
Abstract
Our objectives were to compare measurements of ureteral wall area, ureteral wall volume and ureteral wall thickness for their use in prediction of shock wave lithotripsy outcomes. We retrospectively identified 218 patients that underwent shock wave lithotripsy for ureteral calculi with pretreatment non-contrast computed tomography. We measured ureteral wall thickness, ureteral wall area and ureteral wall volume by high functional viewer. Ureteral wall thickness was defined as the maximum thickness of ureteral wall, and ureteral wall area as the area of ureteral wall around the stone in the maximal stone diameter on axial computed tomography image. Ureteral wall volume was defined as the volume of ureteral wall from the upper to lower edge of the stone. Treatment success was defined as absence of residual fragments within 3 months after the first session. We compared the outcome predictive power among these parameters and logistic regression analysis to identify factors contributing to treatment failure. The treatment success rate was 47.6%. Ureteral wall thickness, ureteral wall area and ureteral wall volume in successful cases were all significantly smaller than those in unsuccessful cases (all p < 0.01). Area under curve of ureteral wall volume was the largest of these parameters and significantly larger than that of ureteral wall thickness (p < 0.01). On multiple logistic regression analysis, ureteral wall volume was the only significant independent predictor of treatment outcome. Ureteral wall volume is a better predictor of shock wave lithotripsy outcome than ureteral wall thickness or ureteral wall area.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Extracorporeal shock wave lithotripsy (SWL) remains one of the most important treatment options in urology because of its safety and low invasiveness, despite remarkable development of endoscopic technology in recent years. Many studies, however, have shown that SWL has a lower treatment success rate than ureteroscopy (URS) or percutaneous nephrolithotomy (PCNL) [1]. It is, therefore, important to identify predictors of SWL outcome and to ascertain the optimum treatment for patients with urolithiasis.
While various factors, including stone size, stone location, numbers of stones, skin-to-stone distance (SSD) and mean stone density (MSD), have been identified as predictors of SWL outcome [2,3,4,5,6,7], ureteral wall thickness (UWT) measured at the site ureteral stone by non-contrast computed tomography (NCCT) has been reported as a new noteworthy predictor of SWL outcome [8]. In addition, wide UWT is reportedly associated with a higher risk of impacted stones and poor endoscopic findings [9].
A method of measuring UWT, to our knowledge, has not yet been established. In previous studies, UWT was defined as the maximum thickness at the stone site according to axial NCCT images [8, 9]. However, thickening of ureteral wall around the entire stone cannot be evaluated by this definition. In the present study, the ureteral wall area (UWA) around the stone at the maximal diameter on axial NCCT image and ureteral wall volume (UWV) were measured around the entire stone in addition to UWT. Paying attention to the predictive powers of SWL outcome, these measurements were compared.
Materials and methods
Patients
After obtaining institutional review board approval (approval number 1887), we retrospectively reviewed the records of consecutive patients who underwent SWL for their radiopaque ureteral calculi at the Wakayama Medical University Hospital between January 2008 and January 2016. Of these 218 patients, 84 patients were excluded because pretreatment NCCT was not performed, and the remaining 134 patients were enrolled in this study. All subjects underwent pre-treatment regular NCCT (5 mm collimation width using a LightSpeed 64-slice multidetector helical CT scanner at 0.5 s per rotation, 120 kV and 100 mA). All participants gave written informed consent prior to the study.
SWL procedures
SWL treatments were performed using Lithotripter S (Dornier MedTech, Germany). All physicians performed SWL after receiving specific technical training. All patients underwent up to a maximum of 4000 shocks with a gradual augmentation of power at 70 shocks per minute. Shock-wave intensity was left to the physician’s judgement. They decided the number of shocks and the used intensity based on the efficiency of lithotripsy and the patients’ ability to continue through the pain. During treatment, stones were targeted with fluoroscopy at regular intervals.
Predictors
Patient demographics and clinical data were retrospectively collected from patient medical records. Patient demographics included patient age and sex, and clinical data included stone side (right or left), stone location (proximal, middle or distal ureter), stone number (single or multiple), stone volume, MSD, SSD, hydronephrosis, urinary drainage, UWT, UWA and UWV. UWT was defined as the maximum thickness of ureteral wall in the maximal stone diameter on axial NCCT image (Fig. 1). UWA was defined as the area of ureteral wall around the stone in the maximal diameter on axial NCCT image (Fig. 2a). UWV was defined as the volume of ureteral wall from the upper edge to the lower edge of the stone (Fig. 2b, c). UWA and UWV were evaluated using Aquarius iNtuition Viewer (TeraRecon, Inc., USA) as well as stone volume and MSD. We defined stones as lesions ≥ 100 HU as described in the previous study [10]. The details of measuring methods for stone volume, MSD, UWA and UWV were as follows: (1) we made a digitizing free-hand trace of the ureteral wall edge on each axial NCCT image from upper edge to the lower edge of the stone using Aquarius iNtuition Viewer (2). We clicked the “extraction” button after setting the threshold value at ≥ 100 HU; then stone volume and MSD were calculated (3). We clicked the “extraction” button after setting the threshold value at < 100 HU; then UWA and UWV were calculated. SSD was defined as the mean vertical distance from the center of the stone to the skin measured on axial NCCT image at 0°, 45° and 90° as suggested by Pareek et al. [5]. All measurements were performed using the abdominal window by a well-trained radiologist who was blinded to the treatment outcome. Urinary drainage was defined as the pretreatment placement of ureteral stent or nephrostomy tube.

Example of non-contrast computed tomography (NCCT) image demonstrating ureteral wall thickness (UWT). UWT was defined as the maximum thickness of ureteral wall in the maximal stone diameter on axial NCCT image. UWT in this example case was 7.14 mm

Example of measurement of a ureteral wall area (UWA) and (b: coronal image and c: sagittal image) ureteral wall volume (UWV) using Aquarius iNtuition Viewer. UWA was defined as the area of ureteral wall around the stone in the maximal diameter on axial NCCT image. UWV was defined as the volume of ureteral wall from the upper edge to the lower edge of the stone
Outcomes
Patients were evaluated by kidney, ureter, and bladder radiographs and ultrasonography a few weeks after the first SWL session. If sufficient treatment effect was not obtained (i.e. not fragmented at all, too large fragments for spontaneous passage or ‘stone street’ [steinstrasse] with fragments), patients underwent a second SWL session on the same day. In cases where sufficient treatment effect was successfully obtained, SWL outcome was determined using NCCT within 3 months after the first SWL session and treatment success was defined as the absence of residual fragments. Patients who required additional SWL sessions or adjunctive treatment (URS, PCNL, ureteral stenting or nephrostomy tube placement) were classified as unsuccessful cases.
Statistical analyses
Patient demographics and clinical data were compared using the Chi square tests or Mann–Whitney U tests of successful and unsuccessful cases. Receiver operating characteristic (ROC) curves were constructed to compare the predictive powers for SWL outcomes between UWT, UWA and UWV. Univariate and multiple logistic regression analyses were performed to identify factors that contributed to treatment failure. All statistical analyses were performed using JMP Pro 13 (SAS Institute, USA) and p < 0.05 was considered statistically significant.
Results
Of the 134 patients, 66 (49.3%) were classified as successful cases and 68 patients (50.7%) as unsuccessful cases. Comparison of patient characteristics and stone parameters between the two groups are shown in Table 1. Significantly different factors between these groups included age (p = 0.04), stone volume (p = 0.04) and urinary drainage (p = 0.03). Compared to the patients in unsuccessful group, the patients in the successful group were significantly young and had smaller stone volume and lower percentage of urinary drainage.
Table 2 shows the comparison of UWT, UWA and UWV between successful and unsuccessful cases. UWT, UWA and UWV in cases where SWL was successful were all significantly larger than those in cases where SWL was unsuccessful (all p < 0.01).
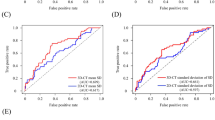
Figure 3 shows the ROC curves of UWT, UWA and UWV for prediction of SWL outcomes. Area under curve (AUC) of UWT, UWA and UWV were 0.636, 0.693 and 0.803, respectively (Table 3). AUC of UWV was the largest of these parameters and significantly larger than that of UWT (p < 0.01). ROC analysis showed that UWV of 73.4 mm3 was the optimal cutoff value predictive of SWL outcome after the first session. This cutoff had a sensitivity of 63.2% and specificity of 86.4% in predicting SWL outcome after the first session.

Receiver operating characteristics of radiographic parameters associated with ureteral wall. ROC analysis showed that UWV of 73.4 mm3 was the optimal cutoff value predictive of SWL outcome after the first session. This cutoff had a sensitivity of 63.2% and specificity of 86.4% in predicting SWL outcome after first session
Table 4 shows the results of univariate and multiple logistic regression analyses of various parameters that predict SWL failure after the first session. In univariate analysis, higher age (p = 0.030), multiple stones (p = 0.04), urinary drainage (p = 0.033) and thicker UWV (p < 0.001) were associated with treatment failure. On multiple analysis, thicker UMV was the only significant independent predictor of treatment failure (p < 0.001).
Discussion
In the present study, we focused on the methods of evaluation of thickening of ureteral walls at the site of stones. Our results revealed that the volumetric parameter of ureteral wall at the stone site, namely UWV, was a critical factor for SWL outcome compared with UWT and UWA.
When ureteral stones stay in the same position for a certain period, these stones, namely impacted stones, could cause surrounding chronic inflammation, interstitial fibrosis, ureteral epithelial hypertrophy, ureteral edema and polyps [11, 12]. These features of impacted stones can reportedly lead to the failure of spontaneous passage or SWL [11, 13,14,15]. In addition, ureteral stone impaction has been reported to be associated with ureteral perforation and ureteral stricture after URS [16]. It is, therefore, important to evaluate the risk of stone impaction before expectant management for spontaneous passage or stone removal operation.
There are several definitions of impacted stones, but several issues have been raised with regard to these definitions [9]. One definition is a stone staying at the same position in the ureter for more than 2 months, but we cannot accurately measure the period of impaction in the ureter because the initial day of impaction is unknown. A second definition is the failure of visualization of the ureter distal to the stone on intravenous urography (IVU) or computed tomographic urography (CTU), but neither IVU nor CTU is routinely performed in clinical practice because some patients are unable to receive contrast medium because of allergies or renal disorder. A third definition is the inability to pass a guidewire or catheter beyond the stone on the initial attempt [8, 11, 17], but it is impossible to determine whether a guidewire or catheter can pass through the stones without fluoroscopic treatment.
Recently, several studies have reported the usefulness of UWT based on NCCT as an indicator of impacted stones. Yoshida et al. reported that high UWT was associated with higher risk of impacted stone, poor endoscopic findings and adverse surgical outcomes in patients who underwent URS for their ureteral stones [9]. Moreover, Sarica et al. reported that high UWT at the ureteral stone site was an important predictor for SWL failure [8]. In both studies, UWT was defined as the maximum thickness at the stone site on axial NCCT image. However, which measuring method is appropriate for evaluating thickening of the ureteral wall remains unknown. We hypothesize that volumetric evaluation of ureteral wall, namely UWV, is more suitable for evaluation than UWT because it can represent thickening of the ureteral wall around the entire stone.
The current study suggests that UWV can be a critical predictor of SWL outcomes. In comparison with UWT and UWA, UWV has stronger predictive power of SWL outcomes than other parameters (Table 3). Moreover, in multiple logistic regression analysis, higher UWV is an independent significant predictor of SWL failure (p < 0.001). These results suggest that evaluation of the entire ureteral wall thickness around the stone is important for predicting SWL outcome. Although UWT can be simply used in clinical practice, we speculate that UWT has certain problems because it represents the thickness of ureteral wall at only one site. One problem is that it is possible that the ureteral wall around stones is extended and UWT tends to be low in patients with large axial diameter stones. A second problem is that it is difficult to evaluate the thickening of the ureteral wall in a direction perpendicular to the ureter by single axial image, especially in middle or distal ureter. On the other hand, UWV could overcome these problems because it can three-dimensionally represent the thickening of the ureteral wall around the entire stones. The results of subgroup analysis according to stone size (divided by median stone axial diameter, 6.5 mm) and stone location (proximal, middle and distal ureter) have shown that UWV in cases where SWL is successful is significantly higher than that in cases where it is unsuccessful and AUC of UWV is larger than that of UWT, regardless of stone size and location (Tables 5, 6).
Several limitations of our study should be acknowledged. This was a retrospective study with relatively small cohort. Second, the timing of evaluating the SWL outcome was inconsistent, although all participants received NCCT within 3 months after the first SWL session. A final limitation is that there is no evidence that 100 HU is the most appropriate cut-off CT attenuation value for distinguishing the ureteral wall and stones. However, the previous study demonstrated that substances with ≥ 100 HU in the human body are generally bone, calculus and calcification only, and 100 HU can be used as the cut-off CT attenuation value for extracting three-dimensional stone images [10]. Despite these limitations, the present study is the first to show that the volumetric evaluation of ureteral wall at the stone site, namely UWV, is more important in predicting SWL outcomes than UWT. We believe that our results will contribute to future development of nomograms or scoring systems for predicting SWL outcome.
Conclusions
UWV at the ureteral stone site can be considered to be a better predictor for outcome of SWL than UWT or UWA. UWV may be a novel useful pretreatment parameter in the decision process for patients about their treatment options.
Abbreviations
- SWL:
-
Shock wave lithotripsy
- URS:
-
Ureteroscopy
- PCNL:
-
Percutaneous nephrolithotomy
- SSD:
-
Skin-to-stone distance
- MSD:
-
Mean stone density
- UWT:
-
Ureteral wall thickness
- NCCT:
-
Non-contrast computed tomography
- UWA:
-
Ureteral wall area
- UWV:
-
Ureteral wall volume
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under curve
- IVU:
-
Intravenous urography
- CTU:
-
Computed tomographic urography
References
Wolf JS Jr (2007) Treatment selection and outcomes: ureteral calculi. Urol Clin N Am 34(3):421–430. https://doi.org/10.1016/j.ucl.2007.04.010
El-Nahas AR, El-Assmy AM, Mansour O, Sheir KZ (2007) A prospective multivariate analysis of factors predicting stone disintegration by extracorporeal shock wave lithotripsy: the value of high-resolution noncontrast computed tomography. European urology 51(6):1688–1693. https://doi.org/10.1016/j.eururo.2006.11.048(discussion 1693–1684)
Gupta NP, Ansari MS, Kesarvani P, Kapoor A, Mukhopadhyay S (2005) Role of computed tomography with no contrast medium enhancement in predicting the outcome of extracorporeal shock wave lithotripsy for urinary calculi. BJU Int 95(9):1285–1288. https://doi.org/10.1111/j.1464-410X.2005.05520.x
Kanao K, Nakashima J, Nakagawa K, Asakura H, Miyajima A, Oya M, Ohigashi T, Murai M (2006) Preoperative nomograms for predicting stone-free rate after extracorporeal shock wave lithotripsy. J Urol 176(4 Pt 1):1453–1456. https://doi.org/10.1016/j.juro.2006.06.089(discussion 1456–1457)
Pareek G, Hedican SP, Lee FT Jr, Nakada SY (2005) Shock wave lithotripsy success determined by skin-to-stone distance on computed tomography. Urology 66(5):941–944. https://doi.org/10.1016/j.urology.2005.05.011
Wiesenthal JD, Ghiculete D, Honey RJDA, Pace KT (2010) Evaluating the importance of mean stone density and skin-to-stone distance in predicting successful shock wave lithotripsy of renal and ureteric calculi. Urol Res 38(4):307–313. https://doi.org/10.1007/s00240-010-0295-0
Yoshida S, Hayashi T, Ikeda J, Yoshinaga A, Ohno R, Ishii N, Okada T, Osada H, Honda N, Yamada T (2006) Role of volume and attenuation value histogram of urinary stone on noncontrast helical computed tomography as predictor of fragility by extracorporeal shock wave lithotripsy. Urology 68(1):33–37. https://doi.org/10.1016/j.urology.2006.01.052
Sarica K, Kafkasli A, Yazici O, Cetinel AC, Demirkol MK, Tuncer M, Sahin C, Eryildirim B (2015) Ureteral wall thickness at the impacted ureteral stone site: a critical predictor for success rates after SWL. Urolithiasis 43(1):83–88. https://doi.org/10.1007/s00240-014-0724-6
Yoshida T, Inoue T, Omura N, Okada S, Hamamoto S, Kinoshita H, Matsuda T (2017) Ureteral wall thickness as a preoperative indicator of impacted stones in patients with ureteral stones undergoing ureteroscopic lithotripsy. Urology 106:45–49. https://doi.org/10.1016/j.urology.2017.04.047
Yamashita S, Kohjimoto Y, Iwahashi Y, Iguchi T, Iba A, Nishizawa S, Hara I (2018) Three-dimensional mean stone density measurement is superior for predicting extracorporeal shock wave lithotripsy success. Int J Urol. https://doi.org/10.1111/iju.13827
Morgentaler A, Bridge SS, Dretler SP (1990) Management of the impacted ureteral calculus. J Urol 143(2):263–266
Dretler SP, Young RH (1993) Stone granuloma: a cause of ureteral stricture. J Urol 150(6):1800–1802
Mugiya S, Ito T, Maruyama S, Hadano S, Nagae H (2004) Endoscopic features of impacted ureteral stones. J Urol 171(1):89–91. https://doi.org/10.1097/01.ju.0000100960.08768.81
Mueller SC, Wilbert D, Thueroff JW, Alken P (1986) Extracorporeal shock wave lithotripsy of ureteral stones: clinical experience and experimental findings. J Urol 135(4):831–834
Chaussy CG, Fuchs GJ (1989) Current state and future developments of noninvasive treatment of human urinary stones with extracorporeal shock wave lithotripsy. J Urol 141(3 Pt 2):782–789
Roberts WW, Cadeddu JA, Micali S, Kavoussi LR, Moore RG (1998) Ureteral stricture formation after removal of impacted calculi. J Urol 159(3):723–726
Deliveliotis C, Chrisofos M, Albanis S, Serafetinides E, Varkarakis J, Protogerou V (2003) Management and follow-up of impacted ureteral stones. Urol Int 70(4):269–272. https://doi.org/10.1159/000070133
Acknowledgements
This document was proof-read and edited by Benjamin Phillis at the Clinical Research Center, Wakayama Medical University.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest. No competing financial interests exist
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yamashita, S., Kohjimoto, Y., Iguchi, T. et al. Ureteral wall volume at ureteral stone site is a critical predictor for shock wave lithotripsy outcomes: comparison with ureteral wall thickness and area. Urolithiasis 48, 361–368 (2020). https://doi.org/10.1007/s00240-019-01154-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-019-01154-w