
Abstract
Clinical trials are abundant in adult cardiovascular medicine; however, they are rare in pediatric cardiology. Pediatric cardiac trial design may be impacted by the heterogeneous nature of the underlying cardiac defects, as well as by a strong emotional response from parents whose child will undergo a surgical intervention. The purpose of this study was to assess factors that may have an impact on parents considering enrollment of their child in a clinical trial at the time of surgical intervention. A voluntary, self-administered questionnaire (14 questions) was provided to parents of children 16 years of age or younger during the preadmission testing period. Demographic and procedure-related variables were collected for each patient. A total of 119 surveys were analyzed over a 1.5-year period. Only 8% of the parents had their child participate in a clinical trial in the past. Fifty-six percent of the parents preferred that their child’s cardiologist or surgeon explain clinical trial details, with 23% preferring the principal investigator and 3% preferring the research coordinator. Fifty percent of the parents were favorably disposed to participate in a clinical trial if the drug or device was currently used by their child’s doctor, and 19% were encouraged to participate if the drug or device was approved for use in adults. The majority of parents (64%) preferred to be asked about participating in a trial within 1 month prior to the planned procedure, and 40% preferred to discuss trial details at a remote time in an outpatient location. Sixty-three percent of parents believed that most of the medications currently used in children were already approved by the Food and Drug Administration. Most parents (91%) believed that clinical trials conducted in children will help improve pediatric health care; 74% believed that their child may receive potential benefit from enrolling in a trial. Finally, 43% believed that funding for trials should come from government and health care agencies, as opposed to pharmaceutical companies (24%). This survey reveals the importance of the attending physician and timing in educating parents regarding a cardiac critical care clinical trial. These data may impact the design and successful conduct of future trials.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Adult cardiovascular trials are abundant; however, pediatric cardiovascular clinical trials are rare. Pediatric studies present a challenge to the medical community, industry, and the guardians and children [1, 4, 10]. Pediatric cardiac trial design may be impacted by the heterogeneous patient population with a multitude of underlying cardiac defects. Additionally, many patients receive a surgical intervention that may elicit a strong parental emotional response at the time of potential trial enrollment.
The purpose of this study was to assess factors that may impact parents who are considering enrolling their child in a clinical trial at the time of surgical intervention. The factors considered included the parents’ prior experience with clinical trials, assessing by whom and where they would like to be approached concerning a trial, and understanding their current opinion about clinical trials.
Materials and Methods
A 14-question survey was used that was voluntary and self-administered. This study was approved by the Columbus Children’s Hospital institutional review board. The parents of children 16 years of age or younger were approached during preadmission testing for a surgical intervention from March 2003 to October 2004. Demographic and procedure-related variables were collected for all patients for whom a survey was completed. The study was designed to include only those coming electively for surgical intervention, therefore excluding all inpatients, which thus excluded some neonates with critical congenital heart disease.
The survey included several sections encompassing the following: (1) basic information and previous experience with research, (2) knowledge and opinion about research, and (3) approach of the parent for clinical trial participation. The study questions are outlined in Table 1.
Results
There were 119 respondents (29 male and 90 female) with a 40% completion rate. Of those, 72% of the parents were married, 18% were single, and 10% were separated or divorced. Ninety-four percent of the respondents had health insurance. Of the 119 respondents, 8% had a child participate in a clinical trial previously, and 11% knew of someone who had previously participated in a clinical trial.
Using the Food and Drug Administration (FDA) age groupings, the patients included 1% less than 1 month of age, 48% between 1 month and 2 years of age, 39% between 2 and 12 years of age, and 12% between 12 and 16 years of age. There were several highly represented physiologic categories, which included 35% with left-to-right shunts (congestive heart failure), 15% single ventricle physiology, 9% cyanotic heart disease, 9% aortic valve disease, and 8% mitral valve disease. Many conditions that did not involve the aforementioned physiologic states represented small percentages yet totaled 24% of the population. Eighty-four percent presented for a biventricular repair, whereas 16% presented for a single ventricle palliation. The majority of patients (58%) were on preoperative medications, and 41% had a previous cardiac operation.
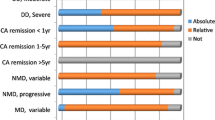
Respondents’ answers to Section 2 of the survey are represented in Table 2. Figure 1 represents the responses to question 11, and Fig. 2 represents the answers to question 13. Fifty percent of the respondents felt more comfortable enrolling their child in a trial that involves a drug or device currently used in their physician’s practice, whereas 19% were encouraged by a drug or device approved in adults, 9% by a drug or device tested in adults, and 2% by a drug or device tested in animals. Twenty percent of the respondents did not know. Approximately 40% of the respondents felt most comfortable discussing details about a trial in the outpatient clinic at a time remote from the planned procedure, whereas 18% preferred the intensive care unit periprocedure and 11% preferred the clinic periprocedure. Thirty-one percent of the respondents did not know.

Percentage responses to the question, “Who would you most prefer to explain a clinical trial?”

Percentage responses to the question, “When is the best time to ask about a clinical trial involving the use of a drug or device around the time of surgery?”
Discussion
Many relatively recent acts of regulation by the FDA have attempted to stimulate drug trials in children. The Food and Drug Administration Modernization Act (FDAMA) enacted in November 1997 specifically addressed pediatric drug trials and also provided impetus to sponsors to complete trials by providing 6 months of extended market exclusivity [5]. Under the U.S. Food, Drug, and Cosmetic Act of 1999, regulations were set to industry for new drugs anticipated for pediatric use. Not only was early planning of trials for the particular drug encouraged but also a requirement for studying and labeling these drugs for pediatric use was established. The Best Pharmaceuticals for Children Act, enacted into law in 2002, in essence renewed the exclusivity previously enacted in 1997 under FDAMA [3]. This act also detailed public posting of results of trials and ensured reporting of adverse events for 1 year after exclusivity was granted. In 2003, the Pediatric Research Equity Act provided the FDA the authority to require the study of drugs for the pediatric population to ensure safety [8]. Despite these governmental acts, pediatric cardiac critical care trials are still rare. In order to optimize enrollment in these studies, the cardiac intensive care community must ascertain a parent’s view of clinical trials and address obstacles facing investigators.
Our study examined parental views of several key elements to pediatric cardiac critical care research. Basic knowledge and experience with research was limited. Very few respondents had their child participate (8%) or knew of someone who had participated (11%) in a clinical trial previously. Almost two-thirds of the respondents believed that most medicines used in pediatrics were approved by the FDA for use in children. Despite this lack of experience and misunderstanding of FDA-approved medications, the overwhelming majority (91%) of respondents believed that clinical trials will help improve pediatric care, and 74% believed that by enrolling their child in a trial, the participant may receive a medicine or device that could be of benefit. In a recent study of 34 parents of neonates with congenital heart disease, 53% stated societal benefit and 47% stated individual benefit for their infant were factors in determining participation in research [7]. One may conclude that despite a lack of experience with trials, there is enthusiasm for research from parents of patients with heart disease.
The approach to parents may be one of the most vital aspects of successful enrollment in pediatric research [2, 6, 9, 11, 12]. The majority of parents believed that being approached about a clinical trial by the patient’s primary pediatric cardiologist or cardiothoracic surgeon was most desirable as opposed to being approached by the principal investigator or the research coordinator. Comfort likely plays a significant role in this process; however, as with any study, one has to guard against coercion. It is thus imperative that a coordinated approach of all responsible researchers ensures that the family is well informed and the consent process is without bias. The primary cardiologist or cardiothoracic surgeon will have to be responsible and familiar with all protocols if he or she is to approach families concerning clinical trials in an unbiased and informative manner.
The majority of respondents were interested in discussing a cardiac critical care trial at least 1 month prior to the planned procedure. Very few respondents were interested in discussing the trial even within 2 days of the planned event. Approximately 40% of the respondents wanted to discuss the trial in the clinic at a remote time from the planned procedure, 19% preferred the intensive care unit at the time of the planned procedure, and 11% preferred the clinic at approximately the time of the planned procedure. Although this represents diverse responses, it seems that slightly more than half of the parents prefer to discuss the trial in the clinic. This finding emphasizes the need for advanced education potentially through physician–parent interaction, literature, or Internet link availability.
This survey study has limitations, including a 40% completion rate. Additionally, the study design excluded inpatients; therefore, parents of neonates awaiting congenital heart disease surgery during initial hospitalization are not represented. However, in order to have the subjects each experience a relatively uniform process, those having a child undergo preadmission testing as an outpatient were studied. Finally, socioeconomic and education status of the parents was not assessed.
Conclusions
This study may impact the design and conduct of future pediatric cardiac critical care trials. Through appropriate education of parents via proactive and comfortable communication in an appropriate venue, cardiac critical care trials in children may be facilitated even during emotionally stressful hospitalizations. Finally, it may be helpful to create a multicenter design for this survey to assess regional differences and evaluate multiple factors that could eventually lead to the formation of a model of trial characteristics and execution that leads to optimal enrollment.
References
Ackerman TF (2001) The ethics of drug research in children. Paediatr Drugs 3:29–41
Barfield RC, Church C (2005) Informed consent in pediatric clinical trials. Curr Opin Pediatr 17:20–24
Best Pharmaceuticals for Children Act (2002). Public Law 107–109
Caldwell PH, Murphy SB, Butow PN, Craig JC (2004) Clinical trials in children. Lancet 364:803–811
Food and Drug Administration Modernization Act of 1997. Public Law 105–115
Hoehn KS, Nelson RM (2004) Advising parents about children’s participation in clinical research. Pediatr Ann 33:778–781
Hoehn KS, Wernovsky G, Rychik J, et al. (2005) What factors are important to parents making decisions about neonatal research? Arch Dis Childhood Fetal Neonatal Ed 90:F267–F269
Pediatric Research Equity Act of 2003. Public Law 108–155
Rothmier JD, Lasley MV, Shapiro GG (2003) Factors influencing parental consent in pediatric clinical research. Pediatrics 111:1037–1041
Salazar JC (2003) Pediatric clinical trial experience: government, child, parent and physician’s perspective. Pediatr Infect Dis J 22:1124–1127
Tait AR, Voepel-Lewis T, Malviya S (2003) Participation of children in clinical research: factors that influence a parent’s decision to consent. Anesthesiology 99:819–825
Tait AR, Voepel-Lewis T, Siewert M, Malviya S (1998) Factors that influence parents’ decisions to consent to their child’s participation in clinical anesthesia research. Anesth Analg 86:50–53
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hoffman, T., Taeed, R., Niles, J. et al. Parental Factors Impacting the Enrollment of Children in Cardiac Critical Care Clinical Trials. Pediatr Cardiol 28, 167–171 (2007). https://doi.org/10.1007/s00246-006-0020-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-006-0020-5