
Abstract
The purpose of our study is to analyze the definitive relation of C-reactive protein (CRP) and other factors with the spontaneous stone passage in patients with distal ureteric calculus of 5–10 mm and to calculate the risk of failure of expectant management in patients. 185 patients of ureteric colic, who were subjected to medical expulsive therapy (MET), were included prospectively from August 2016 to May 2018 and followed up for 4 weeks. Patients were divided into two groups. Group A included successful spontaneous passage patients and group B included failure in the same. The parameters analyzed were age, gender, longitudinal and transverse diameter of stone, CRP, total leucocyte count, ureteric diameter and hydroureteronephrosis (HUN). We performed univariate and multivariate analysis. Receiver operating characteristics curve was used to determine the cutoff value for significantly associated variables. 122 (65.90%) and 63 (34.10%) patients were included in group A and B, respectively. In univariate analysis, CRP, longitudinal and transverse diameter of stone, HUN, proximal and distal ureteric diameters were statistically significant. However, in multivariate analysis, only negative CRP (p = 0.002), smaller longitudinal diameter of stone (p < 0.001) and absence of HUN (p = 0.005) were significantly associated with successful expulsion. Cutoff for CRP was 0.41 mg/dl and longitudinal diameter was 6.7 mm. The success rate in the group of patients with no risk factor was 96.7% and with all three risk factors was 16.7%. Patients with a longitudinal diameter of stone > 6.7 mm, HUN, and CRP > 0.41 mg/dl should be considered for early intervention. The success rate of MET can be increased to 86% after exclusion of patients with all three risk factors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ureteric colic is one of the common emergencies with a lifetime prevalence of 10–15% and ureteric calculus constitutes 20% of all stone diseases in urology [1, 2]. Medical expulsive therapy (MET), shock wave lithotripsy and ureteroscopic lithotripsy are available modalities of treatment for ureteric calculi. If the pain is manageable and there is no infection or renal failure, expectant management with MET can be the first-line treatment within a reasonable time frame. However, the failure rate of expectant management is about 30–40% which can make a patient endure symptoms for a longer period of time with no benefit [3]. The superiority of alpha-blockers compared to other medications has been proved in reducing colic episodes and in successful stone expulsion [4]. Parameters which affect spontaneous expulsion have been studied extensively. Size and location of stone are the most accepted ones in clinical practice [4, 5]. There could be some other parameters which can play an important role in predetermination of success rate and these can guide urologists for appropriate selection of patients. These hidden factors can be related to the inflammatory reactions which are produced by the calculus. Various studies have been done on inflammatory markers level. However, their relation to spontaneous stone passage is not consistent and reproducible. C-reactive protein (CRP) is an acute phase protein which is synthesized in the liver. Its level rises in various conditions like renal tubular injury, pyelonephritis and vesicoureteral reflux. It can be useful in prediction of failure of expectant management and in the selection of an appropriate patient for the same. The aim of our study is to analyze the definitive relation of CRP and other factors with the spontaneous stone passage in patients with distal ureteric calculus of 5–10 mm and to calculate the risk of failure of expectant management in an index patient with pre-defined parameters.
Materials and methods
The present study is a prospective clinical study conducted in the Department of Urology, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER) from August 2016 to May 2018 with clinical trial registration number CTRI/2018/04/012974. The approval from the Institute Ethics Committee (Human Studies) was obtained for the study. The sample size is estimated both for estimating the simultaneous stone expulsion and also identifying the association of stone expulsion with CRP. The expected percentage of patients with non-expulsion was 25% and the sample size is estimated at 5% level of significance and 25% relative precision. Final estimated size was 185.
Patients of 18–50 years of age with acute colicky pain due to maximal 5–10 mm size lower ureteric calculi confirmed by non-contrast CT of kidney, ureter, and bladder (NCCT KUB) were included in the study. We excluded patients with pregnancy, solitary kidney, impaired renal function, who wished to remove the stone immediately. Patients who were suffering from any inflammatory disease (viral infection, arthritis, gastroenteritis, hepatitis, or respiratory infection), cardiovascular disease, obesity, diabetes, and lost to follow-up were also excluded from the study.
Patients with flank pain were initially screened with X-ray KUB and ultrasound (USG) KUB and subsequently underwent NCCT KUB to confirm the diagnosis. Blood sample for complete blood counts (CBC) and CRP was drawn at the time of presentation. We prescribed Tamsulosin 0.4 mg for 4 weeks and a nonsteroidal anti-inflammatory drug (NSAIDs) for 5 days as MET and for pain relief, respectively. CRP levels were estimated at initial presentation prior to starting NSAIDs (NSAIDs are known to reduce the CRP). It was measured by dilution method using a latex agglutination test, RHELAX CRP (TULIP Diagnostics Ltd., India). Normal CRP level in our laboratory is 0.6 mg/dl. A level above 0.6 mg/dl was considered as positive. Standardization of detection limit of RHELAX-CRP is traceable to the WHO, international reference standard (85/506) for human CRP. Assays were performed at JIPMER Hospital Laboratory.
We reassessed all patients at 2 weeks and at 4 weeks in terms of symptoms, X-ray, USG KUB and if needed by NCCT KUB. Persistent stone at 4 weeks is classified as a failure of conservative management and planned for definitive surgical treatment. The patients evaluated in the study were divided into two groups, namely, group A patients with spontaneous expulsion of stone and group B patients who failed to pass the stone and required surgical intervention. We compared age, gender, stone size in the axial and coronal section of NCCT, CRP, blood urea, creatinine, total leucocyte count (TLC), kidney size, HUN, and renal parenchymal thickness.
HUN was defined as AP renal pelvic diameter more than 6 mm in NCCT KUB.
To define risk in the index patient, we divided patients according to the number of significant factors and the estimated success rate in each group.
Statistical analysis
Continuous data were checked for normality by one-sample Kolmogorov–Smirnov test. The comparison of the age, stone size, kidney size, renal parenchymal thickness, CRP and other continuous variables mentioned above in relation to the categorical variables was carried out using independent Student’s t test/Mann–Whitney U test. The association of spontaneous stone expulsion with categorical variables like HUN, gender, and laterality had been carried out using the Chi-square test. The predictive power of the significant continuous variable for the stone expulsion was carried out using the receiver operating characteristic (ROC) curve. The independent factors associated with the simultaneous stone expulsion explored using logistic regression analysis. All statistical analyses were performed using SPSS version 19 at 5% level of significance and p value < 0.05 was considered as significant.
Results
Among 185 patients, the mean age was 34.36 years with a male to female ratio of 2.3:1.
Overall 122 (65.90%) patients successfully passed the stone and were included in group A. 63 (34.10%) patients who failed to pass the stone required further intervention and were included in group B. Out of 52 CRP-positive patients, 28 (53.84%) failed to pass the stone. Similarly, in 133 CRP-negative patients, 98 (73.60%) patients successfully passed the stone.
In group B, 47 patients underwent elective ureteroscopic stone removal after 4 weeks. Of the remaining, seven patients presented with fever and nine with refractory recurrent colic underwent DJ stenting in emergency and they finally underwent ureteroscopic lithotripsy electively.
Table 1 demonstrates the comparison of parameters between the groups. Hydroureteronephrosis, level of CRP, transverse and longitudinal diameter of stone, ureteral diameter proximal and distal to stone were significantly higher in group B.
In multivariate analysis, low CRP (p = 0.002), smaller longitudinal diameter of stone (p < 0.001) and the presence of hydroureteronephrosis (p = 0.005) were significantly associated with successful stone expulsion (Table 2).
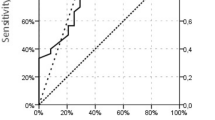
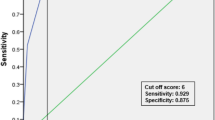
We used ROC curve to determine the cutoff value of CRP and longitudinal diameter of stone for prediction of failure (Figs. 1, 2). For CRP, we calculated cutoff of 0.41 mg/dl at 82% sensitivity and 78% specificity. Similarly for longitudinal diameter, the calculated cutoff was 6.7 mm at 90% sensitivity and 71% specificity.

ROC curve for C reactive protein (AUC = 0.820, p < 0.001) to determine the cut-off value for prediction for the failure of the spontaneous expulsion of stone

ROC curve for the longitudinal diameter of stone (AUC = 0.851, p < 0.001) to determine the cut-off value for prediction for the failure of the spontaneous expulsion of stone
On the basis of number of significant factors, we divided all patients into four groups and estimated success rate in each group (Table 3). In the group of patients with no risk factor, the success rate was 96.7%, similarly 96.3% in patients with a single risk factor, 62.3% in patients with two risk factors and 16.7% in patients with all three risk factors. The adjusted success rate after removal of patients with all three risk factors was 85.40%.
Discussion
In clinical practice, a noninvasive approach is preferred over invasive one. There is a dispute in decision making for the management of lower ureteric calculus, especially for patients with stone size less than 10 mm. The failure rate of MET may be a strong reason behind this. Assigning a patient to MET for ureteric calculi can sometimes make a patient endure symptoms with no benefits. These patients have to live with the obstructed urinary tract. This can lead to irreversible renal damage.
The success rate of MET in our study was 65.9%, which is comparable to other similar studies [6,7,8,9,10].
Ureteroscopic lithotripsy (URSL) is the most preferred invasive treatment with a success rate of up to 93% [11]. However, URSL has its own complications and is more expensive than expectant management. Hence, the challenge is to identify those patients who are at greatest risk of failure of MET so that they can undergo early intervention.
It is well known that the level of CRP increases with age; hence, we excluded patients older than 50 years [12]. However, we did not find any association of age with expulsion. Some studies have found that stone expulsion rate decreases with age and hypothesized that older age leading to a sedentary lifestyle can decrease ureteric peristalsis similar to esophageal peristalsis [13].
TLC is one of the markers of inflammation and showed significant association with CRP level. However, its association with expulsion was not found to be significant in the present study. Sfoungaristos et al. [14] found leukocytosis in patients with spontaneous expulsion. On the contrary, Park et al. [15] and Lee et al. [16] found that a higher percentage of neutrophils and higher neutrophil to lymphocyte ratio were associated with failure of expulsion. For better interpretation, it is imperative to consider TLC along with other clinical features.
Miller et al. [17] reported a higher expulsion rate in right-sided stone owing to the caudal location of the right kidney. On the other hand, Sfoungaristos et al. [5] demonstrated that left-sided stones are more prone to pass spontaneously owing to fewer attachments of the left ureter with peritoneum when compared to its right counterpart resulting in greater mobility. All these contradictory findings may suggest dependency on anatomical variations rather than laterality.
CRP is a nonspecific marker of inflammation synthesized in the liver. It rises in inflammatory conditions like appendicitis, cystitis and UTI [18,19,20]. Ureteric calculus produces inflammatory changes in the ureter leading to a rise in its serum level. This is well correlated with the intensity of inflammation which is determined by the degree of obstruction. In severe inflammatory conditions like pyelonephritis, CRP is seen to rise by 20 times the normal value and such patients need an early intervention [21].
In our study, we used CRP as a novel parameter for decision making whenever there is an ambiguity viz. expectant management or early intervention.
Özcan et al. [13] concluded that the patients of lower ureteric calculi of size 4–10 mm with high CRP level were significantly associated with failure of expulsion with a cut off value of 0.506 mg/dl. Aldaqadossi [22] calculated the cutoff at 2.19 mg/dl.
Hada et al. [23] analyzed the association of CRP with stone expulsion and demonstrated that only CRP was significantly associated with stone expulsion with the cutoff at 2.45 mg/dl. In our study, cutoff was 0.41 mg/dl. Their high cutoff of CRP may be due to the non-exclusion of patients with confounding factors. They have also not estimated success rate of MET in the individual patient based on significant factors.
In our study, 26% of patients even with negative CRP were not able to pass the stone. All these patients had other two significant associated parameters. It suggests that the outcome cannot be determined by a single parameter alone.
It needs to be stressed that patients with renal colic due to upper tract calculi, who are older than 75 years with leukocytosis and high CRP (≥ 2.8 mg/dl), are more prone to sepsis and require emergency urinary diversion [24, 25].
Traditionally, for all practical purposes, transverse diameter of stone measured on axial sections is used for decision making and it is well known that axial images underestimate the size compared to coronal section [26]. In our study, we measured longitudinal as well as the transverse diameter of stone in coronal and axial sections, respectively. We found that transverse diameter which is expected to be a parameter associated with failure was not found to be statistically significant in multivariate analysis. However, the longitudinal diameter of stone was significantly (p = 0.001) associated with failure with an odds ratio of 2.34. We calculated the cutoff of 6.7 mm at sensitivity and specificity of 90% and 71%, respectively, using the ROC curve.
Lee et al. [26], in their retrospective study, demonstrated a mean stone diameter of 6.79 mm in failure group and 5.1 mm in the success group based on longitudinal diameter which is similar to our prospective study.
It is hypothesized that ureteral stones are cylindrical in shape and elicit more inflammation longitudinally rather than transversely owing to larger contact surface area with the ureteric wall.
It is well known that severe HUN associated with long-term obstruction secondary to large ureteric stone affects overall renal parenchymal function and in this subset of patients, secondary ureteral pathologies like mucosal edema and stricture make conservative management a poor option [27, 28].
Factors like ureteral diameter proximal and distal to stone and transverse diameter of stone which are significantly associated with expulsion in univariate analysis are not found to be significant in multivariate analysis.
Till date, no study has calculated precise risk in index patient on the basis of the aforementioned parameters which we have considered to define the risk of failure. In our study, after excluding patients with all three risk factors, the adjusted success rate of MET was 85.4%. In a group of patients with no risk factors or with single risk factor, the success rate was more than 95%.
Limitation of our study is that the results cannot be generalized to higher age group patients and patients with severe comorbidities as CRP value has an association with other parameters also. However, we have taken the population in which ureteric colic is more common. To overcome this limitation, further studies are needed in various age groups of patients.
Conclusion
To select an appropriate management strategy, it is crucial to predetermine the probability of spontaneous stone passage. Longitudinal diameter of stone, the presence of HUN and higher CRP are the significant risk factors for failure of spontaneous passage. The success rate of MET is 66% which can be increased to 85–90% by appropriate patient selection based on high-risk parameters. To reduce the failure rate of MET, patients with all three risk factors should be considered for early surgical intervention.
References
Rukin N, Siddiqui Z, Chedgy E, Somani B (2016) Trends in upper tract stone disease in England: evidence from the hospital episodes statistics database. Urologia Internationalis 98(4):391–396
Elton T, Roth C, Berquist T, Silverstein D (1993) A clinical prediction rule for the diagnosis of ureteral calculi in emergency departments. J Gen Intern Med 8(2):57–62
Dellabella M, Milanese G, Muzzonigro G (2003) Efficacy of tamsulosin in the medical management of juxtavesical ureteral stones. J Urol 170(6):2202–2205
Wang H, Man L, Huang G, Li G, Wang J (2016) Comparative efficacy of tamsulosin versus nifedipine for distal ureteral calculi: a meta-analysis. Drug Des Dev Ther 10:1257–1265
Sfoungaristos S, Kavouras A, Perimenis P (2011) Predictors for spontaneous stone passage in patients with renal colic secondary to ureteral calculi. Int Urol Nephrol 44(1):71–79
Celik S, Akdeniz F, Yildirim M, Bozkurt O, Bulut M, Hacihasanoglu M et al (2017) Computed tomography findings predicting the success of silodosin for medical expulsive therapy of ureteral stones. Kaohsiung J Med Sci 33(6):290–294
Ahmed A, Al-Sayed A (2010) Tamsulosin versus alfuzosin in the treatment of patients with distal ureteral stones: prospective, randomized, comparative study. Korean J Urol 51(3):193
Furyk J, Chu K, Banks C, Greenslade J, Keijzers G, Thom O et al (2016) Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized multicenter trial. Ann Emerg Med 67(1):86–95.e2
Hollingsworth J, Canales B, Rogers M, Sukumar S, Yan P, Kuntz G et al (2016) Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ 355:i6112
Wang C, Huang S, Chang C (2008) Efficacy of an α1 blocker in expulsive therapy of lower ureteral stones. J Endourol 22(1):41–46
Savić S, Vukotić V, Lazić M, Savić N (2014) Management of calculus anuria using ureteroscopic lithotripsy as a first line treatment: its efficacy and safety. Urol J 11(2):1392–1399
Pepys M, Hirschfield G (2003) C-reactive protein: a critical update. J Clin Investig 111(12):1805–1812
Özcan C, Aydoğdu O, Senocak C, Damar E, Eraslan A, Oztuna D et al (2015) Predictive factors for spontaneous stone passage and the potential role of serum C-reactive protein in patients with 4 to 10 mm distal ureteral stones: a prospective clinical study. J Urol 194(4):1009–1013
Sfoungaristos S, Kavouras A, Katafigiotis I, Perimenis P (2012) Role of white blood cell and neutrophil counts in predicting spontaneous stone passage in patients with renal colic. BJU Int 110(8b):E339–E345
Park C, Ha J, Park C, Kim C, Kim K, Kim B (2013) Relationship between spontaneous passage rates of ureteral stones less than 8 mm and serum C-reactive protein levels and neutrophil percentages. Korean J Urol 54(9):615
Lee K, Ha J, Koo K (2017) Significance of neutrophil-to-lymphocyte ratio as a novel indicator of spontaneous ureter stone passage. Yonsei Med J 58(5):988
Miller O, Kane C (1999) time to stone passage for observed ureteral calculi: a guide for patient education. J Urol 162(3):688–691
Paajanen H, Tainio H, Laato M (1996) A chance of misdiagnosis between acute appendicitis and renal colic. Scand J Urol Nephrol 30(5):363–366
Sandberg T, Lidin-Janson G, Edén C (1989) Host response in women with symptomatic urinary tract infection. Scand J Infect Dis 21(1):67–73
Shaoul R, Lahad A, Tamir A et al (2008) C-reactive protein (CRP) as a predictor for true bacteremia in children. Med Sci Monit 14:CR255–CR261
Horcajada J, Velasco M, Filella X, Alvarez L, De Lazzari E, Marin J et al (2004) Evaluation of inflammatory and renal-injury markers in women treated with antibiotics for acute pyelonephritis caused by Escherichia coli. Clin Vaccine Immunol 11(1):142–146
Aldaqadossi H (2013) Stone expulsion rate of small distal ureteric calculi could be predicted with plasma C-reactive protein. Urolithiasis 41(3):235–239
Hada A, Yadav SS, Tomar V, Priyadarshi S, Agarwal N, Gulani A (2018) Assessment of factors affecting the spontaneous passage of lower ureteric calculus on the basis of lower ureteric calculus diameter, density, and plasma C-reactive protein level. Urol Ann 10:302–307
Angulo J, Gaspar M, Rodríguez N, García-Tello A, Torres G, Núñez C (2010) The value of C-reactive protein determination in patients with renal colic to decide urgent urinary diversion. Urology 76(2):301–306
McSorley S, Drury M, Majumdar P, Halsall A, Nalagatla S (2013) C-reactive protein to predict the need for surgical intervention in acute renal colic. J Clin Urol 7(6):380–383
Lee S, Jeon H, Park D, Choi Y (2012) Longitudinal stone diameter on coronal reconstruction of computed tomography as a predictor of ureteral stone expulsion in medical expulsive therapy. Urology 80(4):784–789
Hwang E, Kim Y, Yuk S, Sul C, Lim J (2010) Factors that predict spontaneous passage of a small distal ureteral stone %3c 5 mm. J Endourol 24(10):1681–1685
Hiller N, Berkovitz N, Lubashevsky N, Salaima S, Simanovsky N (2012) The relationship between ureteral stone characteristics and secondary signs in renal colic. Clin Imaging 36(6):768–772
Funding
This study was not funded by any agency.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study is highly compliant without variation from Ethical Standard. Annual progression reports are submitted to the institutional ethical committee.
Conflict of interest
None of the authors have any conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and also the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval was obtained for the study on 05/07/2016 (JIP/IEC/2016/27/884).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jain, A., Sreenivasan, S.K., Manikandan, R. et al. Association of spontaneous expulsion with C-reactive protein and other clinico-demographic factors in patients with lower ureteric stone. Urolithiasis 48, 117–122 (2020). https://doi.org/10.1007/s00240-019-01137-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-019-01137-x