cardiomyopathy is a rare disorder in children accounting for only 2–5 % of all pediatric cardiomyopathies [7, 10]. Future investigation in a larger patient population is required to study the mechanism of restrictive physiology in children.
Conclusion
Our study demonstrates the variability in the diastolic indices when used to grade DD in children with RCM. Combination of increased left atrial size, increased septal E/E′ and lack of A wave and presence of mid-diastolic L′-wave were the most significant abnormalities noted in RCM. Individually, E/E′ and E′ alone were noted to be normal in majority of RCM patients, and presence of L′ as an individual parameter had the highest sensitivity and specificity. Contrary to what has been noted in the adult population, decreased LV compliance may exist even with preserved early relaxation properties of the myocardium. Our observations along with the previously published data support the need for more collaborative research in order to develop guidelines for diagnosis and physiologic grading of diastolic dysfunction in children.
References
Border WL, Michelfelder EC, Glascock BJ, Witt SA, Spicer RL, Beekman RH 3rd et al (2003) Color M-mode and doppler tissue evaluation of diastolic function in children: simultaneous correlation with invasive indices. J Am Soc Echocardiogr 16(9):988–994
Brun P, Tribouilloy C, Duval AM, Iserin L, Meguira A, Pelle G et al (1992) Left ventricular flow propagation during early filling is related to wall relaxation: A color M-mode doppler analysis. J Am Coll Cardiol 20(2):420–432
Dragulescu A, Mertens L, Friedberg MK (2013) Interpretation of left ventricular diastolic dysfunction in children with cardiomyopathy by echocardiography: problems and limitations. Circ Cardiovasc Imaging 6(2):254–261
Eidem BW, McMahon CJ, Cohen RR, Wu J, Finkelshteyn I, Kovalchin JP et al (2004) Impact of cardiac growth on doppler tissue imaging velocities: a study in healthy children. J Am Soc Echocardiogr 17(3):212–221
Gewillig M, Mertens L, Moerman P, Dumoulin M (1996) Idiopathic restrictive cardiomyopathy in childhood. A diastolic disorder characterized by delayed relaxation. Eur Heart J 17(9):1413–1420
Leonardi B, Margossian R, Colan SD, Powell AJ (2008) Relationship of magnetic resonance imaging estimation of myocardial iron to left ventricular systolic and diastolic function in thalassemia. JACC Cardiovasc Imaging 1(5):572–578
Lipshultz S, Sleeper L, Sleeper L, Towbin J, Lowe A, Orav E, Cox G et al (2003) The incidence of pediatric cardiomyopathy in two regions of the united states. N Engl J Med 348(17):1647–1655
Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA et al (2009) Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr 22(2):107–133
Nishihara K, Mikami T, Takatsuji H, Onozuka H, Saito N, Yamada S et al (2000) Usefulness of early diastolic flow propagation velocity measured by color M-mode doppler technique for the assessment of left ventricular diastolic function in patients with hypertrophic cardiomyopathy. J Am Soc Echocardiogr 13(9):801–808
Nugent AW, Daubeney PE, Chondros P, Carlin JB, Cheung M, Wilkinson LC et al (2003) The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med 348(17):1639–1646
Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM (2006) Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 355(3):251–259
Rajagopalan N, Garcia MJ, Rodriguez L, Murray RD, Apperson-Hansen C, Stugaard M et al (2001) Comparison of new doppler echocardiographic methods to differentiate constrictive pericardial heart disease and restrictive cardiomyopathy. Am J Cardiol 87(1):86–94
Rivenes SM, Kearney DL, Smith EO, Towbin JA, Denfield SW (2000) Sudden death and cardiovascular collapse in children with restrictive cardiomyopathy. Circulation 102(8):876–882
Swaminathan S, Ferrer PL, Wolff GS, Gomez-Marin O, Rusconi PG (2003) Usefulness of tissue doppler echocardiography for evaluating ventricular function in children without heart disease. Am J Cardiol 91(5):570–574
Taggart NW, Cetta F, O’Leary PW, Seward JB, Eidem BW (2010) Left atrial volume in children without heart disease and in those with ventricular septal defect or patent ductus arteriosus or hypertrophic cardiomyopathy. Am J Cardiol 106(10):1500–1504
Takatsuji H, Mikami T, Urasawa K, Teranishi J, Onozuka H, Takagi C et al (1996) A new approach for evaluation of left ventricular diastolic function: Spatial and temporal analysis of left ventricular filling flow propagation by color M-mode doppler echocardiography. J Am Coll Cardiol 27(2):365–371
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sasaki, N., Garcia, M., Ko, H.H. et al. Applicability of Published Guidelines for Assessment of Left Ventricular Diastolic Function in Adults to Children with Restrictive Cardiomyopathy: An Observational Study. Pediatr Cardiol 36, 386–392 (2015). https://doi.org/10.1007/s00246-014-1018-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-014-1018-z