
Abstract
There are an increasing number of healthcare smartphone applications (‘apps’) available. Urolithiasis presents a major healthcare burden. Patients are increasingly keen to educate themselves regarding the diagnosis and management of their condition. There is no formal regulation of healthcare apps, including a large number of apps relating to urolithiasis. This review aims to examine the range of apps available, and the prevalence of healthcare professional input. Four international smartphone app stores were searched: Apple’s App Store, Google Play (Android), BlackBerry App World and the Windows Phone App store. A total of 42 unique apps were downloaded and analysed. Recorded data included the cost (£/$), publisher information, number of ratings, average rating and any documentation of medical professional involvement. Twenty-one (50 %) apps required payment for download. The mean cost was £3.58 ($6.04) with range £0.61–£34.90 ($1.03–$58.87). Thirty-three (79 %) of the 42 apps were designed to be used by patients. Fifteen (36 %) of the 42 apps had clear input from health professionals. Twenty-two apps offered patient information, including dietary advice on lowering calcium intake, which is contrary to current evidence-based practice. We conclude that urolithiasis apps have future potential to inform both patients and healthcare professionals on stone management. However, inaccuracies in the recommendations made by some apps can be misleading or even harmful due to a lack of specialist involvement. We recommend improving the usefulness of these apps by seeking a ‘quality stamp’ from recognised urological organisations and greater clinician involvement in future app development.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A smartphone can be defined as a computer system within a phone that is able to perform a diverse range of tasks [1]. Smartphone ownership continues to grow with 56 % of American adults now owning a smartphone [2] and the resulting market for applications (apps) expanding alongside increasing smartphone usage. There have been an estimated 1 billion app releases so far and app revenues from the first half of 2010 alone were estimated as $2.2 billion [3]. Downloadable apps can be free or available to buy, and the only limit on their design is the requirement to run quickly and easily using the available smartphone hardware.
‘Health apps’ are used in a number of ways including as reference tools for both patients and health professionals [1, 4, 5]. There are estimated to be over 7,000 smartphone health apps [6]. Their use includes providing medical advice, appointment prompts, treatment compliance monitors, health questionnaires, and access to information at point of care (decisions supports and health records) [7]. One recent study has suggested a doubling in the ‘health-related’ use of mobile phones by the US population between 2010 and 2012 [8] and it is estimated that by 2015 five hundred million smartphone users will be using a healthcare application worldwide [9]. Despite the wide range of health apps available to clinicians and their patients, very few have undergone formal regulatory approval [10]. To date, the use of smartphone health apps has been documented in a range of specialties including orthopaedic surgery, neurosurgery, plastic surgery, urology, infectious diseases and obesity surgery [1, 3, 5, 11–13].
Urolithiasis is a major clinical and economic burden for healthcare systems and the prevalence of urological stone disease is rising across the world [14–16]. With increasing numbers of patients being diagnosed with this condition, there is a need for the provision of reliable health information on a variety of related topics including prevention, diagnosis, treatment and long-term sequelae. Inevitably, patients and the public are using smartphone apps and the internet, as a source of information presenting a range of potential benefits to the end user including: supplementing information received from a healthcare professional, anonymity in health information seeking and increases in understanding of medical conditions [17]. However, there are concerns regarding the utilisation of apps by both patients and clinicians without regulation or peer review [7]. In September 2013, the FDA issued “Mobile Medical Applications Guidance for Industry and Food and Drug Administration Staff” which explains the agency’s oversight of only those mobile medical apps that can be classified as medical devices and its intention to focus on those that present a greater risk to patients [18].
In light of the increasing prevalence of health-related smartphone apps, and the lack of formal regulation, the aim of this study is to review available ‘apps’ for urolithiasis and to assess the level of medical professional involvement in their design.
Methods
Smartphone apps relating to urolithiasis were identified in September 2013. Four UK app stores were searched: Apple’s App Store, Google Play (Android), BlackBerry App World and the Windows Phone App store. Two authors undertook the search independently using simple keywords and phrases relating to urolithiasis in the way a member of the public would search in the app store interface (Table 1). Apps designed for patients and/or health professionals and citing urolithiasis in their title and/or content were included. Data were collected from the app overview provided by the developer and free and paid apps were downloaded for analysis. Recorded data included the cost ($ = US dollars), publisher information, number of ratings, average rating and any documentation of medical professional involvement. Apps were then subcategorised based on their primary content topic and target audience (Table 2). Each app was reviewed independently by the authors (DJS and KM) for medical accuracy of content. Content was rated on a 4-point Likert scale with: 1 = mostly inaccurate information with little scientific basis for advice, 2 = some scientific basis for information given but significant inaccuracies, 3 = mostly accurate and broadly follows recognised medical advice and 4 = medically sound advice (Table 3). If the accuracy rating between the two authors differed, a consensus was reached with discussion as to the most representative rating.
Results
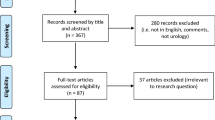
A total of 44 apps relating to urolithiasis were identified (Apple App Store = 14, Windows Phone App Store = 1, BlackBerry App World = 1, Google Play = 28).
2 of 44 apps were duplicated, 1 in Apple’s App store and Google Play, 1 in BlackBerry World and Google Play. When duplicated in two stores, the Google Play apps were excluded once they had been checked in both platforms to check format and content was consistent. Therefore, 42 apps were categorised.
Thirty-three (79 %) of the 42 apps were designed to be used by patients. Apps were categorised as follows: patient information (n = 22, 52 %), health professional resources (n = 9, 21 %), patient dietary recording tools (n = 4, 10 %), patient advice on herbal remedies (n = 4, 10 %), patient advice on uric acid/gout (n = 2, 5 %) and one app advertising medical professionals/latest evidence (n = 1, 2 %). Fifteen (36 %) of the 42 apps had clear input from health professionals (Table 2).
Twenty-one of the 42 apps (50 %) required payment for download. The mean cost was $6.04 (£3.58) with range $1.03–$58.87 (£0.61–£34.90). Nineteen (45 %) apps had a customer satisfaction score based on ratings. The mean number of customer ratings per app was 8.5 (range 1–52) and the mean app rating score was 3.6 out of 5 (range 1–5). Six of the 42 apps (14 %) had the lowest accuracy rating of 1, 20 (48 %) apps had a rating of 2, 10 (24 %) apps had a rating of 3 and 6 (14 %) apps had the highest accuracy rating of 4.
Patient information
22 (52 %) apps were identified offering patient information relating directly to the aetiology and management of urolithiasis or recommending dietary changes. 16 of these 22 apps provided predominantly information regarding the aetiology and management of kidney stones in terms of descriptions and diagrams to explain specific medical terminology. Health professional input was apparent in 3 out of the 22 apps (14 %). The remaining 6 apps in this category provided dietary advice including how to lower the amount of calcium in the diet, the role of honey in preventing kidney stones and advice on dietary intake of parsley. There was no evident health professional involvement in these 6 apps, accounting for 28 % of the 22 apps in this category.
Health professional resources
Nine out of the total of 42 apps (21 %) were identified that aimed to provide information for health professionals. Health professional involvement was evident in all apps. The information covered all aspects of aetiology and management of urolithiasis. Six of the nine apps (67 %) provided information on the whole field of urology. One of these apps, a ‘Handbook of Urology’ was produced by a recognised publisher and is fully referenced. The handbook app was significantly more expensive than the remaining apps, with the price matching the paper copy. Four of these nine apps (44 %) apps had customer ratings, with an average score of 3.6 (score 2.1–4.2).
Patient dietary recording tools
Four out of the total of 42 apps (10 %) were identified that provide interactive methods of recording dietary intake. All apps had customer ratings, with an average score of 3.8 (2–5). Two of the apps provided methods to record the patients’ daily intake of fluid and suggested strategies to increase how much they drink. One of these apps had health professional involvement. The two remaining apps provided a way of calculating daily calcium intake and offered information on foods which are high in calcium. There was no evidence of health professional involvement provided. All apps had customer ratings, with an average score of 3.8 (2–5).
Herbal remedies
Four out of the total of 42 apps (10 %) provided information on herbal remedies which they suggest can be used for the prevention/treatment of urolithiasis. There was no evidence of health professional involvement for any of these apps. One app had a customer rating, with an average rating of 4.7.
Uric acid/gout advice
Two apps provided information on the management of uric acid levels. Neither apps had a customer rating or evidence of health professional involvement. Information was provided that explained the formation and treatment of uric acid kidney stones, although the main aim of the app was to provide advice on the management and prevention of gout.
Advertisement of urologists/latest evidence
One app provided information on some of the latest urology research and press releases. However, the app also provided a list and contact details for local urologists and renal physicians. Health professional input was evident.
Discussion
As smartphones assume an increasingly important role in modern society, patients and physicians are accessing information in different ways. The ‘app’ now offers a portable and convenient way to provide content or fulfil a specific desired function. This study has summarised the availability of apps pertaining to urolithiasis and assessed the involvement of healthcare professionals in their design.
This review identified 42 apps of which 33 are aimed at patients. Fifteen of the 42 had input from healthcare professionals. All 6 apps which the author’s deemed to have medically sound advice, had evidence of input from healthcare professionals. Of the 36 apps which scored less than 4 for accuracy, only 2 had evidence of input from healthcare professionals (Table 3). If smartphone apps are to become a reliable and routine source of information for patients and healthcare professionals, it is essential that the content is accurate and appropriate. This is particularly important when apps may be used to influence behaviour, e.g. encouraging patients to adopt a specific diet. Low levels of health professional involvement in app design has been described in other specialties, and content has been found to lack appropriate academic reference and occasionally mislead [11, 19, 20]. In this review, we identified apps that recommend a low-calcium diet. This is not the current evidence-based recommendation, and may even be harmful [21].
In September 2013, the US Food and Drug Administration issued final guidance as to their oversight of mobile medical apps. They intend to focus their regulation on apps that are an accessory to a registered medical device or transform a smartphone platform into a medical device, e.g. an app that turns a smartphone into an ECG monitor [18]. As a result, none of the apps identified in this review would fall under this regulatory process despite the potential to offer inaccurate information.
It is not clear how medical apps will be regulated in the future. However, there are two simple measures that could be introduced to ensure patients and health professionals who can use apps related to urolithiasis with confidence. Firstly, the establishment of a ‘quality stamp’ provided by an international urology association. In a similar way to external peer review of research articles, app developers would submit their designs to be approved. Secondly, app stores should insist on full authorship disclosure, including any competing interests authors may have. These measures have been proposed before and would reassure consumers that an app was of sufficient scientific quality [11, 13].
There are two notable limitations of this study. Firstly, authorship disclosure within product summaries and apps themselves can be difficult to identify, therefore, the degree of health professional involvement may have been underestimated. However, it seems likely that if apps did have expert input, then this would be made clear to users as a positive feature. Secondly, the proliferation of smartphone apps is such that by the time this review is published, it will no longer describe the current availability.
Urolithiasis is a condition with unique and complex symptoms. For example, decisions such as surgical approach, and when and if to intervene, often depend largely on patients’ expectations of how their lives will be improved by such an intervention [22]. It is important that patients are able to understand the array of options, e.g. extracorporeal shockwave lithotripsy vs ureterorenoscopy. To make informed decisions about surgery, patients must receive sufficient and appropriate information, and also comprehend it [23]. It is feasible that an app could be developed that allows patients to navigate through the pros and cons of different treatment modalities for their stone after inputting their own patient and stone characteristics. Apps tailored to physicians could similarly offer the latest research at their fingertips during patient consultations.
Conclusion
Apps are an everyday part of many people’s lives. There are already a significant number of apps relating to urolithiasis. Unfortunately, lack of regulation means that the information can be misleading or even incorrect. It is important for medical specialists and their professional organisations to engage with this technology and to develop or regulate this field. If apps can have a ‘quality stamp’ as we have suggested, from a national urological organisation (e.g. American Urological Association, British Association of Urological Surgeons and European Association of Urology), healthcare professionals can have greater confidence in directing patients to this resource as an adjunct to a consultation on their stone disease. Future research should look to develop apps for urolithiasis that are safe, effective and fulfil a useful clinical purpose.
References
Franko OI (2011) Smartphone apps for orthopaedic surgeons. Clin Orthop Relat Res 469(7):2042–2048. doi:10.1007/s11999-011-1904-0
Smith A. Smartphone ownership —2013 update. Pew Research Centre Reports. 2013 June. http://www.pewinternet.org/~/media/Files/Reports/2013/PIP_Smartphone_adoption_2013.pdf. Accessed 09 Oct 2013
Makanjuola JK, Rao AR, Hale J, Bultitude M, Challacombe B, Dasgupta P (2012) Urology apps: a review of all apps available for urologists. BJU Int 110(4):475–477. doi:10.1111/j.1464-410X.2012.11200.x
D4(2007) A survey of mobile phone usage by health professionals in the UK. http://www.d4.org.uk/research/survey-mobile-phone-use-health-professionals-UK.pdf. Accessed 2 Dec 2012
Dasari KB, White SM, Pateman J (2011) Survey of iPhone usage among anaesthetists in England. Anaesthesia 66(67):630–631. doi:10.1111/j.1365-2044.2011.06747.x
Kailas A, Chong CC, Watanabe F (2010) From mobile phones to personal wellness dashboards. IEEE Pulse 1(1):57–63. doi:10.1109/MPUL.2010.937244
Barton AJ (2012) The regulation of mobile health applications. BMC Med 10:46. doi:10.1186/1741-7015-10-46
Fox S, Duggan M (2012) Mobile health. Pew internet & american life project http://www.pewinternet.org/Reports/2012/Mobile-Health.aspx. Accessed 9 Oct 2013
Janhs RG (2010) research2guidance. http://www.research2guidance.com/500m-people-will-be-using-healthcare-mobile-applications-in-2015/. Accessed 14 Oct 2013
Vos J, Parker C (2012) Medical device regulation: Health policy and position. GSMA connected living programme. http://www.gsma.com/connectedliving/wp-content/uploads/2012/03/gsmamedicaldeviceregulationmhealthpolicyandposition.pdf. Accessed 9 Oct 2013
O’Neill S, Brady RR (2012) Colorectal smartphone apps: opportunities and risks. Colorectal Dis 4(9):e530–e534. doi:10.1111/j.1463-1318.2012.03088.x
Freshwater MF (2011) iPhone and iPad applications for plastic surgeons. J Plast Reconstr Aesthet Surg 64(10):1397–1399. doi:10.1016/j.bjps.2011.06.020
Stevens DJ, Jackson JA, Howes N (2014) Obesity surgery smartphone apps: a review. Obes Surg 24(1):32–36. doi:10.1007/s11695-013-1010-3
Romero V, Akpinar H, Assimos D (2010) Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Rev Urol 12:e86–e96
Stamatelou K, Francis M, Jones C, Nyberg L, Curhan G (2003) Time trends in reported prevalence of kidney stones in the United States: 1976–1994. Kidney Int 63:1817–1823. doi:10.1046/j.1523-1755.2003.00917.x
Turney BW, Reynard JM, Noble JG, Keoghane SR (2012) Trends in urological stone disease. BJU Int 109(7):1082–1087. doi:10.1111/j.1464-410X.2011.10495.x
Gallagher S, Tedstone Doherty D, Moran R, Kartalova-O’Doherty Y (2008) Internet use and seeking health information online in Ireland: demographic characteristics and mental health characteristics of users and non users. In: HRB Research Series 4, Health Research Board, Dublin
Patel B (2013) Mobile medical applications—guidance for Industry and Food and Drug Administration Staff. http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM263366.pdf. Accessed 14 Oct 2013
Hamilton AD, Brady RR (2012) Medical professional involvement in smartphone ‘apps’ in dermatology. Br J Dermatol 167(1):220–221. doi:10.1111/j.1365-2133.2012.10844.x
Rosser BA, Eccleston C (2011) Smartphone applications for pain management. J Telemed Telecare 17(6):308–312. doi:10.1258/jtt.2011.101102
National Kidney and Urologic Diseases Information Clearinghouse (NKUDIC) (2013) Diet for Kidney Stone Prevention. US Department of Health and Human Services. http://kidney.niddk.nih.gov/Kudiseases/pubs/kidneystonediet/index.aspx. Accessed 18 Apr 2014
Penniston K, Nakada S (2013) Development of an instrument to assess the health related quality of life of kidney stone formers. J Urol 189(3):921–930. doi:10.1016/j.juro.2012.08.247
Faden RR, Beauchamp TL (1986) A history and theory of informed consent. Oxford University Press, New York
Conflict of interest
None of the authors declare a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Stevens, D.J., McKenzie, K., Cui, H.W. et al. Smartphone apps for urolithiasis. Urolithiasis 43, 13–19 (2015). https://doi.org/10.1007/s00240-014-0738-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-014-0738-0