
Abstract
The objective of the study was to compare the efficacy of dimethyl sulfoxide (DMSO) mixed with lignocaine and eutectic mixture of local anesthetics (EMLA) cream as topically applied surface anesthetics in relieving pain during shock wave lithotripsy (SWL) in a prospective randomized study. Of the 160 patients, 80 patients received DMSO with lignocaine and 80 patients received EMLA cream, applied to the skin of the flank at the area of entry of shock waves. SWL was done with Seimens lithostar multiline lithotripter. The pain during the procedure was assessed using visual analog and verbal rating scores. The mean visual analog scale scores for the two groups were 3.03 for DMSO group and 4.43 for EMLA group. The difference of pain score on visual analog scale was statistically significant (p < 0.05). Similarly, the pain scores as rated on the verbal rating scale were also evaluated; the mean score on verbal rating scale were 2.34 for DMSO group and 3.00 for the EMLA group. The difference between the pain score on verbal rating scale was also found to be statistically significant (p < 0.05). Our study showed that DMSO with lignocaine is a better local anesthetic agent for SWL than EMLA cream. The stone fragmentation and clearance rates are also better in the DMSO group.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Shockwave lithotripsy (SWL), since its approval by US food and drug administration (FDA) and introduction in clinical use in 1984, has been become a routine modality of treatment for urinary stones. The first-generation lithotripters caused pain and discomfort during the procedure, due to the shock wave entry at the cutaneous level. Hence, the procedure required general or epidural anesthesia. With the advent of second- and third-generation lithotripters the need for anesthesia has reduced, nevertheless the need for adequate analgesia still persists even with the second- and third-generation lithotripters. Several studies have been conducted to investigate the effect of different local anesthetic agents on therapy dependent pain with varying results [1–6].
Materials and methods
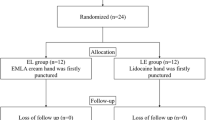
After institutional ethics committee approval and written informed consent, 160 patients scheduled to undergo elective SWL of kidney or upper ureteric stones were enrolled in this prospective randomized, controlled clinical trial. The patients enrolled for this study were randomly allotted to two groups, consisting 80 patients each. Patients in first group received 10 g of 50% dimethyl sulfoxide (DMSO) with lignocaine equal to that in lignocaine gel (prepared by our pharmacology section) 10 min prior to the beginning of ESWL session (DMSO group). Patients in the second group received 10 g of EMLA cream about 10 min prior to the starting treatment (EMLA group).The cream was applied in an area of around 200 cm [2] marked by the urologist. All the patients underwent SWL with the highest energy level which they could tolerate and the highest number of shocks which they could tolerate. Any additional pain was treated with intramuscular injection of diclofenac and intravenous injection of benzodiazepines as required. The first session of lithotripsy was kept for 30 min after which patients were given a proforma to be filled by them which indicated the pain scores in both visual analog scores and verbal rating scores. At the end, the stone fragmentation rates were determined by comparing pre- and post-SWL X-ray findings. The stone fragmentation was rated on a scale of 0 to +4.
SWL was done with Seimens lithostar multiline lithotripter giving a maximum energy level of 4 joules with the shock rate of 2 shocks per second. The maximum of 4,000 shocks were given in a single sitting.
Difference in pain score, number of shock waves, energy level used, and duration of treatment was evaluated using the Mann–Whitney U test. Chi- square test was also be used for statistical analysis of difference for stone fragmentation rates.
Results
There was no statistical difference between the two groups regarding age, sex, stone burden or stone location (Table 1). Of the 80 patients in DMSO group, 58 were men and 22 were women with a mean age of 38.2 ± 11.9 years. In this group, 66 patients had renal stone and 14 had ureteric stone with a mean size of 0.95 ± 0.22 cm. In DMSO group, 64 were men and 16 were women with a mean age of 38.6 ± 13.8 years. In this group, 70 patients had renal stone and 10 had ureteric stone with a mean size of 0.90 ± 0.32 cm.
The average number of applied shock waves was 3,449 ± 211 in DMSO group and 3,156 ± 323 in EMLA group (p < 0.05). The mean energy level used in the DMSO group (3.4 ± 0.38 kv) was more than that used in the EMLA group (2.95 ± 0.43 kv) and the difference was statistically significant (p < 0.05).
The mean fragmentation score in the DMSO group (2.7 ± 0.7) was significantly higher compared to that in the EMLA group (1.7 ± 0.7; p < 0.05). The mean visual analog scale scores for the two groups were 3.0 ± 1.1 for DMSO group and 4.4 ± 1.8 for EMLA group (p < 0.05). The mean scores on verbal rating scale were 2.3 ± 0.7 for DMSO group and 3.0 ± 1.1 for the EMLA group (p < 0.05; Table 2).
Discussion
With the trend towards minimal invasive therapy for kidney stones, SWL stands out as a very important tool in the armamentarium of the urologist for treating renal and ureteric stones. One of the most important side effects related to SWL is the shock wave related pain that occurs during the procedure due to the entry of shock waves at the level of skin. With the first-generation lithotripters, the procedure was done under general anesthesia or epidural analgesia which required hospital admission. With improvement in technology related to shock wave and introduction of second- and third-generation lithotripters, it was possible to perform SWL on an out-patient basis without the need for general or spinal anesthesia. Nevertheless, SWL without anesthesia demands proper pain management of shock wave related pain to ensure patient relaxation, co-operation, and satisfaction since patient relaxation and co-operation is required for proper stone localization for adequate stone fragmentation during the procedure.
Various sedative and analgesic medications have been used for SWL. Variable results related to the efficacy of local and topical anesthesia with EMLA cream have been reported [2, 4, 7]. In one of the studies, EMLA group was reported to need less fentanyl (23%) and have less pain compared to placebo, but the difference was not statistically significant [8]. In another study done by Monk et al. [9], which compared the EMLA cream with intravenous fentanyl during SWL, EMLA cream reported to have cutaneous analgesia, but failed to demonstrate any opoid sparing effect. In another study done with first-generation lithotripters, McDonald and Berry [7] found EMLA cream to be comparable to placebo.
Dimethyl sulfoxide, a polar solvent, used frequently as an industrial solvent, was shown to have a local anesthetic and analgesic action [10]. There has been extensive research on its pharmacological actions. On local application, DMSO is rapidly absorbed from the skin. Experiments in animal model have shown that radioactivity appears in blood 5 min after cutaneous application of DMSO. In our study, we have applied DMSO 10 min prior to the procedure, while EMLA cream was applied 60 min prior to the procedure. DMSO has shown to prolong conduction velocity in the C fibers conducting pain. Experiments on nerve conduction have shown that the nerve conduction was decreased by 40% when sciatic nerve was immersed in 6% DMSO, and the effect was totally reversed when nerve was washed with a buffer for 1 h [11]. Shealy [12] studied the peripheral small fiber after discharge in cats. Concentrations of 5–10% DMSO eliminated the activity in C fibers within 1 min. The effect was totally reversed after DMSO was washed away. Haigler [13] demonstrated that the DMSO produced analgesia by both acting locally and systemically, DMSO had duration of action greater than morphine, 6 versus 2 h, respectively. In our study, DMSO had shown significantly lower pain scores both on verbal rating scale and on visual analog scale compared to EMLA cream.
Experiments have also demonstrated that the DMSO has a diuretic action [7]. In rats, 0.5 mL of 90% of DMSO applied topically had shown to increase the urine volume by tenfold. There was an increase in sodium and potassium excretion also. Probably, this pharmacological action was also a reason for the significantly higher stone fragmentation rates seen in the group receiving DMSO with lignocaine when compared to the group receiving EMLA cream in our study.
Conclusion
Our study has shown that DMSO with lignocaine to be a more effective local anesthetic, analgesic agent compared to EMLA cream during SWL. Apart from the good analgesic action, patients receiving DMSO with lignocaine had better stone fragmentation rates when compared to the patients receiving EMLA cream. Patients receiving DMSO with lignocaine could tolerate higher amount of energy and higher number of shockwaves compared to the patients receiving EMLA cream. From our experience, we advocate the use of DMSO with lignocaine for SWL to provide adequate analgesia and local anesthesia, better fragmentation and probably better stone clearance.
References
Aekins B, Fritz KW, Hoene E (1986) Initial experience with local anesthesia in extra corporeal shock wave lithotripsy. Urologia Internationalis 41:246–247
Honnes de Lichtenberg M, Miskowiak J, Mogensen P et al (1992) Local anaesthesia for extracorporeal shock wave lithotripsy: a study comparing eutectic mixture of local anesthetics cream and lidocaine infiltration. Journal of Urology 147:96–97
Loening S, Kramolowsky EV, Willoughby B (1987) Use of local anaesthesia for extracorporeal shock wave lithotripsy. Journal of Urology 137:626–628
Tiselius HG (1993) Cutaneous anaesthesia with lidocaine-prilocaine cream: a useful adjunct during shock wave lithotripsy with analgesic sedation. Journal of Urology 149:8–11
London RA, Kudlak T, Riehle RA (1986) Immersion anaesthesia for extracorporeal shock wave lithotripsy review of two hundred twenty treatments. Urology 28:86–94
Demir E, Kilciler M, Bedir S et al (2007) Comparing two local anaesthesia techniques for extracorporeal shock wave lithotripsy. Urology 69:625–628
McDonald PF, Berry AM (1992) Topical anaesthesia for extracorporeal shock wave lithotripsy. British Journal of Anaesthesia 69:399–400
Bierkens AF, Maes RM, Hendrikx JM et al (1991) The use of local anesthesia in second generation extracorporeal shock wave lithotripsy. Eutectic mixture of local anesthetics. Journal of Urology 146:287–289
Monk TG, Ding Y, White PF et al (1994) Effects of topical local anesthetics on pain response and analgesics requirements during lithotripsy procedures. Anaesth Analg 79:506–511
Weissmen G, Sessa G, Bevans V (1967) Effect of DMSO on the stabilization of lysosome by cortisone and chloroquine in vitro. Annals of the New York Academy of Sciences 14:326–332
Sams WM (1967) The effects of DMSO on nerve conduction. Annals of the New York Academy of Sciences 141:242–247
Shealy CN (1996) The physiological substrate of pain. Headache 6:101–108
Haigler HJ (1983) Comparison of analgesic effects of DMSO and morphine. Annals of the New York Academy of Sciences 411:19–27
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kumar, S., Kumar, S., Ganesamoni, R. et al. Dimethyl sulfoxide with lignocaine versus eutectic mixture of local anesthetics: prospective randomized study to compare the efficacy of cutaneous anesthesia in shock wave lithotripsy. Urol Res 39, 181–183 (2011). https://doi.org/10.1007/s00240-010-0324-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-010-0324-z