
Abstract
This meta-analysis aims to compare the safety and efficacy of fluoroscopy versus ultrasound guidance during the access to the renal collecting system. A systematic literature review was performed in September 2016. Outcomes were explored using review manager v5.0. 18 studies with 2919 patients were included in the final analysis. There was no significant difference in stone-free rate (RR: 1.0; 95% CI, 0.98 to 1.05; p = 0.41), operation time (MD: 1.75; 95% CI, −9.15 to 12.65; p = 0.75), hospital stay (MD: −1.02; 95% CI, −3.08 to 1.05; p = 0.34), and success rate of tract creation (RR: 1.00; 95% CI, 0.98–1.02; p = 0.88) between ultrasonography and fluoroscopy. Compared to fluoroscopy, ultrasonography had shorter puncture time (MD: −4.71; 95% CI, −6.43 to −3.0; p < 0.0001), higher success rate of fist puncture (RR: 1.16; 95% CI, 1.04 to 1.3; p = 0.01), less blood loss (MD: −0.42, 95% CI −0.81 to −0.02; p = 0.04), and less transfusion requirement (RR: 0.73; 95% CI, 0.33–1.6; p = 0.44). Two patients in each group experienced perforation of the renal pelvis. Five patients in fluoroscopy and two in ultrasonography group had pneumothorax. One patient in fluoroscopy group had intestinal injury. Both fluoroscopy and ultrasound guidance can aid to obtain successful percutaneous renal access. The advantages of ultrasonography over fluoroscopy include shorter puncture time, higher success rate of fist puncture, less blood loss, and less complications.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Renal access is a major step for percutaneous nephrolithotomy (PCNL). It can be obtained either with fluoroscopy or ultrasound guidance. Fluoroscopy was the most commonly used image modality. However, fluoroscopic use can result in radiation exposure to the patient and the staff in the operating theatre. Ultrasound is another useful interventional tool which has the advantages of reduced radiation exposure, lower cost, and portability [1, 2]. And it is the choice for pregnant or transplanted patients [3–5].
To date, the choice of the imaging modality is mainly based on the preference of the surgeon. The ideal modality of image guidance for PCNL has not reached a consensus. Therefore, we perform the meta-analysis of available studies comparing the safety and efficacy between ultrasonography and fluoroscopy during PCNL.
Literature search and article selection
We carried out an electronic search of PubMed, Embase, Cochrane Library, Chinese Biomedical Literature databases, and Chinese National Knowledge Infrastructure to find relevant studies in September 2016. The search terms included: “Percutaneous Nephrostomy”, “Percutaneous nephrolithotomy”, “PCNL”, “minimally invasive percutaneous nephrolithotomy”, “MPCNL”, “fluoroscopy”, “X-ray”, “ultrasound”, “ultrasonography”, “US”, and their synonyms. References of searched papers were also checked manually to identify relevant articles.
Two reviewers independently selected studies for inclusion. Studies were included if they met the following criteria: (1) patients who received percutaneous PCNL, (2) adult patients, (3) patients received either ultrasound or fluoroscopy guidance.
Data extraction and quality assessment
The data were independently extracted using a pre-defined data extraction form, which included study characteristics, patient characteristics, and methodological quality. The measured outcomes were stone-free rate, operation time, hospital stay, time to puncture, success rate of access creation and first puncture, hemoglobin decrease and transfusion requirement.
The methodological quality of the studies was assessed using the Newcastle-Ottawa Scale (NOS) for nonrandomized controlled trials [6] and the Jadad scale for RCTs [7].
Statistical analysis
Meta-analysis was performed by Review Manager 5.3. For dichotomous variables, results were expressed as risk ratios (RR) with 95% confidence intervals (CI). For continuous outcomes, the mean difference (MD) was used with 95% CI. Heterogeneity between the included studies was analyzed using a Chi2 test and the I2 test, with p value of 0.05 used for statistical significance. The data were analyzed using the random-effects model when I-square >25%. Forest plots were used for graphical displays of results from the meta-analysis.
Results
Study characteristics
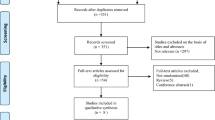
The search strategy identified 352 studies (Fig. 1). 18 studies [8–25] with 2919 patients were included in the final analysis. The literature screening process is shown in Fig. 1. Six studies were RCTs and twelve were case–control studies. Table 1 presents the study characteristics and quality assessment of the included studies.

Study flow chart outlining the systematic search strategy and study selection process
Stone-free rate
Thirteen studies reported the stone-free rate. No statistical significant difference was found when ultrasonography was compared with fluoroscopy for stone-free rate (RR: 1.0; 95% CI, 0.98–1.05; p = 0.41, Fig. 2a).

Forest plot comparing stone-free rate (a), operation time (b), and hospital stay (c)
Operation time
The data of operation time was available in 4 studies. The pooled data showed no significant difference between ultrasonography and fluoroscopy (MD: 1.75; 95% CI, −9.15 to 12.65; p = 0.75, Fig. 2b).
Hospital stay
A forest plot for the difference in hospital stay of the two methods is presented in Fig. 2c. There was no significant difference in hospital stay group between the two groups (MD: −1.02; 95% CI, −3.08 to 1.05; p = 0.34).
Success rate of access creation and first puncture
Meta-analysis of eleven studies showed no significant difference in success rate of access creation between ultrasonography and fluoroscopy (RR: 1.00; 95% CI, 0.98–1.02; p = 0.88, Fig. 3a). Five studies reported the success rate of first puncture. Meta-analysis of these studies indicated that the ultrasonography had a higher success rate than fluoroscopy (RR: 1.16; 95% CI, 1.04–1.3; p = 0.01, Fig. 3b).

Forest plot comparing success rate of access creation (a), success rate of first puncture (b), and time to puncture (c)
Time to puncture
Twelve studies reported the time to puncture. The data were heterogeneous (I 2 = 99%), and the random-effect model showed less time in ultrasonography group as compared with fluoroscopy group (MD: −4.71; 95% CI, −6.43 to 3.0; p < 0.0001, Fig. 3c).
Hemoglobin decrease and transfusion requirement
Five studies reported hemoglobin decrease. The data were heterogeneous (I 2 = 91%), and the random-effect model showed that the hemoglobin decrease was less in the ultrasonography group (MD: −0.42, 95% CI −0.81 to −0.02; p = 0.04, Fig. 4a). Meta-analysis of four studies by the fixed-effects model (I 2 = 0%) demonstrated less blood transfusion in the ultrasonography group. There was no significant difference between the two groups (RR: 0.73; 95% CI, 0.33–1.6; p = 0.44, Fig. 4b).

Forest plot comparing hemoglobin decrease (a), hemoglobin decrease (b), and fever (c)
Complications
Meta-analysis of three studies showed no significant difference in fever (RR: 0.37; 95% CI, 0.08–1.76; p = 0.21, Fig. 4c).Two patients in each group experienced perforation of the renal pelvis during the attempt to gain access [8, 13]. Five patients in fluoroscopy and two in ultrasonography group had pneumothorax [16, 20, 22]. One patient in fluoroscopy group had intestinal injury [20].
Discussion
The access to the renal collecting system is the first process in PCNL, and this procedure is usually performed under fluoroscopy. Ultrasound is another image modality for obtaining access and the number of studies demonstrating the success of ultrasound-guided PCNL is increasing. Our meta-analysis compared the safety and efficacy of the two imaging methods and demonstrated that there was no significant difference in stone-free rate, operation time, hospital stay and success rate of tract creation. Compared to fluoroscopy, ultrasonography had shorter puncture time, higher success rate of fist puncture, less blood loss and less postoperative complication.
Fluoroscopy is an important tool for the performance of PCNL. It is useful during puncture on the kidney, insertion of guidewires, tract dilatation and removal of stones [26]. However, fluoroscopy-guided PCNL exposes both patients and operators to a significant amount of ionizing radiation which may cause genetic mutation and cancer, and the severity of the effect increases with dose [27, 28]. As the number of PCNL procedures performed is increasing, the cumulative dose of radiation may be substantial especially in high-volume centers. It is important to follow the principles of As Low As Reasonably Achievable (ALARA) in PCNL [27]. The International Commission on Radiation Protection (ICRP) recommends the annual limit for equivalent dose in the lens of the eye at 150 mSv, in the skin at 500 mSv, and in the extremities at 500 mSv [29]. For this reason, using ultrasound instead of fluoroscopy during PCNL should be popularized to reduce radiation exposure.
Our analyses indicated that there is no difference in the stone-free rate and hospital stay. Meanwhile, our study showed some advantages of ultrasonography guidance. First, in ultrasonography guided PCNL, the time taken to puncture was shorter and the success rate of first puncture was higher. During the access to the calyx with ultrasonography, you do not need to rotate the x-ray machine and wear a lead apron and thyroid collar to protect you from radiation. It is quick to obtain the access to the targeted calyx especially for experienced operators.
Another advantage of ultrasonography guidance was lower risk of complications. The analysis indicated that the hemoglobin decrease was significantly less in the ultrasonography group. And transfusion requirement reduced in the ultrasonography group. The reason for this difference may be related to the shorter access time. As Akman showed that the blood loss during PCNL was related to prolonged access time [30]. In addition, we think the high success rate of first puncture also contributed to the less blood loss. Additionally, US can help to evaluate the depth of the access needle and allow identification of the surrounding structure, thus avoiding injuries to nearby organs. The present study also showed less pneumothorax and intestinal injury in the ultrasonography guided PCNL.
However, US guided PCNL is experience dependent and requires a certain amount of training. Yan Song indicated that the ultrasound screening time and operation time both dropped as the experience gradually increased, he concluded that the number for the competence with high stone-free rate and without major complication is 60 [31]. At present, not all the operators can perform this technique independently. In china, ultrasonography is a commonly used modality in many centers, and is familiar to most urologists. Many of them use ultrasonography guidance for all stages of PCNL without fluoroscopy, and operation time is usually shorter under ultrasonography guidance.
The choice for image guidance is mainly based on personal preference and experience. The fluoroscopy is familiar to most urologists and it is the most commonly used technique in many centers. The CROES PCNL data revealed that 86.3% of patients had fluoroscopic-guided access vs 13.7% with ultrasonography guidance [32]. One factor that limits the wide use of ultrasonography is the early learning curve. It is hard for the beginners. For example, they may misjudge the actual position of the needle tip with ultrasonography guidance, easily causing a deeper puncture than expected. Another problem of the ultrasonography is poor imaging of the renal anatomy in obese patients and in patients with nondilated collecting systems [33]. In this condition, a combined approach using ultrasound and fluoroscopy may be a good choice.
There are several limitations to our present study. First of all, most of the studies were nonrandomized comparisons. There were only six RCTs available for inclusion. In addition, heterogeneity among studies was high for several parameters. This heterogeneity could be due to difference in study design, medical settings and surgeon’s experience.
Conclusion
In conclusion, current evidence from this meta-analysis indicated that both fluoroscopy and ultrasonography guidance can aid to obtain successful percutaneous renal access. In addition to radiation free, the advantages of ultrasonography over fluoroscopy include shorter puncture time, higher success rate of first puncture, less blood loss, and less complications.
References
Zegel HG, Pollack HM, Banner MC et al (1981) Percutaneous nephrostomy: comparison of sonographic and fluoroscopic guidance. AJR Am J Roentgenol 137(5):925–927
Basiri A, Ziaee SA, Nasseh H et al (2008) Totally ultrasonography-guided percutaneous nephrolithotomy in the flank position. J Endourol Endourol Soc 22(7):1453–1457
Evans HJ, Wollin TA (2001) The management of urinary calculi in pregnancy. Curr Opin Urol 11(4):379–384
McAleer SJ, Loughlin KR (2004) Nephrolithiasis and pregnancy. Curr Opin Urol 14(2):123–127
Francesca F, Felipetto R, Mosca F, Boggi U, Rizzo G, Puccini R (2002) Percutaneous nephrolithotomy of transplanted kidney. J Endourol Endourol Soc 16(4):225–227
Cook DA, Reed DA (2015) Appraising the quality of medical education research methods: the Medical Education Research Study Quality Instrument and the Newcastle-Ottawa Scale-Education. Acad Med J Assoc Am Med Coll 90(8):1067–1076
Clark HD, Wells GA, Huet C et al (1999) Assessing the quality of randomized trials: reliability of the Jadad scale. Control Clin Trials 20(5):448–452
Jagtap J, Mishra S, Bhattu A, Ganpule A, Sabnis R, Desai MR (2014) Which is the preferred modality of renal access for a trainee urologist: ultrasonography or fluoroscopy? Results of a prospective randomized trial. J Endourol Endourol Soc 28(12):1464–1469
Basiri A, Mirjalili MA, Kardoust Parizi M, Moosa Nejad NA (2013) Supplementary X-ray for ultrasound-guided percutaneous nephrolithotomy in supine position versus standard technique: a randomized controlled trial. Urol Int 90(4):399–404
Agarwal M, Agrawal MS, Jaiswal A, Kumar D, Yadav H, Lavania P (2011) Safety and efficacy of ultrasonography as an adjunct to fluoroscopy for renal access in percutaneous nephrolithotomy (PCNL). BJU Int 108(8):1346–1349
Karami H, Rezaei A, Mohammadhosseini M, Javanmard B, Mazloomfard M, Lotfi B (2010) Ultrasonography-guided percutaneous nephrolithotomy in the flank position versus fluoroscopy-guided percutaneous nephrolithotomy in the prone position: a comparative study. J Endourol Endourol Soc 24(8):1357–1361
Falahatkar S, Neiroomand H, Enshaei A, Kazemzadeh M, Allahkhah A, Jalili MF (2010) Totally ultrasound versus fluoroscopically guided complete supine percutaneous nephrolithotripsy: a first report. J Endourol Endourol Soc 24(9):1421–1426
Basiri A, Ziaee AM, Kianian HR, Mehrabi S, Karami H, Moghaddam SM (2008) Ultrasonographic versus fluoroscopic access for percutaneous nephrolithotomy: a randomized clinical trial. J Endourol Endourol Soc 22(2):281–284
Liu L, Liu SH, Zhang JX, Fu X, Suai Q (2013) Comparison of clinical application in percutaneous nephrolithotomy between B ultrasound and arm X light positioning. China Med Pharm 3(12):115–121
Chen MX, Wang HS, Liao XP (2012) Experience of minimally invasive percutaneous nephrolithotomy under B ultrasound combined with X-ray. Zhong guo she qu yi shi 14(24):161–163
Liang XD, Liu XL, Zhang QL (2012) B ultrasound versus fluoroscopy in percutaneous nephrolithotomy. Xinjiang Med J 42(6):55–57
Liu YL, Hu JQ, Ou ZQ, Li T (2014) B ultrasound versus fluoroscopy in percutaneous nephrolithotomy. Mod Diagn Treat 25(12):2746–2747
Xin R, Zhang GM, Xing Q (2010) Comparison of the efficacy of established access under the guidance of B-ultrasound and radiography in percutaneous nephrolithotomy. Chin J Clin Healthcare 12(1):54–56
Wu XH, Jiang XZ, Zhong KB, Dai YB (2007) Comparison of the efficacy of established percutaneous access under the guidance of B-ultrasound and radiography. J Modern Med Health 24(5):649–651
Sun XH, Lin WT, Wu WZ, Tan JM (2007) Comparison of the efficacy of B-ultrasound versus radiography in percutaneous nephrolithotomy. Chin J Misdiag 7(28):6755–6756
Dong GQ (2014) Comparison of ultrasonography versus fluoroscopy for renal access in minimally invasive percutaneous nephrolithotomy. China Foreign Med Treat 5(14):164–165
Wu JP, Liu J, Jia RP, Shu JH, Shen MS, Sun HB, Cao ZG (2013) Comparison of ultrasound and X-ray in establishing percutaneous access for minimally invasive percutaneous nephrolithotomy. J Modern Urol 18(1):46–47
Zhu ZP, Di JM (2013) Comparative analysis of percutaneous nephrolithotomy with B ultrasound and X-ray guided puncture in treatment of kidney calculi. Chin J Endourol 7(3):213–215
Yang XM, Liu G, Liu J, Chang LS, Yang YF, Song DK (2007) Comparison of ultrasound and X-ray in establishing percutaneous nephrolithotomy aisies. Chin J Pract Med 36(14):39–41
Chen HM, Li YS, Xu YG (2013) The comparative analysis of ultrasound and X-ray guided percutaneous nephrolithotomy in the treatment of renal calculus. J Laparosc Surg 18(7):497–499
de la Rosette J, Assimos D, Desai M, Gutierrez J, Lingeman J, Scarpa R et al (2011) The Clinical Research Office of the endourological society percutaneous nephrolithotomy global study: indications, complications, and outcomes in 5803 patients. J Endourol 25:11–17
Lipkin ME, Preminger GM (2012) Risk reduction strategy for radiation exposure during percutaneous nephrolithotomy. Curr Opin Urol 22(2):139–143
Kumar P (2008) Radiation safety issues in fluoroscopy during percutaneous nephrolithotomy. Urol J Winter 5(1):15–23
The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Annals of the ICRP. 2007;37(2–4):1–332
Akman T, Binbay M, Sari E et al (2011) Factors affecting bleeding during percutaneous nephrolithotomy: single surgeon experience. J Endourol Endourol Soc 25(2):327–333
Song Y, Ma Y, Song Y, Fei X (2015) Evaluating the Learning Curve for Percutaneous Nephrolithotomy under Total Ultrasound Guidance. PLoS One 10(8):e0132986
Andonian S, Scoffone CM, Louie MK et al (2013) Does imaging modality used for percutaneous renal access make a difference? A matched case analysis. J Endourol Endourol Soc 27(1):24–28
Park S, Pearle MS (2006) Imaging for percutaneous renal access and management of renal calculi. Urol Clin N Am 33(3):353–364
Acknowledgements
Supported by Grant 31170907, Grant 31370951, Grant 81470927, Grant 81300579 from the National Natural Science Foundation of China, Grant 2014SZ0028 from the Technology Support Program of Science and Technology Department of Sichuan Province, and Grant 2014SCU04B21 the scientific research foundation of Sichuan University for talented young scholars.
Conflict of interest
The authors have declared that no conflict of interest exists.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Liu, Q., Zhou, L., Cai, X. et al. Fluoroscopy versus ultrasound for image guidance during percutaneous nephrolithotomy: a systematic review and meta-analysis. Urolithiasis 45, 481–487 (2017). https://doi.org/10.1007/s00240-016-0934-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-016-0934-1