
Abstract
Stress myocardial perfusion scintigraphy imaging (SMPSI) has important applications for evaluating coronary disease and ventricular function. Studies consistently focus on the left ventricle (LV), with no normal right ventricle (RV) data available. This study sought to evaluate the feasibility of RV perfusion with technetium (Tc-99m) sestamibi using a low radiotracer dose for children free of coronary artery (CA) anomalies and to determine its normal pattern. Patients with a history of Kawasaki disease who showed no coronary complications on selective angiography or no LV perfusion defects on SMPSI were studied at rest and during an exercise challenge. The RV uptake counts were compared with those for different segments of the LV, and multiple ratios of the uptakes between RV and LV segments were calculated. The study subjects were 23 children (age, 11.1 ± 3.3 years) imaged with 0.12 ± 0.03 mCi/kg at rest and 0.31 ± 0.06 mCi/kg during stress. The RV to LV uptake proportion was approximately 6%. Exercise-related uptake increased threefold in both the RV and the LV. The findings showed RV myocardial scintigraphy to be feasible with reproducible ratios. Potential clinical applications include acquired and congenital CA anomalies such as Kawasaki disease, right CA ostium stenosis after a switch operation, and anomalous origin of the right CA.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Stress myocardial perfusion scintigraphy imaging (SMPSI), is documented to be a sensitive method for detecting myocardial ischemia [19, 21, 23, 27, 29]. For pediatric patients, similar to adults, the interest of SMPSI studies investigating ischemic coronary disease is focused consistently on the left ventricle (LV). Myocardial ischemic disease in children with SMPSI has mainly been studied in patients with Kawasaki disease (KD) and anomalous origin of the left coronary artery (CA) from the pulmonary artery after an arterial switch for D-transposition of the great arteries [8, 11, 15, 22, 23, 39, 43].
The most frequent locations of CA aneurysms in KD are the proximal left anterior descending CA and the proximal right CA [23, 40]. Similarly, complications of the arterial switch in the transposition of the great arteries include right coronary ostia stenosis [7, 16, 25, 41]. Nevertheless, the literature has no specific data addressing evaluation of right ventricle (RV) perfusion by SMPSI in the pediatric population.
Because of the potential long-term deleterious effects resulting from exposure to radiation induced by nuclear imaging, a new radiotracer dose was suggested by the manufacturer based on a previous study (A Trial to Determine Radiation Exposure to Organs and Assess the Safety of Cardiolite in Pediatric Subjects) registered under www.clinicaltrials.gov (NCT00162045). Hence, this study had two aims: to evaluate the feasibility of RV imaging with a low radiotracer dose and to determine the normal patterns of RV perfusion imaging with technetium (Tc-99m) sestamibi single-photon emission computer tomography (SPECT) in children free of detectible CA anomalies.
Materials and Methods
Settings
An open-label, nonrandomized, international, multicenter phase 3 trial (A Study to Evaluate the Use and Safety of Cardiolite in Pediatric Patients With KD), hereafter called Cardiolite-301, is an industry-sponsored study on the myocardial perfusion scan in children with KD, registered under www.clincalgtrials.gov (NCT00162032). The study presented in this report was a single-site subanalysis determined by the local principal investigator (N.D.) focusing on the feasibility of RV myocardial perfusion detection.
The Cardiolite-301 study was conducted to evaluate myocardial perfusion imaging in patients with KD to predict the risk for the development of cardiac events related to CA sequelae after KD. The RV subanalysis was intended to evaluate the feasibility of imaging RV myocardial perfusion and to report the expected values in children without detectible CA sequelae.
Patients
The KD patients enrolled in the Cardiolite-301 study from our site were eligible for inclusion in this study if they presented no coronary aneurysm or stenosis as determined by serial echocardiography follow-up assessments and confirmed with a selective coronary angiography, and if the rest–stress Tc-99m sestamibi SPECT study of the LV was considered normal. All the SMPSI studies were conducted between September 2005 and October 2006.
All the patients underwent two-dimensional echocardiography at the onset of KD and at regular intervals later and were evaluated at the time of patient screening in the aforementioned study. All the patients had received rest and stress SPECT myocardial perfusion imaging and had been followed for 3 years afterward. The study was approved by the Sainte-Justine Institutional Review Board and Ethics Committee. Written informed consent was obtained from all the patients, parents, or legal guardians.
Rest and Treadmill Stress 99 mTc-Sestamibi SPECT
A same-day stress and rest Tc-99m sestamibi SPECT protocol was used, with the treadmill exercise constituting the stress modality. The rest SPECT study was performed first within 20 to 30 min after injection of Tc-99m MIBI (0.1–0.2 mCi/kg). Then 2–3 h later, a treadmill exercise stress challenge was performed according to the Bruce protocol [9]. The stress radiotracer dose (0.3 mCi/kg) was injected intravenously at peak treadmill stress. The patient was required to remain on the treadmill for 1 min after the injection, and SPECT-gated imaging acquisition was started 20 to 30 min after the injection. A rotating two-head SPECT gamma camera (128 × 128 pixels, 180°, 17 steps of 6°, 60 s/step) (Axis; Philips, Cleveland, OH, USA) was used for image acquisition.
The myocardial uptake image acquisition after the stress test was electrocardiography (ECG)-gated with an accepted heart rate variation of ±10%. The RV images were analyzed in a qualitative and semiquantitative manner. Data of the maximum counts in the different regions of interest were acquired by a single experienced operator (S.L.) blinded to the objectives of the study and to the patients’ clinical information. Qualitative image analysis was performed comparing the RV myocardium to the background ratio and the ability to delineate both the RV cavity and the myocardium in both exercise and resting states.
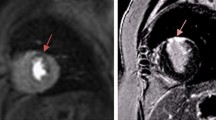
For semiquantitative analysis, the maximal stress and rest counts of the left and RVs were determined in the apical, mid, and basal short-axis and vertical long-axis views. Regions of interest were defined as the RV, the ventricular septum, and the LV anterior, lateral, and inferior walls. The RV count rate profile was determined across the middle long-axis tomographic slice where the RV was best visualized (Fig. 1). Multiple ratios between the RV and the LV were calculated with proportional stress and rest counts of the different regions of interest.

Regions of interest for semiquantitative analysis. Left panel Septum (1), LV lateral wall (2), and RV (3). Right panel LV anterior (1) and inferior (2) walls
Statistical Analysis
Data are expressed as mean ± standard deviation. The Kolmogorov–Smirnov normality test was applied to assess the normal distribution of the count rate profile ratios at stress and rest of the RV and the different regions of interest. A P value <0.05 indicates that the data varies significantly from the pattern expected, assuming that the population has a normal distribution.
Results
Patients
In the target population of 35 subjects, 27 met the selection criteria based on CA status. Focal LV regional myocardial perfusion defects were detected in 4 of the 27 subjects, and they were therefore excluded from analysis. The remaining 23 patients (16 boys and seven girls) were 11.1 ± 3.3 years old at the time of the study. The age at KD onset was 3.9 ± 1.9 years, and the interval between onset of KD and SMPSI was 7.1 ± 3.4 years. Selective right and left CA angiography and right and left hemodynamic evaluation were available for all the study patients within 0.04 ± 0.6 months before or after the SMPSI.
Of the 23 subjects, 19 had right coronary dominance, three had left dominance including one subject with a unique left CA, and one had co-dominant distribution. All the coronary angiography and hemodynamic study results were normal without evidence of coronary aneurysm, stenosis, interarterial course, or systolic or diastolic dysfunction.
Treadmill Stress Protocol
All the subjects had normal treadmill exercise stress test results (Table 1). The estimated energy expenditure was 13.5 ± 2.1 metabolic equivalents (METS), and the total stress duration was 11.0 ± 1.8 min. The maximum heart rate was 89 ± 5.6% predicted for age. Blood pressure at rest and peak exercise were within expected limits.
The stress test was limited by fatigue for all the subjects, with 20 (87%) of the 23 subjects achieving a peak heart rate exceeding 85% predicted for age. The remaining three patients were younger than 6 years and had no ST abnormalities or exercise-induced arrhythmias.
SMPSI RV Imaging
The administered rest and stress radiotracer doses were respectively 0.13 ± 0.03 and 0.32 ± 0.07 mCi/kg. For three patients, algorithms to correct movement artifacts were applied. Adequacy of qualitative imaging analyses of exercise and resting acquisition were considered optimal for all the patients. The ECG-gated LV wall motion and the ejection fraction were within the normal expected limits for all the subjects. For all the subjects, the RV imaging was considered appropriate for quantitative measurements, and no fixed lesions or ischemic changes in the RV or LV were identified by the blinded reporting radiologists.
Semiquantitative analysis of the RV showed a normal distribution for most of the count rate profile ratios at stress and at rest between the RV and LV regions of interest (Table 2). On the average, the ratio of the RV perfusion uptake represented approximately 6% of the LV uptake, and approximately 22–28% of the uptake of various LV segments and the interventricular septum. These ratios were stable among the study subjects (1.0–1.06) between the resting state and the exercise challenge, whereas the right or the LVs seemed to increase their perfusion requirements threefold (average, 2.9–3.0).
Discussion
From the feasibility standpoint, all the subjects were able to cooperate with the exercise stress protocol, and the majority achieved the target maximal heart rate expected for age. The effective dose of Tc-99m-sestamibi was half the previously recommended dose in clinical practice before this study [34]. Finally, the RV visualization and evaluation at stress and at rest in a quantitative or semiquantitative manner were feasible, with the low radiotracer dose dictated by the study protocol.
In the pediatric population, the evaluation of coronary ischemia with SMPSI has been studied mainly in conditions such as KD [11, 17, 19, 21, 23, 29, 32] after arterial switch surgical repair for transposition of the great arteries [22, 43, 44] and anomalous origin of the left CA from the pulmonary artery [8, 15, 39]. Other interesting applications include evaluation of the RV function in congenital cardiac anomalies with morphologic systemic RV [17, 28, 39], evaluation of the RV overload in vascular pulmonary hypertension [1, 34], and prognostic evaluation in hypertrophic cardiomyopathy and Duchenne muscular dystrophy [14, 20, 36].
As with adults, the main interest of SMPSI studies in the pediatric age group is focused consistently on LV perfusion. Perfusion of an obstructed right CA often is assumed by left CA collaterals and typically left untreated in adults. For children, however, whose remaining life span is longer than that of adults, efforts to preserve the native network of coronary arteries and to avoid a single CA physiology would potentially avert future mortality and morbidity events [18] such as arrhythmias or RV congestive failure. For instance, KD affects mainly preschool children [32]. The estimated risk of CA aneurysm is about 25% for untreated patients compared with 5% for those who receive appropriate treatment [10, 12, 24, 37].
To date, CA stenosis is best assessed invasively by coronary angiography, with its potential complications inherent to the invasive aspect of the technique such as CA spasm, arrhythmia, ST changes, and complications at the site of vascular access [40]. The SMPSI technique is documented to be a sensitive method for detecting left heart myocardial ischemia under exercise or pharmacologic challenge [19, 21, 23, 27, 29]. It is reported to correlate with echocardiographic findings of exercise-induced LV segmental contractile anomalies [11]. It also is part of the 2004 guidelines to detect coronary complications in high-risk patients during follow-up assessment [32]. We believe however, that special attention must be paid to RV perfusion when such tests are performed because the right CA represents 69% of occlusive lesions and 89% of segmental stenotic lesions [40]. Actually, CA intervention for KD-related CA stenosis equally involves the right and left CA segments. In a multicenter Japanese study, 54% of percutaneous catheter intervention addressed the right CA alone compared with 45% of the intervention that addressed the left CA alone [30]. According to the same study, 42% of the surgical series involved both right and left CA, and another 8% involved the right CA alone.
Other clinical situations equally important to highlight are congenital anomalies affecting the right CA circulation. The adequacy of the coronary blood flow after the arterial switch operation may cause CA stenosis in up to 7.8% of subjects, leading to patient demise in some cases [7, 16, 25, 41]. Such complications may occur as early as perioperatively or many years after the surgical intervention. Selective coronary angiography and coronary multislice computer tomography have been used for systematic screening. Besides the relatively high radiation exposure, multihead scanners may not provide optimal resolution for young children due to a physiologically accelerated heart rate. Due to the development of collaterals supplying the affected region, the exact role of imaging assessing coronary supply, including SMPSI, is yet to be defined [43].
The other type of congenital CA anomaly is the abnormal aortic origin of the CA [4, 6, 13, 26, 42, 45, 46]. Mechanisms precipitating death are triggered by myocardial ischemia, as suggested by pathologic evidence of acute myocardial damage [6, 26, 42]. Although such damage is thought to be confined solely to the left CA aberrant origin in the early reports [26], sudden cardiac death associated with abnormal origin of the right CA from the left coronary sinus was reported to be the second most frequently observed anomaly in a large autopsy series [42].
In another recent review article, 5 (28%) of 18 athletes had their right CA originating from the left aortic sinus [6]. One died suddenly; one required surgical correction; and one had an ischemic myocardial perfusion scintigraphy profile. We believe that in right CA anomalies, congenital or acquired, RV SMPSI may be a valuable method to assess the risk for exercise-related cardiac events such as subischemic states, the potential for secondary dilated cardiomyopathy, and the risk for sudden death.
It is ethically challenging to enroll totally healthy children in a similar study for the sole purpose of defining the normal relative myocardial perfusion. The relatively low number of subjects in our study may represent a methodologic limitation subsequent to the ethical dilemma. Nevertheless, the normal distribution of the SMPSI profile observed in most target ratios consolidates the reliability of our data. In this perspective, use of mean values and their standard deviations is appropriate when the data are normally distributed. Alternatively, the median value with the percentile range should be used when a particular patient is compared with the normal values drawn from our series.
From a technical standpoint, cardiac stress testing focuses mainly on LV evaluation, with well-established significance in the diagnosis and management of CA disease. The American Society of Echocardiography and other governing bodies have recently acknowledged the importance of assessing the RV function for both diagnostic and prognostic purposes [35]. A right coronary stenosis usually is suspected during stress echocardiography indirectly when contraction abnormalities of the LV inferior wall are present [5, 33]. This is due to the low yield of free RV wall imaging. Hence, direct stress echocardiography assessment for RV ischemic changes has been mostly qualitative, typically limited by challenges secondary to the complex geometry, kinetics, and often limited anatomic visualization of the RV. As a result, the studies assessing exercise-induced ischemic RV changes have been few and sometimes limited [5–47].
Several echocardiographic parameters such as RV wall motion [5], RV systolic pressure at stress [3], tricuspid annulus motion [2], and RV vector imaging [47] have been suggested. But the scarcity of quantitative data from both normal and pathologic states is a factor that limits widespread clinical application. Consequently, the available recommendations do not appear to be uniformly used or standardized [35]. Considering that effect, we believe our study provides valuable data for the ongoing efforts toward noninvasive RV and right CA evaluation. We acknowledge that the radiation-free nature, the higher specificity, and the lower cost of stress echocardiography are advantageous in general. On the other hand, the potential advantages of stress perfusion studies, including a higher technical success rate and sensitivity, should not be disregarded [38].
In conclusion, Tc-99 sestamibi SPECT imaging of the RV provides quality images with a low radiotracer dose and may represent a useful tool for evaluating RV perfusion in children. As we advance a few potential clinical applications for RV myocardial perfusion assessment, future studies involving cases with abnormal coronary flow to the RV are needed.
References
Akiba T, Yoshikawa M, Otaki S, Nakasato M, Suzuki H, Sato S, Sato T (1992) Estimation of right ventricular pressure in children by thallium-201 myocardial imaging using single-photon emission computed tomography. Am J Cardiol 69:673–676
Alam M, Samad BA (1999) Detection of exercise-induced reversible right ventricular wall motion abnormalities using echocardiographic determined tricuspid annular motion. Am J Cardiol 83:103–105, A8
Armstrong DW, Matangi MF (2010) Estimated right ventricular systolic pressure during exercise stress echocardiography in patients with suspected coronary artery disease. Can J Cardiol 26:e45–e49
Ayalp R, Mavi A, Serçelik A, Batyraliev T, Gümüsburun E (2002) Frequency of the anomalous origin of the right coronary artery with angiography in a Turkish population. Int J Cardiol 82:253–257
Bangalore S, Yao SS, Chaudhry FA (2007) Role of right ventricular wall motion abnormalities in risk stratification and prognosis of patients referred for stress echocardiography. J Am Coll Cardiol 50:1981–1989
Basso C, Maron BJ, Corrado D, Thiene G (2000) Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol 35:1493–1501
Bonnet D, Bonhoeffer P, Piéchaud JF, Aggoun Y, Sidi D, Planché C, Kachaner J (1996) Long-term fate of the coronary arteries after the arterial switch operation in newborns with transposition of the great arteries. Heart 76:274–279
Chen ML, Lo HS, Chao IM, Su HY (2007) Dipyridamole Tl-201 myocardial single photon emission computed tomography in the functional assessment of anomalous left coronary artery from the pulmonary artery. Clin Nucl Med 32:940–943
Cumming GR, Everatt D, Hastman L (1978) Bruce treadmill test in children: normal values in a clinic population. Am J Cardiol 41:69–75
Curtis N, Levin M (1998) Kawasaki disease thirty years on. Curr Opin Pediatr 10:24–33
Dahdah NS, Fournier A, Jaeggi E, van Doesburg NH, Lambert R, Dionne N, Sauvé C (1999) Segmental myocardial contractility versus perfusion in Kawasaki disease with coronary arterial aneurysm. Am J Cardiol 83:48–51
Dajani AS, Taubert KA, Gerber MA, Shulman ST, Ferrieri P, Freed M, Takahashi M, Bierman FZ, Karchmer AW, Wilson W (1993) Diagnosis and therapy of Kawasaki disease in children. Circulation 87:1776–1780
Davis JA, Cecchin F, Jones TK, Portman MA (2001) Major coronary artery anomalies in a pediatric population: incidence and clinical importance. J Am Coll Cardiol 37:593–597
Dilsizian V, Bonow RO, Epstein SE, Fananapazir L (1993) Myocardial ischemia detected by thallium scintigraphy is frequently related to cardiac arrest and syncope in young patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 22:796–804
Elhendy A, Zoet-Nugteren S, Cornel JH, Fioretti PM, Bogers AJ, Roelandt JR, Krenning E, Postma-Tjoa J, McGhie J, Spitaels SE (1996) Functional assessment of ALCAPA syndrome by dobutamine stress thallium-201 SPECT and echocardiography. J Nucl Med 37:748–751
El-Segaier M, Lundin A, Hochbergs P, Jögi P, Pesonen E (2010) Late coronary complications after arterial switch operation and their treatment. Catheter Cardiovasc Interv 76:1027–1032
Espinola-Zavaleta N, Alexanderson E, Attié F, Castellanos LM, Dueñas R, Rosas M, Keirns C (2004) Right ventricular function and ventricular perfusion defects in adults with congenitally corrected transposition: correlation of echocardiography and nuclear medicine. Cardiol Young 14:174–181
Frescura C, Basso C, Thiene G, Corrado D, Pennelli T, Angelini A, Daliento L (1998) Anomalous origin of coronary arteries and risk of sudden death: a study based on an autopsy population of congenital heart disease. Hum Pathol 29:689–695
Fukuda T, Ishibashi M, Yokoyama T, Otaki M, Shinohara T, Nakamura Y, Miyake T, Kudoh T, Oku H (2002) Myocardial ischemia in Kawasaki disease: evaluation with dipyridamole stress technetium 99m tetrofosmin scintigraphy. J Nucl Cardiol 9:632–637
Haley JH, Miller TD (2001) Myocardial ischemia on thallium scintigraphy in hypertrophic cardiomyopathy: predictor of sudden cardiac death. Circulation 104:E71–E71
Hamamichi Y, Ichida F, Tsubata S, Hirono K, Watanabe S, Rui C, Yu X, Uese K, Hashimoto I, Simizu M, Seto H, Origasa H, Miyawaki T (2002) Dobutamine stress radionuclide ventriculography reveals silent myocardial dysfunction in Kawasaki disease. Circ J 66:63–69
Hayes AM, Baker EJ, Kakadeker A, Parsons JM, Martin RP, Radley-Smith R, Qureshi SA, Yacoub M, Maisey MN, Tynan M (1994) Influence of anatomic correction for transposition of the great arteries on myocardial perfusion: radionuclide imaging with technetium-99m 2-methoxy isobutyl isonitrile. J Am Coll Cardiol 24:769–777
Kashyap R, Mittal BR, Bhattacharya A, Manojkumar R, Singh S (2011) Exercise myocardial perfusion imaging to evaluate inducible ischaemia in children with Kawasaki disease. Nucl Med Commun 32:137–141
Kato H, Sugimura T, Akagi T, Sato N, Hashino K, Maeno Y, Kazue T, Eto G, Yamakawa R (1996) Long-term consequences of Kawasaki disease: a 10- to 21-year follow-up study of 594 patients. Circulation 94:1379–1385
Legendre A, Losay J, Touchot-Koné A, Serraf A, Belli E, Piot JD, Lambert V, Capderou A, Planche C (2003) Coronary events after arterial switch operation for transposition of the great arteries. Circulation 108(Suppl 1):186–190
Liberthson RR, Dinsmore RE, Fallon JT (1979) Aberrant coronary artery origin from the aorta: report of 18 patients, review of literature and delineation of natural history and management. Circulation 59:748–754
Lim CW, Ho KT, Quek SC (2006) Exercise myocardial perfusion stress testing in children with Kawasaki disease. J Paediatr Child Health 42:419–422
Millane T, Bernard EJ, Jaeggi E, Howman-Giles RB, Uren RF, Cartmill TB, Hawker RE, Celermajer DS (2000) Role of ischemia and infarction in late right ventricular dysfunction after atrial repair of transposition of the great arteries. J Am Coll Cardiol 35:1661–1668
Miyagawa M, Mochizuki T, Murase K, Tanada S, Ikezoe J, Sekiya M, Hamamoto K, Matsumoto S, Niino M (1998) Prognostic value of dipyridamole-thallium myocardial scintigraphy in patients with Kawasaki disease. Circulation 98:990–996
Muta H, Ishii M (2010) Percutaneous coronary intervention versus coronary artery bypass grafting for stenotic lesions after Kawasaki disease. J Pediatr 157:120–126
Nadel HR, Stilwell ME (1998) Cardiopulmonary nuclear medicine in children. In: Freeman LM (ed) Nuclear Medicine Annual 1998. Lippincott-Raven Publishers, Philadelphia, pp 165–224
Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, Shulman ST, Bolger AF, Ferrieri P, Baltimore RS, Wilson WR, Baddour LM, Levison ME, Pallasch TJ, Falace DA, Taubert KA, Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association (2004) Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics 114:1708–1733
Picano E (2009) Stress echocardiography, 5th edn. Springer, Berlin, pp 105–123
Rabinovitch M, Fischer KC, Treves S (1981) Quantitative thallium-201 myocardial imaging in assessing right ventricular pressure in patients with congenital heart defects. Br Heart J 45:198–205
Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB (2010) Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 23:685–713
Scopinaro F, Manni C, Miccheli A, Massa R, De Vincentis G, Schillaci O, Ierardi M, Danieli R, Banci M, Iorio F (1996) Muscular uptake of Tc-99m MIBI and TI-201 in Duchenne muscular dystrophy. Clin Nucl Med 21:792–796
Senzaki H (2008) Long-term outcome of Kawasaki disease. Circulation 118:2763–2772
Sicari R, Nihoyannopoulos P, Evangelista A, Kasprzak J, Lancellotti P, Poldermans D, Voigt JU, Zamorano JL, European Association of Echocardiography (2009) Stress Echocardiography Expert Consensus Statement–Executive Summary: European Association of Echocardiography (EAE) (a registered branch of the ESC). Eur Heart J 30:278–289
Stern H, Sauer U, Locher D, Bauer R, Meisner H, Sebening F, Bühlmeyer K (1993) Left ventricular function assessed with echocardiography and myocardial perfusion assessed with scintigraphy under dipyridamole stress in pediatric patients after repair for anomalous origin of the left coronary artery from the pulmonary artery. J Thorac Cardiovasc Surg 106:723–732
Suzuki A, Kamiya T, Kuwahara N, Ono Y, Kohata T, Takahashi O, Kimura K, Takamiya M (1986) Coronary arterial lesions of Kawasaki disease: cardiac catheterization findings of 1,100 cases. Pediatr Cardiol 7:3–9
Tanel RE, Wernovsky G, Landzberg MJ, Perry SB, Burke RP (1995) Coronary artery abnormalities detected at cardiac catheterization following the arterial switch operation for transposition of the great arteries. Am J Cardiol 76:153–157
Taylor AJ, Rogan KM, Virmani R (1992) Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 20:640–647
Vogel M, Smallhorn JF, Gilday D, Benson LN, Ash J, Williams WG, Freedom RM (1991) Assessment of myocardial perfusion in patients after the arterial switch operation. J Nucl Med 32:237–241
Weindling SN, Wernovsky G, Colan SD, Parker JA, Boutin C, Mone SM, Costello J, Castañeda AR, Treves ST (1994) Myocardial perfusion, function, and exercise tolerance after the arterial switch operation. J Am Coll Cardiol 23:424–433
Wilkins CE, Betancourt B, Mathur VS, Massumi A, De Castro CM, Garcia E, Hall RJ (1988) Coronary artery anomalies: a review of more than 10,000 patients from the Clayton Cardiovascular Laboratories. Tex Heart Inst J 15:166–173
Yamanaka O, Hobbs RE (1990) Coronary artery anomalies in 126, 595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 21:28–40
Yang HS, Mookadam F, Warsame TA, Khandheria BK, Tajik JA, Chandrasekaran K (2010) Evaluation of right ventricular global and regional function during stress echocardiography using novel velocity vector imaging. Eur J Echocardiogr 11:157–164
Acknowledgments
This study was a site-specific subanalysis from a large multinational industry-sponsored study. Dr. Velasco-Sanchez is supported by two unrestricted grants provided by the LaCaixa Foundation, Spain, and the Sainte-Justine Hospital Foundation, Montreal, Canada.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Velasco-Sanchez, D., Lambert, R., Turpin, S. et al. Right Ventricle Myocardial Perfusion Scintigraphy: Feasibility and Expected Values in Children. Pediatr Cardiol 33, 295–301 (2012). https://doi.org/10.1007/s00246-011-0128-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-011-0128-0