
Abstract
Long-term survival after tetralogy of Fallot (TOF) repair is excellent. However, little is published regarding late noncardiac complications. This study aimed to determine the prevalence and risk factors for renal dysfunction among adults after TOF repair. For this study, 56 adult patients with complete repair of TOF were identified, and their charts were retrospectively reviewed. An estimated glomerular filtration rate (eGFR) for each patient was calculated using the Modification of Diet in Renal Disease formula (MDRD). Using each patient’s eGFR, he or she was classified into stages based on the National Kidney Foundation chronic kidney disease (CKD) staging. Clinical parameters were compared among patients with and those without renal dysfunction to identify risk factors for renal impairment. The median estimated eGFR rate for the cohort was 78 ml/min/1.73 m2. Based on the National Kidney Foundation CKD staging system, 54 % of the patients had at least stage 2 chronic renal disease. The risk factors identified were hypertension (p < 0.01), type 2 diabetes mellitus (p < 0.05), longer follow-up evaluation (p < 0.005), older age at complete repair (p < 0.05), and use of daily diuretics (p < 0.05). After repair of TOF, renal dysfunction is common at late follow-up evaluation. The study findings show the importance of routine assessment of renal function and the need to limit or avoid future episodes of acute kidney injury in this at-risk population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
After tetralogy of Fallot (TOF) repair, numerous studies have demonstrated excellent long-term survival. The patients, however, remain at life-long risk for multiple late cardiac complications.
Over the last several years, it has been increasingly apparent that the effects of congenital heart disease extend beyond the cardiovascular system, affecting multiple other organ systems. Examples of these late complications include restrictive lung disease [11], hepatic dysfunction [18], and renal impairment [4, 7]. Chronic kidney disease (CKD) is reported to be common among adults with repaired congenital heart disease [4]. Additionally, CKD in the adult with congenital heart disease is a predictor of mortality, associated with up to a fivefold higher mortality than among those without CKD [4].
Currently, the prevalence and risk factors for renal dysfunction in adults after previous palliation of TOF remains poorly defined. We aimed to determine the prevalence of renal dysfunction in our adult patients with a history of previous TOF palliation and to identify associated risk factors of the development of CKD.
Methods
After approval from the Children’s Hospital of Wisconsin Institutional Review Board (IRB), 56 adult patients (median age, 39 years; range, 18–69 years) with a history of repaired TOF were identified. All the patients were followed in the Wisconsin Adult Congenital Heart Disease Program and had been seen in an ambulatory setting within the preceding 12 months. Charts were reviewed retrospectively and pertinent data collected.
Using gender, age, and baseline laboratory values, an estimated glomerular filtration rate (eGFR) for each patient was estimated using the Modification of Diet in Renal Disease formula (MDRD) [6]. Each patient’s eGFR was used to classify him or her into stages of CKD based on the National Kidney Foundation CKD staging system (Table 1). This was originally defined by the Kidney Disease Outcome Quality Initiative (NKF-K/DOQI) in 2002 [9]. Findings have shown this staging system be a predictor of cardiovascular morbidity and mortality for adults with acquired heart disease [8, 14]. We chose to define the presence of renal dysfunction as a reduced eGFR classified as CKD stage 2 or higher.
Statistical Analysis
Continuous variables were analyzed using a two-sample t test or the Mann–Whitney rank sum test, whereas Fisher’s exact test was used for categorical variables. The associations between variables were assessed by Spearman rank order correlation analysis. A p value lower than 0.05 was considered statistically significant.
Results
The median follow-up period from the time of complete repair was 35 years (range, 15–54 years). Overall, 36 of the patients (64 %) had undergone a previous shunt placement before complete repair. Two previous surgeries had been performed for 71 % of our patients, three surgeries for 20 %, and four surgeries for 13 %. Four patients had identified chromosomal abnormalities, with three having 22Q11.2 microdeletion syndrome and one having CHYME syndrome. Importantly, five patients had hypertension. Three of these five patients also had concurrent type 2 diabetes mellitus. Finally, three patients had known renal anomalies. Two patients had a solitary kidney, and one patient had a known horseshoe kidney. Importantly, none of these three patients with renal anomalies had a history of renal dysfunction or were being followed actively by nephrology (Table 2).
At the time of their last clinic evaluation, the majority of our patients were categorized as New York Heart Association (NYHA) functional class 1, 39 % as functional class 2 or 3, and none as class 4. As shown by echocardiographic analysis, 29 % of our patients had moderate or severe pulmonary regurgitation. Importantly, only 27 % of our cohort had decreased right ventricular systolic function, with only three of these patients having moderate or severely reduced systolic function. Nine patients (16 %) had decreased left ventricular systolic function, defined as an ejection fraction of less than 55 %. Six of these patients were receiving an angiotensin-converting enzyme inhibitor or angiotensin 2 receptor blocker. Eleven patients (20 %) were taking daily diuretics.
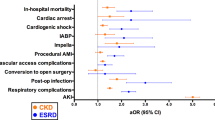
The median eGFR rate for the cohort was 78 ml/min/1.73 m2 (range, 8–125 ml/min/1.73 m2) (Fig. 1). Overall, based on the National Kidney Foundation CKD staging system, 54 % of our cohort (n = 30) had abnormal kidney dysfunction, defined as stage 2 CKD or higher. Overall, 23 (41 %) of the 30 patients with abnormal kidney function had CKD stage 2, 6 (11 %) had CKD stage 3, and 1 had CKD stage 5.

Distribution of the estimated eGFR among the study cohort, with a mean eGFR of 78 ml/min/1.73 m2 for the group, as calculated by the MDRD
We next compared the overall prevalence of renal dysfunction in our cohort with that predicted for the general population and that predicted for different age cohorts (Fig. 2). The predicted prevalence of stage 2 kidney disease or higher in the general population is ~10 %. This is significantly lower than the prevalence of 54 % identified in our cohort (p < 0.05).

Prevalence of CKD in the general adult population versus that among adults with repaired TOF by age groups. *p < 0.05
When our cohort was further divided into different age groups, he result was similar findings, with all age groups in our cohort having a higher prevalence of renal dysfunction than predicted for the general population (p < 0.05). For our cohort, the prevalence of CKD was 14 % among those 20–39 years of age, 52 % among those 40–59 years of age, and 80 % for those 60–69 years of age. All these values are significantly higher than the predicted prevalences of CKD in the general population, estimated respectively at 2 % for those 20–39 years of age, 8 %, for those 40–59 years of age, and 21 % for those 60–69 years of age.
When analyzed, type 2 diabetes (p < 0.05) and hypertension (p < 0.01) were found to be significant risk factors for the development of CKD in our cohort of patients. All three patients with diabetes and all five patients with hypertension had renal dysfunction. Another significant risk factor was the length of the follow-up period. Patients with renal dysfunction had a longer mean follow-up period (43 vs. 30 years in the normal cohort; p < 0.005). Patients with renal dysfunction also were found to be older at time of complete repair, with a mean age of 10 versus 5 years (p < 0.05). Finally, patients with renal dysfunction were more likely to require daily diuretics than those with normal renal function (p < 0.05) (Table 3).
In addition to these significant risk factors, several other trends were identified. Compared with patients who had normal kidney function, patients with renal dysfunction were more likely to have undergone a previous shunt placement (50 vs. 38 %), more likely to have decreased LV systolic function (23 vs. 8 %), and finally, more likely to have decreased RV systolic function (37 vs. 15 %). None of these factors, however, reached significance.
Other factors that were not significant included number of previous surgeries, presence of chromosomal anomaly, or presence of renal anomaly (Table 3).
When the patients with hypertension and diabetes mellitus were excluded from the analysis, similar results were found. For the remaining 51 patients, the significant risk factors included length of the follow-up period (39 vs. 29 years; p < 0.05), older age at the time of complete repair (7 vs. 4.5 years; p < 0.03), and greater likelihood of daily diuretics use (p < 0.05) (Table 4).
Discussion
Our data demonstrate that the prevalence of renal impairment among patients with repaired TOF is significantly higher than expected for the general population [3]. The etiology of CKD in this population is clearly multifactorial. Data show that long-standing cyanosis, exposure to nephrotoxic medications, and multiple previous cardiac catheterizations all contribute [7]. In addition, all these patients have needed multiple previous surgeries requiring cardiopulmonary bypass. Cardiopulmonary bypass is a well-known risk factor for acute kidney injury, with as many as 30–50 % of adult patients experiencing acute kidney injury after cardiopulmonary bypass [5, 8, 13]. In addition, a number of investigators have shown that multiple episodes of acute kidney injury have a cumulative effect, leading to CKD [1, 16].
In our analysis, patients had worse renal function if complete repair occurred at a later age. In addition, a trend among the patients with CKD was a greater likelihood of having undergone a previous Blalock–Taussig shunt placement. Both of these variables suggest that patients more likely to experience the development of CKD may have been cyanotic longer [4, 7]. Dimopoulos et al. [4] found cyanosis to be a strong multivariable predictor of eGFR in a large retrospective review of patients with adult congenital heart disease followed at their center. Several previous papers have discussed the relationship between long-standing cyanosis and the risk for cyanotic glomerulopathy [5, 7, 10]. Although the relationship between cyanosis and renal dysfunction is well established, the underlying mechanism leading to renal dysfunction is debated. Most experts believe that chronic hypoxia likely has both direct and indirect effects leading to renal dysfunction [5, 7, 10].
Other risk factors for renal dysfunction in adult congenital heart disease patients identified in previous studies include age at follow-up evaluation, use of diuretics, and ventricular function [4]. In our study, we found similar risk factors. The patients in our cohort with renal dysfunction clearly were older and more likely to be using diuretics. In addition, the patients with renal dysfunction in our series manifested a trend for decreased systolic function.
In patients with acquired heart disease and ventricular dysfunction, end organ perfusion often is compromised. Decreased renal perfusion leads to activation of neurohormonal physiology, such as the sympathetic nervous system or the renin-angiotensin cascade, potentiating ventricular remodeling and retention of sodium and water [12]. This ultimately may lead to a slow progression of cardiac and renal insufficiency. It is reasonable to assume that this cycle also is present in patients with congenital heart disease.
Not surprisingly, the presence of hypertension and type 2 diabetes mellitus also were found to be risk factors for the development of renal dysfunction in our cohort. The mechanisms of both disorders that affect kidney function have been well described in the literature. Importantly, the prevalence of CKD in our cohort remained well above the expected prevalence in the general population even when patients with type 2 diabetes mellitus and hypertension were excluded from our analysis. We believe this is a very important finding that emphasizes the importance of routine screening for other treatable risk factors (i.e., hypertension and type 2 diabetes mellitus) in this high-risk patient group.
The impact of CKD on both total and cardiovascular morbidity and mortality in adults with acquired heart disease is well described in the literature. The prevalence and impact of CKD on the adult with congenital heart disease, however, has rarely been evaluated [4]. Similar to our data, Dimopoulos et al. [4] found a high prevalence of renal dysfunction among adults with congenital heart disease, with 50 % of the 1,100 patients evaluated in their program having at least stage 2 CKD. Even more concerning was that in this study, patients with CKD beyond stage 3 had a 6-year mortality rate fivefold higher than those with normal kidney function. Similar to our data, the majority of patients in their study had only mildly reduced renal function. However, in their study, the prevalence of even mildly reduced renal function carried an increased risk of mortality, with a twofold increase in the 6-year mortality rate versus that among patients who had a normal eGFR [4].
In our study, we risk stratified our patients using the National Kidney Foundation CKD staging system. In this staging system, the calculated eGFR for each patient is extremely important for decision making. The MDRD is a widely accepted and implemented formula that factors serum creatinine, age, sex, and race [6]. Other calculations, such as the Crockraft and Gault equation [2], incorporate body weight, whereas pediatric calculations such as the Schwartz formula incorporate height [15]. It is important to note that although these calculations are indeed estimates, they are more accurate than the use of serum creatinine alone and should be applied to monitor for the progression of CKD.
The MDRD, validated in many studies, is used in the Kidney Disease Outcome Quality Initiative (NKF-K/DOQI) staging system. Finally, the MDRD also has performed well when studied in adults with congenital heart disease [17].
Study Limitations
Our study was limited by its retrospective design. The study encompassed many years of medical data, and although we analyzed all information, complete medical history was not necessarily available. For example, we were unable to account for all nephrotoxic exposures such as contrast dye or antibiotics throughout each patient’s lifetime. Urine analysis was not available for all our patients when data were collected, precluding the ability to evaluate for proteinuria, and thus potentially underestimating the degree of renal insufficiency in our cohort. Finally, a larger sample of patients would have added power to the study as well as further delineation of which nonsignificant associations may have contributed to renal insufficiency.
Conclusion
In conclusion, renal dysfunction in adults after surgical repair of TOF is common, and the prevalence is much higher than expected compared with the general population. Our results emphasize the importance of routine assessment of renal function and the need to limit or avoid future episodes of acute kidney injury in this at-risk population.
References
Chawla LS, Amdur RL, Amodeo S et al (2011) The severity of acute kidney injury predicts progression to chronic kidney disease. Kidney Int 79:1361–1369
Cockcroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16:31–41
Coresh J, Selvin E, Stevens LA et al (2007) Prevalence of chronic kidney disease in the United States. J Am Med Assoc 17:2038–2047
Dimopoulos K, Diller GP, Jiktsudam D et al (2008) Prevalence, predictors, and prognostic value of renal dysfunction in adults with congenital heart disease. Circulation 117:2320–2328
Dittrich S, Kurschat K, Dahnert I et al (2000) Renal function after cardiopulmonary bypass surgery in cyanotic congenital heart disease. Int J Cardiol 73:173–179
Levey AS, Bosch JP, Breyer Lewis J et al (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med 330:877–884
Martinez-Quintana E, Rodriguez-Gonzalexz F, Fabregas-Brouard M, Nieto-Lago V (2009) Serum and 24-hour urine analysis in adult cyanotic and noncyanotic congenital heart disease patients. Congenit Heart Dis 4:147–152
Muntner P, He J, Hamm L, Loria C, Whelton PK (2002) Renal insufficiency and subsequent death resulting from cardiovascular disease in the United States. J Am Soc Nephrol 13:745–753
National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39:S1–S266
Perloff JK, Latta H, Barsotti P (2000) Pathogenesis of the glomerular abnormality in cyanotic congenital heart disease. Am J Cardiol 86:1198–1204
Pianosi PT, Johnson JN, Turchetta A, Johnson BD (2009) Pulmonary function and ventilatory limitation to exercise in congenital heart disease. Congenit Heart Dis 4:2–11
Rastogi A, Fonarow GC (2008) The cardiorenal connection in heart failure. Curr Cardiol Rep 10:190–197
Rosner MH, Okusa MD (2006) Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol 1:19–32
Sarnak MJ, Levey AS, Schoolwerth AC et al (2003) Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 42:1050–1065
Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A (1976) A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 58:259–263
Thakar CV, Christianson A, Himmelfarb J, Leonard AC (2011) Acute kidney injury episodes and chronic kidney disease risk in diabetes mellitus. Clin J Am Soc Nephrol 6:2567–2572
Tutarel O, Denecke A, Bode-Boger SM, Martens-Lobenhoffer J, Schieffer B, Westhoff-Bleck M, Kielstein JT (2011) Symmetrical dimethylarginine outperforms CKD-EPI and MDRD-derived eGFR for the assessment of renal function in patients with adult congenital heart disease. Kidney Blood Press Res 34:41–45
Wu FM, Ukomadu C, Odze RD et al (2011) Liver disease in the patient with Fontan circulation. Congenit Heart Dis 6:190–201
Acknowledgments
The authors gratefully acknowledge Mary Krolikowski for her support and guidance throughout this project. Funding was provided by the Medical College of Wisconsin.
Conflict of interest
No authors have any conflicts of interest to report.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Buelow, M.W., Dall, A., Bartz, P.J. et al. Renal Dysfunction is Common Among Adults After Palliation for Previous Tetralogy of Fallot. Pediatr Cardiol 34, 165–169 (2013). https://doi.org/10.1007/s00246-012-0408-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-012-0408-3