
Abstract
Renal manifestations of chronic hyperoxaluria include nephrolithiasis and, when extreme, interstitial scarring and progressive loss of function. Exposure of cultured renal cells to oxalate has been reported to cause cell death, as well as proliferation. The current study was performed to assess the time course and cell-type specificity of these responses. Proximal (LLC-PK1) and distal [cIMCD and primary human renal (HRC1)] renal epithelial cells, as well as interstitial KNRK cells, were exposed to oxalate (0.5–2.0 mM) for 24–72 h. The generation of reactive oxygen species (ROS) was measured using the fluorescent probe DCF, and cell number was determined with CyQuant reagent. HSP-70 expression was assessed via real time PCR and quantitative Western blot. In response to all oxalate concentrations (0.5–2.0 mM) and lengths of exposure (15 min–2 h), cultured proximal and distal renal epithelial cells and renal fibroblasts generated ROS. After 24 h, cells demonstrated initial cell death and decrease in cell numbers, but by 48–72 h adapted and grew, despite the continued presence of oxalate. This response was associated with increased expression of HSP-70 mRNA and protein. Renal cells in vivo may possess adaptive mechanisms to withstand chronic hyperoxaluria, including increased expression of chaperone molecules such as HSP-70.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Renal manifestations of chronic hyperoxaluria include nephrolithiasis and, when extreme, interstitial scarring and progressive loss of function. The clinical outcome in many patients with primary hyperoxaluria, a genetic disorder characterized by hepatic overproduction of oxalate, is dismal because multiple complications of the disease develop including nephrolithiasis, nephrocalcinosis and renal failure often resulting in death at a young age [1, 2]. Although primary hyperoxaluria is relatively rare, hyperoxaluria secondary to gastrointestinal malabsorption is not [3], and in these circumstances oxalosis is also sometimes observed [4]. Furthermore, the formation of kidney stones is extremely common [5], and evidence suggests that minimal, perhaps transient elevations in urinary oxalate concentration may be an important factor in at least a subgroup of patients with idiopathic calcium oxalate urolithiasis [6].
In the cases of primary and secondary hyperoxaluria, oxalate appears to be a key mediator of renal manifestations that include tubulointerstitial scarring as well as nephrolithiasis [4, 7]. For patients with idiopathic calcium oxalate stone disease and mild hyperoxaluria, it has been postulated that stimulation of these same pathways can result in a local nidus for stone formation [8]. Since different regions of the kidney are likely to be exposed to different oxalate concentrations [9], in the current study we defined cell-type responses to oxalate, including reactive oxygen species (ROS) generation, cell growth, and induction of a representative stress response protein.
Materials and methods
Cell culture
Rat continuous inner medullary collecting duct (cIMCD) cells were a generous gift of Dr Jack Kleinman, Medical College of Wisconsin, Milwaukee, WI, and porcine proximal tubular LLC-PK1 cells a gift of Dr. Thomas Dousa, Mayo Clinic, Rochester, MN. Mouse renal fibroblastic KNRK cells were obtained from the American Tissue Culture Collection (CL-101).
Human renal cells were isolated from the urine of a healthy, non-stone forming male using the method of Dörrenhaus [10]. Briefly, a fresh urine sample (50 ml) was centrifuged 100 g for 5 min), and rinsed twice with Hams F-12 culture medium containing penicillin (100 U/ml), streptomycin (100 μg/ml), amphotericin (1.25 μg/ml) and 20% calf serum. The resulting pellet was resuspended in 50 μl of medium and seeded in a single well of a 24-well collagen-coated plate (Falcon) to which an additional 50 μl of medium was placed. Wells were fed with an additional 100 μl of medium the following day, and the medium replaced every 2–3 days thereafter. Once confluent, cells were trypsinized and replated onto other collagen-coated wells. Resulting cell lines were then propagated on standard Falcon plates in DMEM with 10% calf serum. One line (HRC1) was fully characterized for these studies. HRC1 cells formed a uniform tight monolayer, stained with lectins from Jacalin, Concanavalin A, but not Vicia villosa (VVL), Erythrina crystagalli (ECA) or Griffonia simplficolia (GSII). Alkaline phosphatase activity was also detected. Together, the evidence is most consistent that the cells are a primary culture of distal renal cells [11].
Stock plates were grown in Dulbecco-Vogt modified Eagle’s medium containing 25 mM glucose (DMEM) and 10% fetal calf serum at 37°C in a CO2 incubator as previously described [12]. For assays in 96 well plates, cells were trypsinized and resuspended in DMEM containing 1.6 μM biotin and 5% (cIMCD, KNRK, HRC1) or 10% (LLC-PK1) fetal calf serum at a density designed to achieve an initial confluence of ~50%. Initial plating densities were approximately 25×104 cells/ml (HRC1), 30×104 cells/ml (cIMCD and KNRK), and 50×104 cells/ml (LLC-PK1). After 8 h, the media was changed to DMEM containing 0.05% fatty acid free bovine serum albumin (BSA, Sigma) and 1.6 µM biotin. The media was changed daily for three more days with DMEM 0.05% BSA and 1.6 µM biotin. On day 4, when cells had reached 75–85% confluence, they were exposed to vehicle or potassium oxalate (0.1–2.0 mM) prepared in phenol red free DMEM (BioWhittaker) plus 0.05% BSA and 1.6 µM biotin. For exposures longer than 24 h, media was changed daily with fresh medium containing the same oxalate concentrations.
Detection of reactive oxygen species
The peroxide sensitive fluorescent probe, 2′,7′-dichlorofluorescin diacetate (DCF-DA) was used to assess the generation of reactive oxygen species (ROS) [13]. Briefly, cells were plated into 96 well plates containing phenol red-free DMEM and 1% fetal calf serum. After equilibration and attachment, the medium was changed to Earle’s balanced salt solution containing 10 µM DCF-DA (Molecular Probes) and 1% bovine serum albumin for 30 min at 37˚C. The medium was then removed and replaced with fresh phenol red free DMEM containing 0.05% BSA and 1.6 µM biotin to which vehicle or potassium oxalate (0.1–2.0 mM) was added. Relative fluorescence intensity measurements were obtained over time (15–120 min) by fluorometry using a Fusion-α Fluorometer containing a 96 well plate reader (Packard Instruments Downers Grove, Ill., USA). Fluormetric readings were obtained using an excitation wavelength of 485 nm and emission wavelength of 530 nm.
Quantification of cell proliferation
To quantitate cell proliferation, cells were plated into 96 well plates in phenol red-free DMEM containing 2% fetal calf serum at the densities indicated above. After 1 day, media was changed to phenol red free DMEM containing 0.05% BSA. The following day (day 2), and each subsequent day the media was changed to phenol-red free DMEM that contained potassium oxalate (0.5–2.0 mM) or vehicle. On days 3, 4, and 5, media was aspirated and plates were frozen to −80°C to lyse cells. To quantitate cell number, plates were thawed and 50 μl of CyQuant reagent (Molecular Probes) was added to each well. Plates were incubated at room temperature for 5 min prior to measuring relative fluorescence (480 nm excitation, 530 nm emission).
Live/dead staining
For live/dead staining, cells were plated on glass coverslips in 24-well dishes at the same densities and conditions as above. After exposure to potassium oxalate (0.5–2.0 mM) for 4 or 24 h, media was aspirated and replaced with 200 μl of Live/Dead mix and placed in the dark for 40 min at room temperature. Excess stain was then blotted off, and coverslips mounted on glass slides using fluorescent mounting medium. One hundred cells per slide were counted for live/dead staining using a fluorescence microscope. For live staining (calcein), absorbance was set at 494 nm and emission at 517 nm; for dead staining (ethidium homodimer-1) absorbance was at 528 nm and emission at 617 nm.
HSP-70 expression
HRC1 cells were grown as above in 100-mm dishes and exposed to two concentrations of oxalate chosen to model mild and extreme hyperoxaluria (0.5 and 2.0 mM), for 4, 24 and 48 h each. Cells were then harvested for total RNA using the Trizol reagent (Invitrogen), and cDNA was prepared using the SuperScript II kit (Invitrogen). Primer pairs were constructed using the human sequences in the database for 18sRNA and HSP-70 (Table 1). PCR conditions were optimized for each so that a single PCR product was obtained on gel electrophoresis, as verified using cDNA prepared from control cells as a template. Real-time quantitative PCR (RT-PCR) was performed using the SYBR Green JumpStart Taq ReadyMix (Sigma) and the Opticon DNA engine (MJ Research). Gene expression under each condition was normalized for 18sRNA, and expressed relative to the matched controls.
Quantitative Western blots for HSP-70
Cells were grown in 24-well plates and exposed to oxalate as above. The medium was aspirated and the monolayer rinsed once with ice-cold phosphate-buffered saline (pH 7.4) prior to the addition of 1× cell culture lysis reagent (200 μl, Promega, Madison, Wis.) after which cells were scraped and vortexed for lysis. The resulting cell lysate was centrifuged at 10,000 g for 2 min in a refrigerated centrifuge, and the supernatant collected and stored at −80°C. At the time of assay this lysate was thawed, mixed with two parts of SDS-PAGE sample buffer, boiled in a water-bath for 3 min, and the proteins were resolved on 4–12% Bis-Tris gradient gels (NuPage, Invitrogen). Gels were electroblotted onto an Immobilon-P membrane (Millipore, Bedford, Mass.), stained with Coommasie blue, and probed for HSP-70 using a monoclonal anti-HSP70 antibody (Sigma, St. Louis, Mo.). Signals of the appropriate size (70 kDa) were densitometrically quantified using a Kodak Gel Logic 100 imaging system (Eastman Kodak, Rochester, N.Y.). Each sample was run in triplicate and averaged.
Materials
Reagents were purchased from Sigma unless otherwise indicated.
Statistics
Data were compared by Student’s t-test; P values <0.05 were accepted as significant. Values presented are means±SEM. Points on graphs are each the mean of 16 or more values (n=8 for each experiment performed at least twice). For real time PCR, results are the mean of two separate experiments (oxalate exposure, RNA isolation and real time PCR).
Results
Renal cells generate ROS in response to oxalate exposure
As assessed using DCF, all four renal cell lines generated ROS within 1 h in response to a moderate and acute oxalate exposure (0.5 mM×1 h, Fig. 1A). ROS could be detected within 15 min, and persisted for the full 2 h studied. In general, at all time points ROS generation was greater for the three epithelial cell lines than KNRK cells, and greatest for the HRC1 line (Fig. 1B). When measured at 1 h, there was no clear relationship between the quantity of ROS generation and oxalate concentration, although the highest percent increases were in general at the highest oxalate level studied (2.0 mM).

Generation of ROS by cultured renal cells. Cells were exposed to oxalate (0.1–2.0 mM) for times ranging between 15 and 120 min, and ROS generation was assessed using DCF. All cells demonstrated increased ROS levels in response to oxalate (0.5 mM) for 1 h (A), although KNRK cells generated a smaller percentage increase. ROS were detected as early as 15 min after 0.5 mM oxalate exposure, and there was no clear trend for further increase up to 2 h later (B). After 1 h exposure, cells generated ROS in response to oxalate concentrations of between 0.5 and 2.0 mM, without any clear trend for increased levels in response to higher oxalate levels (C)
Cell growth in the presence of oxalate
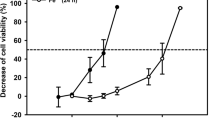
Apoptosis, cell death and DNA synthesis have all been reported in response to acute oxalate exposure. Therefore, we determined the effect of a prolonged oxalate exposure on these disparate cell lines. For all four cell types, cell numbers were lower after 24 h exposure to the higher oxalate concentrations studied (1.0–2.0 mM, Figs. 2, 3, 4, 5). By 48–72 h, however, numbers were similar to the control for cells exposed to all levels of oxalate. Live/dead staining confirmed that there were an increased number of dead cells at 24 h in those exposed to the higher concentrations of oxalate (that also had reduced cell numbers), however, the number of dead cells returned to baseline at 48 and 72 h, and in all instances was the same as control values at these later times (not shown). There was no clear cell-type difference in sensitivity to the effects of oxalate, expect for the suggestion that KNRK cells might exhibit a proliferative response to moderate oxalate levels (0.5 mM), with some persistent toxicity at higher levels and prolonged time lines (2.0 mM for 72 h, Fig. 5).

Growth of LLCPK1 cells in the presence of oxalate. Cells were exposed to oxalate (0.5–2.0 mM) from time 0. At 24, 48, and 72 h cell counts were assessed fluorimetrically using the CyQuant reagent. Cell numbers were reduced in the presence of the higher concentrations of oxalate at 24 and 48 h, but by 72 h cell numbers were similar to control wells never exposed to oxalate. An asterisk indicates P<0.05 vs control

Growth of cIMCD cells in the presence of oxalate. Cells were exposed to oxalate (0.5–2.0 mM) from time 0. At 24, 48, and 72 h cell counts were assessed fluorometrically using the CyQuant reagent. Cell numbers were reduced in the presence of the higher concentrations of oxalate at 24 but not 48 or 72 . An asterisk indicates P<0.05 vs control

Growth of HRC1 cells in the presence of oxalate. Cells were exposed to oxalate (0.5–2.0 mM) from time 0. At 24, 48, and 72 h cell counts were assessed fluorometrically using the CyQuant reagent. Cell numbers were reduced in the presence of the higher concentrations of oxalate at 24 and 48, but not 72 h. An asterisk indicates P<0.05 vs control

Growth of KNRK cells in the presence of oxalate. Cells were exposed to oxalate (0.5–2.0 mM) from time 0. At 24, 48, and 72 h cell counts were assessed fluorometrically using the CyQuant reagent. Cell numbers were reduced in the presence of the higher concentrations of oxalate at 24 h, and increased at moderate oxalate exposure (0.5 mM) at 72 h. An asterisk indicates P<0.05 vs control
HSP-70
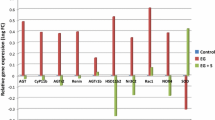
Given the ability of cells to recover and proliferate in the presence of even high concentrations of oxalate, we next looked at HSP-70 expression as an index of stress response. As assessed by real time PCR, HSP-70 gene expression was induced after 24 h exposure to 0.5 mM (nine-fold) and 2.0 mM (27-fold) oxalate, then returned close to baseline by 48 h (Fig. 6A). HSP-70 protein levels were also increased in whole cell lysates both 24 and 48 h after oxalate exposure (10–30%; Fig. 6B), although the difference reached statistical significance only for 2.0 mM oxalate at 24 h. Therefore, HSP-70 induction could be part of a protective response induced by prolonged oxalate exposure.

HSP-70 gene and protein expression after oxalate exposure. A Expression of the gene encoding HSP-70 was upregulated at 24 h after exposure to oxalate (0.5 or 2.0 mM). HSP-70 protein expression, measured by quantitative Western blots of whole cell lysates, was also increased by 10–30% 1 or 2 days after oxalate exposure, but was significant only for 2.0 mM oxalate at 24 hours (B). An asterisk indicates P<0.05
Discussion
Other investigators have hypothesized that tubular cell injury occurs following oxalate exposure, setting into motion a series of events that can result in kidney stone formation, or promote renal scarring when hyperoxaluria exposure is extreme and/or prolonged. [8]. However, many of the toxic effects of oxalate on renal cells were observed in cell culture systems, and the most dramatic adverse effects occurred when relatively high oxalate concentrations were employed [14, 15]. Furthermore, greater toxicity was reported in proximal compared to distal tubular-derived cell lines [16]. In vivo, most observations have been made in rats made hyperoxaluric by administration of ethylene glycol in the drinking water [17], under conditions of high urinary oxalate concentration which could not be precisely controlled, and where metabolites of ethylene glycol other than oxalate could have contributed to the cellular toxicity that was observed.
With these caveats in mind, numerous studies suggest that acute exposure to high concentrations of oxalate, similar to those seen in the urine of primary or secondary hyperoxaluric patients, can injure cultured renal tubular cells in the absence of crystal formation [14, 15, 16]. In lower concentrations oxalate ions induce cellular proliferation [18]. Prior evidence also suggests that oxalate ions damage cells via oxidative pathways [19, 20], and a recent study indicates that diphenyleneiodium (DPI) can ameliorate oxalate ion, calcium oxalate monohydrate crystal and brushite crystal induced up-regulation of the inflammatory cytokine MCP-1 in NRK 52E cells [21]. Since NADPH oxidase subunits are known to be present in renal epithelial cells, this pathway is implicated as a source of ROS in cells exposed to oxalate [22]. Consistent with other studies using cultured renal cells, our investigation confirmed that diverse renal cell types can generate ROS in response to acute oxalate exposure. Marked cell-type differences were not observed, although interstitial KNRK cells generated less ROS at all oxalate concentrations and times of exposure (Fig. 1). Perhaps these fibroblastic cells lack important cell membrane transporters or channels to allow efficient oxalate entry into the cytoplasm.
Overall, after an acute oxalate exposure, our most striking finding was that surviving cells went on to proliferate normally, without further toxicity. These events correlated with enhanced expression of the stress response chaperone HSP-70. Cell death is not a feature of renal tissue derived from patients with nephrolithiasis, or even primary or secondary hyperoxaluria [23]. Although urinary oxalate excretion can vary in relation to the timing of meals [6], it is likely that renal cells in vivo are continuously exposed to an ambient baseline level of oxalate. Our experiments suggest that cells are able to adapt and even proliferate under these circumstances. In some ways, this situation could be analogous to adaptive responses of inner medullary cells to markedly hyperosmolar conditions [24, 25].
It is possible that crystals may be initiating some of the pathologic changes observed under hyperoxaluric conditions in vivo. Calcium oxalate crystals can induce renal epithelial cellular proliferation both in culture models [12] and in vivo [7], but may also cause renal cell injury when present at high concentrations [16]. Once a calcium oxalate crystal is attached, endocytosis [26] appears to be followed by transport of the crystal to the tubulo-interstitium where an inflammatory response is initiated with recruitment of lymphocytes, macrophages, and fibroblasts [27], perhaps leading to renal scarring. Importantly, interstitial inflammation and fibrosis associated with crystal deposition have been observed in renal tissue of hyperoxaluric patients who developed renal insufficiency [4, 7].
In conclusion, both proximal and distal renal cells, as well as fibroblasts, generate ROS in response to oxalate exposure. Cells demonstrate initial cell death and decrease in cell numbers, but by 48–72 h adapt and grow, despite the continued presence of oxalate. This adaptive response may involve chaperones such as HSP-70. Renal cells in vivo may have similar mechanisms to withstand chronic hyperoxaluria.
References
Hockaday TDR, Clayton JE, Frederick EW (1964) Primary hyperoxaluria. Medicine 43: 315
Latta K, Brodehl J (1990) Primary hyperoxaluria type I. Eur J Pediatr 149: 518
Pardi DS, Tremaine WJ, Sandborn WJ, McCarthy JT (1998) Renal and urological complications of inflammatory bowel disease. Am J Gastroenterol 93: 500
Mandell I, Krauss E, Millan JC (1980) Oxalate-induced acute renal failure in Crohn’s Disease. Am J Med 69: 628
Unwin R, Wrong O, Cohen E, Tanner M, Thakker R (1996) Unraveling of the molecular mechanisms of kidney stones. Lancet 348: 1561
Smith LH (1994) Diet and hyperoxaluria in the syndrome of idiopathic calcium oxalate urolithiasis. Am J Kidney Dis 17: 370
Lieske JC, Spargo B, Toback FG (1992) Endocytosis of calcium oxalate crystals and proliferation of renal tubular epithelial cells in a patient with type 1 primary hyperoxaluria. J Urol 148: 1517
Kumar S, Sigmon D, Miller T, Carpenter B, Khan S, Malhotra R, Scheid C, Menon M (1991) A new model of nephrolithiasis involving tubular dysfunction/injury. J Urol 146: 1384
Hautmann R, Lehmann A, Komor S (1980) Calcium and oxalate concentrations in human renal tissue: the key to the pathogenesis of stone formation. J Urol 123: 317
Dörrenhaus A, Müller JIF, Golka K, Jedrusik P, Schulze H, Föllmann W (2000) Cultures of exfoliated epithelial cells from different locations of the human urinary tract and the renal tubular system. Arch Toxicol 74: 618
Grupp C, John H, Hemprich U, Singer A, Munzel U, Muller GA (2001) Identification of nucleated cells in urine using lectin staining. Am J Kid Dis 37: 84
Lieske JC, Walsh-Reitz MM, Toback FG (1992) Calcium oxalate monohydrate crystals are endocytosed by renal epithelial cells and induce proliferation. Am J Physiol 262: F622
Greene EL, Velarde V, Jaffa AA (2000) Role of reactive oxygen species in bradykinin-induced mitogen-activated protein kinase and c-fos induction in vascular cells. Hypertension 35: 942
Scheid C, Koul HK, Kennington L, Hill WA, Luber-Narod J, Jonassen J, Honeyman T, Menon M (1995) Oxalate-induced damage to renal tubular cells. Scanning Microsc 9: 1097
Scheid C, Koul H, Hill WA, Luber-Narod J, Jonassen J, Honeyman T, Kennington L, Kohli R, Hodapp J, Ayvazian P, Menon M (1996) Oxalate toxicity in LLC-PK1 cells, a line of renal epithelial cells. J Urol 155: 1112
Hackett RL, Shevock PN, Khan SR (1994) Madin-Darby canine kidney cells are injured by exposure to oxalate and calcium oxalate crystals. Urol Res 22: 197
Khan SR, Hackett RL (1993) Hyperoxaluria, enzymuria and nephrolithiasis. Contrib Nephrol 101: 190
Jonassen J, Cooney R, Kennington L, Gravel K, Honeyman T, Scheid C (1999) Oxalate-induced changes in the viability and growth of human renal epithelial cells. J Am Soc Nephrol 10: S446
Scheid CR, H. K, Hill WA, Lieske JC, Toback FG, Menon M (1996) Oxalate ion and calcium oxalate crystal interactions with renal epithelial cells. In: Coe FL, Favus MJ, Pak CYC, Parks JH, Preminger GM (eds) Kidney stones: medical and surgical management. Lippincott-Raven, Philadelphia, p 129
Koul H, Kennington L, Nair G, Honeyman T, Menon M, Scheid C (1994) Oxalate-induced initiation of DNA synthesis in LLC-PK1 cells, a line of renal epithelial cells. Biochem Biophys Res Commun 205: 1632
Umekawa T, Byer K, Uemura H, Khan SR (2005) Diphenyleneiodium (DPI) reduces oxalate ion- and calcium oxalate monohydrate and brushite crystal-induced upregulation of MCP-1 in NRK 52E cells. Nephrol Dial Transplant 20: 870
Shiose A, Kuroda J, Tsuruya K, Hirai M, Hirakata H, Naito S, Hattori M, Sakaki Y, Sumimoto H (2001) A novel superoxide-producing NAD(P)H oxidase in kidney. J Biol Chem 276: 1417
Evan AP, Lingeman JE, Coe FL, Parks JH, Bledsoe SB, Shao Y, Sommer AJ, Paterson RF, Kuo RL, Grynpas M (2003) Randall’s plaque of patients with nephrolithiasis begins in basement membranes of thin loops of Henle. J Clin Invest 111: 602
Zhang Z, Cai Q, Michea L, Dmitrieva NI, Andrews P, Burg MB (2002) Proliferation and osmotic tolerance of renal inner medullary epithelial cells in vivo and in cell culture. Am J Physiol Renal Physiol 283: F302
Cowley BD Jr, Muessel MJ, Douglass D, Wilkins W (1995) In vivo and in vitro osmotic regulation of HSP-70 and prostaglandin synthase gene expression in kidney cells. Am J Physiol 269: F854
Lieske JC, Swift HS, Martin T, Patterson B, Toback FG (1994) Renal epithelial cells rapidly bind and internalize calcium oxalate monohydrate crystals. Proc Natl Acad Sci U S A 91: 6987
De Water R, Noordermeer C, Van der Kwast TH, Nizze H, Boeve ER, Kok DJ, Schroder FH (1999) Calcium oxalate nephrolithiasis: effect of renal crystal deposition on the cellular composition of the renal interstitium. Am J Kidney Dis 33: 761
Acknowledgments
This work was supported by grants to J.C.L. and E.L.G. from the National Institutes of Health (DK 53399, DK 60707), the Oxalosis and Hyperoxaluria Foundation (J.C.L.), the Robert Wood Johnson Foundation (E.L.G.) and the Mayo Foundation (J.C.L. and E.L.G.).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Greene, E.L., Farell, G., Yu, S. et al. Renal cell adaptation to oxalate. Urol Res 33, 340–348 (2005). https://doi.org/10.1007/s00240-005-0491-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-005-0491-5