
Abstract
Purpose
Preoperative identification of the artery of Adamkiewicz can help prevent postoperative spinal cord injury following thoracic and thoracoabdominal aortic repair. Several studies have demonstrated the feasibility of evaluating the artery of Adamkiewicz using multi-detector row computed tomography (CT), but precise visualization remains a challenge. The present study was conducted to evaluate the usefulness of ultra-high-resolution CT for visualizing the artery of Adamkiewicz with a slice thickness of 0.25 versus 0.5 mm in patients with aortic aneurysms.
Methods
Our institutional review board approved this study. Twenty-four patients with thoracic and thoracoabdominal aneurysms were scanned with beam collimation of 0.25 mm × 128. Images were reconstructed with slice thicknesses of 0.25 and 0.5 mm. The signal-to-noise ratio (SNR) of the aorta and contrast-to-noise ratio (CNR) between the anterior spinal artery and spinal cord were measured. Two independent observers evaluated visualization of the artery of Adamkiewicz and its continuity between the anterior spinal artery and the aorta using a four-point scale.
Results
No significant differences in the SNR of the aorta or CNR of the anterior spinal artery were observed between 0.25- and 0.5-mm slices. The average visualization score was significantly higher for 0.25-mm slices (3.58 ± 0.78) than for 0.5-mm slices (3.13 ± 0.99) (p = 0.01). The percentage of patients with nondiagnostic image quality was significantly lower for 0.25-mm slices (8.3%) than for 0.5-mm slices (33.3%) (p = 0.03).
Conclusion
In patients with aortic aneurysms, ultra-high-resolution CT with 0.25-mm slices significantly improves visualization of the artery of Adamkiewicz compared to 0.5-mm slices.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Spinal cord injury (SCI) is one of the most devastating complications in thoracic and thoracoabdominal aortic repair. Despite the introduction of many approaches in the operative procedures for aortic aneurysms, SCI remains a major problem, with a non-negligible incidence rate ranging from 0.2 to 8% [1,2,3]. It is known that the underlying cause of SCI is ischemia related to the anterior spinal artery in most cases. In the thoracolumbar spinal cord, the main feeder of the anterior spinal artery is the artery of Adamkiewicz (the great anterior radiculomedullary artery). Several studies have shown that identification of the artery of Adamkiewicz permits better preoperative planning, including modification of the surgical procedure, and thus may reduce the risk of SCI [4,5,6].
Multi-detector row computed tomography (CT) has been suggested as an attractive noninvasive imaging modality for such preoperative evaluation. Although CT has a high visualization rate for the characteristic “hairpin turn” configuration formed by the artery of Adamkiewicz and the anterior spinal artery, it would be desirable to obtain a clearer understanding of the entire anatomical course of the artery, including its connections with other vascular structures. This so-called “continuity” criterion, which includes demonstration of the vascular continuity of the anterior spinal artery, the artery of Adamkiewicz, the radiculomedullary artery, the segmental artery, and the aorta, remains a challenge in CT. Indeed, while detection rates in the range from 80 to 90% have been reported for the hairpin turn configuration criterion, the rates for the vascular continuity criterion are considerably lower, ranging from 29 to 60% [7,8,9,10,11]. In the identification of the artery of Adamkiewicz with CT, it is important to distinguish the artery of Adamkiewicz from the anterior radiculomedullary vein because this vein is very similar in shape to the artery of Adamkiewicz. Therefore, diagnosis based on the vascular continuity criterion is important to differentiate the artery of Adamkiewicz from the anterior radiculomedullary vein in the clinical setting.
Recently, a 128-detector row ultra-high-resolution CT scanner with a detector row width of 0.25 mm and a 1024 × 1024 matrix has been introduced in the clinical setting [12]. The higher spatial resolution of this CT scanner may be particularly advantageous for the visualization of smaller structures such as the artery of Adamkiewicz, which is approximately 1 mm in diameter. Therefore, the present study was conducted to evaluate the usefulness of ultra-high-resolution CT for visualizing the artery of Adamkiewicz in patients with aortic aneurysms.
Materials and methods
Patients
Our institutional review board approved this retrospective study. A total of 24 consecutive patients (18 men and 6 women; age range, 44–85 years; mean age, 68.5 years) who underwent ultra-high-resolution CT angiography for aortic disease between December 2015 and August 2016 were enrolled in the study. The indication for CT examination was the preoperative evaluation of thoracic or thoracoabdominal aortic aneurysm. The aortic diseases included true aortic aneurysms in 15 patients (8 thoracic descending aortic aneurysms and 7 thoracoabdominal aortic aneurysms) and dissecting aortic aneurysms in 9 patients. The patient characteristics are shown in Table 1. Written informed consent to undergo enhanced CT examination was obtained from all patients. The exclusion criteria were impaired renal function (estimated glomerular filtration rate of < 45 mL/min/1.73 m2) or allergy to contrast medium, but no patients met either of these exclusion criteria.
CT data acquisition and image reconstruction
CT angiography was performed using a prototype ultra-high-resolution CT system for clinical use (Toshiba Medical Systems Corporation, Otawara, Japan). This prototype scanner was not commercially available at that time, but it had obtained approval under the Japanese Pharmaceutical and Medical Device Act (Number: 227ADBZX00062000). The ultra-high-resolution CT scanner has 128 detector rows with a 0.25-mm detector row width, supporting image reconstruction with a 1024 × 1024 matrix.
The scanning parameters were as follows: 120 kV, 400 mA, beam collimation of 0.25 mm × 128, beam pitch factor of 0.625, rotation speed of 0.5 or 0.75 s, and scanning field of view (FOV) of 350 mm. Scanning extended from the level of the 7th thoracic vertebra to the level of the 2nd lumbar vertebra.
Images were reconstructed with 0.25-mm slice thickness, 1024 × 1024 matrix, 200-mm display FOV, and kernel FC 13 using an iterative reconstruction algorithm (Adaptive Iterative Dose Reduction 3D [AIDR 3D]; Toshiba) at the standard setting (Fig. 1a). Images were also reconstructed with 0.5-mm slice thickness, 512 × 512 matrix, 200-mm display FOV, and kernel FC 13 using AIDR 3D at the standard setting for comparison with the 0.25-mm slice images (Fig. 1b).

Comparison of a 0.25-mm slice image and a 0.5-mm slice image. Curved planar reformatted images show the artery of Adamkiewicz (arrow) and full continuity between the anterior spinal artery and the aorta through the intervertebral foramen (arrowhead). Note the sharpness of the margins of the vessels in the 0.25-mm slice image. a 0.25-mm slice image. b 0.5-mm slice image
The imaging method for contrast-enhanced CT has been described in previous reports [8, 9]. A total of 2.0 mL/kg body weight of high-osmolarity iodinated contrast medium (iopamidol 370; Bayer, Osaka, Japan) was injected at a rate of 3.5 mL/s via a 20-gauge intravenous catheter placed in an antecubital vein using a double-head power injector. The bolus-tracking method was used to determine the image acquisition timing. A 1-cm-diameter circular region of interest (ROI) was set in the descending aorta at the level of the 7th thoracic vertebra. When the attenuation reached 250 Hounsfield units (HU), scanning was automatically started in the craniocaudal direction. Scanning was performed during a single breath-hold.
All CT data were transferred to a commercially available workstation (Ziostation; Ziosoft, Tokyo, Japan) which is able to process 1024 × 1024 matrix images to generate multiplanar reformation (MPR) images and curved planar reformation (CPR) images. The slice thickness and slice interval of the MPR and CPR images were 0.25 mm for reconstruction of the 0.25-mm slice images and 0.5 mm for reconstruction of the 0.5-mm slice images.
Objective evaluation
Objective image evaluation was performed using the 0.25-mm slice image datasets and the 0.5-mm slice image datasets. For each of these image datasets, the signal-to-noise ratio (SNR) of the aorta and the contrast-to-noise ratio (CNR) between the anterior spinal artery and spinal cord were evaluated according to the method described by Nishida et al. [13]. Both the mean CT number (HU) and standard deviation (SD) for the aorta and spinal cord were measured using circular ROIs (2 and 1 cm in diameter, respectively) at the same position in the axial images. The CT number of the aorta was derived by calculating the mean value in three ROIs placed at the level of the diaphragm, 3 cm above the diaphragm, and 3 cm below the diaphragm. The CT number of the spinal cord was measured as the mean value in three ROIs placed at the levels of the 8th, 9th, and 10th thoracic vertebral bodies. The artery of Adamkiewicz itself was too small to permit measurement of the CT number. Instead, the degree of enhancement was measured by segmenting the anterior spinal artery at 3 cm in a sagittal MPR image [13]. This measurement was performed three times, and the mean value was calculated.
The SNR and the CNR were calculated using the following formulas: SNR = mean CT number of the aorta/SD of the aorta, and CNR = (mean CT number of the anterior spinal artery − mean CT number of the spinal cord)/SD of the spinal cord.
Subjective evaluation
The two image datasets were evaluated by two cardiovascular radiologists (KY and RT) with more than 20 years of experience. They evaluated the images according to the degree of visualization of the artery of Adamkiewicz using the four-point scale proposed by Takagi et al. [11] and Bley et al. [14] with some modifications as follows: 1 point (poor) = the artery of Adamkiewicz is not visualized, 2 points (fair) = the artery of Adamkiewicz is partially visualized, but vascular continuity to the extradural segment is not recognized, 3 points (good) = the artery of Adamkiewicz is clearly visualized, but vascular continuity is partially obscured at the intervertebral foramen, and 4 points (excellent) = the artery of Adamkiewicz is clearly visualized and full vascular continuity through the intervertebral foramen is also recognized. Representative patients are shown in Fig. 2. A score of 3 or 4 points was considered to indicate diagnostic image quality, and a score of 1 or 2 points was considered to indicate nondiagnostic image quality. The side and level of the segmental arteries supplying the artery of Adamkiewicz were also recorded. Any discrepancies in the evaluation results were resolved by mutual consensus.

Representative images (curved planar reformatted images with a 0.5-mm slice thickness) illustrating the four-point scale used to evaluate the degree of visualization of the artery of Adamkiewicz. a Score of 1 point (poor): the artery of Adamkiewicz is not depicted. b Score of 2 points (fair): the hairpin turn of the artery of Adamkiewicz is visualized (arrow). However, the caudal side of the artery of Adamkiewicz is unclear and continuity with the extradural segment cannot be recognized (black arrowheads). c Score of 3 points (good): the hairpin turn of the artery of Adamkiewicz is clearly identified (arrow). However, vascular continuity from the aorta to the anterior spinal artery is partially obscured by the bony structures at the intervertebral foramen (black arrowhead). d Score of 4 points (excellent): the hairpin turn of the artery of Adamkiewicz is clearly depicted (arrow) and continuity of the vessel is clearly visualized through the intervertebral foramen to the extradural segment (white arrowheads)
Statistical analysis
All data were expressed as mean ± standard deviation (SD). The differences in SNR and CNR were compared using the paired t test. The mean values for the degree of visualization of the artery of Adamkiewicz for 0.25- and 0.5-mm slices were also compared using the paired t test. The frequencies of diagnostic versus nondiagnostic image quality were compared using McNemar’s test. Interobserver agreement for the visualization scores of the artery of Adamkiewicz between the two independent reviewers was assessed using Cohen’s kappa test. A value of p < 0.05 was considered to be statistically significant. Analysis was performed using PASW Statistics 21 (SPSS Inc.).
Results
The CT examinations were performed successfully in all 24 patients. The body mass index of the patients was 24.7 ± 2.6 kg/m2. The radiation exposure expressed as the dose-length product (DLP) was 1113.0 ± 211.7 mGy cm.
Objective evaluation results
The artery of Adamkiewicz was not depicted in 1 patient in both the 0.25-mm slice images and 0.5-mm slice images. We did not exclude this patient from the subjective image analysis, because we could measure the degree of enhancement of the anterior spinal artery.
No significant difference in the SNR of the aorta was observed between 0.25-mm slice images (12.7 ± 2.7) and 0.5-mm slice images (13.8 ± 3.0) (p = 0.20). In addition, no significant difference in the CNR of the anterior spinal artery was observed between 0.25-mm slice images (2.3 ± 0.9) and 0.5-mm slice images (2.2 ± 0.9) (p = 0.83).
Subjective evaluation results
The results for the degree of visualization in all patients are summarized in Table 2. The mean value of the degree of visualization for 0.5-mm slice images was 3.13 ± 0.99 (Table 3). The images obtained in a total of 8 patients (33.3%) were judged to be nondiagnostic. The interobserver kappa score was 0.56 (moderate agreement).
The mean value of the degree of visualization for 0.25-mm slice images was 3.58 ± 0.78, which was significantly higher than for 0.5-mm slice images (p = 0.01). The images obtained in only 2 patients (8.3%) were judged to be nondiagnostic, which was significantly lower than for 0.5-mm slice images (p = 0.03). The interobserver kappa score was 0.76 (good agreement).
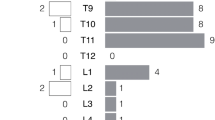
The branching levels and sides of the segmental arteries from which the artery of Adamkiewicz originated were as follows: the left 9th intercostal artery in 5 patients, the left 10th intercostal artery in 4 patients, the left 11th intercostal artery in 3 patients, the left subcostal artery in 1 patient, the right 8th intercostal artery in 3 patients, the right 9th intercostal artery in 3 patients, the right 10th intercostal artery in 2 patients, the right 11th intercostal artery in 1 patient, and the right subcostal artery in 1 patient. The origin could not be identified in 1 patient, because the artery of Adamkiewicz was not visualized. There were 2 patients with duplication of the artery of Adamkiewicz, and the larger artery was selected as the artery of Adamkiewicz in these patients. Collateral arteries due to occlusion of the segmental artery were depicted in 5 patients (21%). We thought that the sources of these collateral pathways were the muscular branch of the intercostal artery in 3 patients and the thoracodorsal artery in 2 patients.
Discussion
It has been reported that obtaining a clear understanding of the artery of Adamkiewicz is useful for reducing the risk of SCI following descending thoracic or thoracoabdominal aortic repair [4, 5]. Recently, a multicenter prospective study involving 2435 patients demonstrated that preoperative identification of the artery of Adamkiewicz with adequate reconstruction or preservation is a useful adjunct to ensure spinal cord protection [6].
Multi-detector row CT is able to depict the artery of Adamkiewicz. The detection rates for the morphologic hairpin turn configuration of the artery of Adamkiewicz have been reported to be in the range from 80 to 90% for 4-detector row CT, 16-detector row CT, and 64-detector row CT with a slice thickness of 0.5 to 2 mm [7,8,9,10,11].
However, previous studies have strongly recommended that the entire course of the artery of Adamkiewicz should be identified by demonstrating continuity from the anterior spinal artery to the aorta via the artery of Adamkiewicz, rather than relying only on demonstration of the characteristic hairpin turn configuration [8,9,10]. This is because the anterior radiculomedullary vein shows a hairpin turn configuration which is similar to that of the artery of Adamkiewicz. When CT is used in the clinical setting, it has been reported that discrimination between the artery of Adamkiewicz and the anterior radiculomedullary vein on the basis of morphology can be very difficult [9]. However, the misidentification of these two vessels may lead to catastrophic results in aortic aneurysm surgery. It is therefore strongly recommended that the artery of Adamkiewicz should be identified by demonstrating vascular continuity from the anterior spinal artery to the aorta via the artery of Adamkiewicz.
The visualization of full vascular continuity from the anterior spinal artery to the aorta via the artery of Adamkiewicz remains a challenge with current CT systems. The demonstration rate for vascular continuity has been reported to be in the range from 29 to 50% for 4-detector row CT with a 2- or 1-mm slice thickness [7, 8] and in the range from 25 to 60% for 16-detector row CT or 64-detector row CT with a 0.5-mm slice thickness [9,10,11]. The difficulty in demonstrating continuity along the entire course of the artery of Adamkiewicz can be attributed not only to the small diameter of the artery but also to the fact that it runs in close proximity to the osseous structures of the intervertebral foramen [9].
In the present report, we have described our initial experience with a novel ultra-high-resolution prototype CT scanner with a 0.25-mm detector row width, with the expectation of improved visualization of smaller structures due to the increased spatial resolution. We investigated the feasibility of visualizing the artery of Adamkiewicz using 0.25-mm slice images as compared to “conventional” images reconstructed with a 0.5-mm slice thickness. A modest but significant increase in the mean value of the degree of visualization was observed, from 3.13 ± 0.99 to 3.58 ± 0.78 (p = 0.01). The percentage of images of diagnostic image quality (grade 3 or 4) for 0.25-mm slice images was 91.6%, which was significantly higher than for reconstruction with a 0.5-mm slice thickness (67.7%) (p = 0.03). Furthermore, the results of this study showed that full vascular continuity between the anterior spinal artery and the aorta (grade 4) could be depicted in 70.8% of patients with a 0.25-mm slice thickness. On the other hand, the depiction rate was only 50.0% for a 0.5-mm slice thickness. Similar results (in the range from 25 to 50%) have been reported by Utsunomiya et al. and Takagi et al. using 0.5-mm slice images acquired using a conventional 64-detector row CT scanner [10, 11].
In most patients, vascular continuity was obscured near the intervertebral foramen. The osseous structures around the intervertebral foramen show high attenuation and may cause blooming artifacts which interfere with visualization of the arteries. The improved spatial resolution of 0.25-mm slice images may make it easier to distinguish small arteries from bony structures, thus permitting successful visualization of full vascular continuity (Fig. 3).

A 69-year-old woman with a thoracic aortic aneurysm. Curved planar reformatted images show the artery of Adamkiewicz. a 0.5-mm slice image. Vascular continuity is not clearly recognized in the intradural segment (arrow) as well as the extradural segment at the intervertebral foramen (arrowhead). b 0.25-mm slice image. Vascular continuity is recognized in both the intradural segment (arrow) and the extradural segment at the intervertebral foramen (arrowhead)
In the present study, the images were reconstructed using an iterative reconstruction method (AIDR 3D) rather than filtered back projection (FBP). It is known that iterative reconstruction can provide improved image quality by reducing image noise. Therefore, the use of an iterative reconstruction algorithm may have also contributed to the observed improvement in the degree of visualization of the artery of Adamkiewicz. However, Nishida et al. reported that application of an adaptive statistical iterative reconstruction algorithm did not result in a significant improvement in the visualization score of the artery of Adamkiewicz in comparison with FBP at a slice thickness of 0.625 mm [13]. Machida et al. also reported similar results [15]. In our study, no significant differences in the SNR of the aorta or the CNR of the anterior spinal artery were observed between 0.25-mm slice images and 0.5-mm slice images. Based on these findings, we think it is reasonable to compare our findings to previous studies, which mostly employed FBP reconstruction [7,8,9,10,11].
On the other hand, more favorable results have been described using model-based iterative reconstruction algorithms, which may facilitate delineation of the artery of Adamkiewicz [13, 15]. At present, model-based iterative reconstruction is not yet available for the ultra-high-resolution CT scanner. We anticipate, however, that the combination of an increased spatial resolution (0.25-mm slice thickness) and model-based iterative reconstruction may be particularly powerful for depicting the vascular continuity of the artery of Adamkiewicz and could potentially further improve overall image quality and the degree of visualization. Bone-subtracted CT angiography has been described as another potentially useful approach which may allow us to more clearly distinguish between osseous structures and enhanced vessels in the intervertebral foramen [16]. However, since this protocol requires two separate scans, the reported radiation exposure as reflected in the mean DLP was 5238.1 ± 1220.8 mGy cm, which is much higher than that in our study (1113.0 ± 211.7 mGy cm).
The present study has several limitations. The first major limitation is the small patient population. Although our results have shown the feasibility of using ultra-high-resolution CT angiography to visualize the artery of Adamkiewicz, studies with larger patient populations are needed to confirm our findings. Second, conventional angiography for verification of the location of the artery of Adamkiewicz was not performed. However, selective intercostal angiography is difficult to perform and is associated with a risk of major procedure-related complications such as SCI, renal failure, and stroke in patients with aortic aneurysms [17]. Conventional angiography was therefore not performed in order to avoid exposing the patients to unnecessary risk. Besides, we should recognize that our CT protocol, in which 2.0 mL/kg body weight of high-osmolarity iodinated contrast medium is injected, has the risk of renal failure. Third, we did not scan patients twice using both the novel ultra-high-resolution CT scanner and the conventional CT scanner with standard spatial resolution. Instead, we reconstructed the 0.5-mm slice images from the 0.25-mm slice images. The degree to which these reconstructed 0.5-mm slice images are representative of directly collimated 0.5-mm slice images was not evaluated. The fact that the detection rate obtained using a 0.5-mm slice thickness in the present study is comparable to that reported in previous studies using 0.5-mm collimated scanning with conventional 64-detector row CT [9,10,11] supports this methodological decision, although more detailed validation, such as by means of a phantom study, would be desirable.
Conclusion
The results of this initial feasibility study show that ultra-high-resolution CT using a 0.25-mm slice thickness significantly improves visualization of the artery of Adamkiewicz, including the depiction of vascular continuity between the anterior spinal artery and the aorta via the artery of Adamkiewicz, as compared to a 0.5-mm slice thickness in patients with aortic aneurysms.
References
Coselli JS, Bozinovski J, LeMaire SA (2007) Open surgical repair of 2286 thoracoabdominal aortic aneurysms. Ann Thorac Surg 83:S862–S864
Schepens MA, Heijmen RH, Ranschaert W, Sonker U, Morshuis WJ (2009) Thoracoabdominal aortic aneurysm repair: results of conventional open surgery. Eur J Vasc Endovasc Surg 37:640–645
Gialdini G, Parikh NS, Chatterjee A et al (2017) Rates of spinal cord infarction after repair of aortic aneurysm or dissection. Stroke 48:2073–2077
Kawaharada N, Morishita K, Fukada J et al (2002) Thoracoabdominal or descending aortic aneurysm repair after demonstration of the Adamkiewicz artery by magnetic resonance angiography. Eur J Cardiothorac Surg 21:970–974
Ogino H, Sasaki H, Minatoya K, Matsuda H, Yamada N, Kitamura S (2006) Combined use of Adamkiewicz artery demonstration and motor-evoked potentials in descending and thoracoabdominal repair. Ann Thorac Surg 82:592–596
Tanaka H, Ogino H, Minatoya K et al (2016) The impact of preoperative identification of the Adamkiewicz artery on descending and thoracoabdominal aortic repair. J Thorac Cardiovasc Surg 151:122–128
Takase K, Sawamura Y, Igarashi K et al (2002) Demonstration of the artery of Adamkiewicz at multi-detector row helical CT. Radiology 223:39–45
Yoshioka K, Niinuma H, Ohira A et al (2003) MR angiography and CT angiography of the artery of Adamkiewicz: noninvasive preoperative assessment of thoracoabdominal aortic aneurysm. Radiographics 23:1215–1225
Yoshioka K, Niinuma H, Ehara S, Nakajima T, Nakamura M, Kawazoe K (2006) MR angiography and CT angiography of the artery of Adamkiewicz: state of the art. Radiographics 26(Suppl 1):S63–S73
Utsunomiya D, Yamashita Y, Okumura S, Urata J (2008) Demonstration of the Adamkiewicz artery in patients with descending or thoracoabdominal aortic aneurysm: optimization of contrast medium application for 64-detector-row CT angiography. Eur Radiol 18:2684–2690
Takagi H, Ota H, Natsuaki Y et al (2015) Identifying the Adamkiewicz artery using 3-T time-resolved magnetic resonance angiography: its role in addition to multidetector computed tomography angiography. Jpn J Radiol 33:749–756
Kakinuma R, Moriyama N, Muramatsu Y et al (2015) Ultra-high-resolution computed tomography of the lung: image quality of a prototype scanner. PLoS One 10:e0137165
Nishida J, Kitagawa K, Nagata M, Yamazaki A, Nagasawa N, Sakuma H (2013) Model-based iterative reconstruction for multi-detector row CT assessment of the Adamkiewicz artery. Radiology 270:282–291
Bley TA, Duffek CC, Francois CJ et al (2010) Presurgical localization of the artery of Adamkiewicz with time-resolved 3.0-T MR angiography. Radiology 255:873–881
Machida H, Tanaka I, Fukui R et al (2013) Improved delineation of the anterior spinal artery with model-based iterative reconstruction in CT angiography: a clinical pilot study. AJR Am J Roentgenol 200:442–446
Nishii T, Kono AK, Nishio M et al (2015) Bone-subtracted spinal CT angiography using nonrigid registration for better visualization of arterial feeders in spinal arteriovenous fistulas. AJNR Am J Neuroradiol 36:2400–2406
Kieffer E, Fukui S, Chiras J, Koskas F, Bahnini A, Cormier E (2002) Spinal cord arteriography: a safe adjunct before descending thoracic or thoracoabdominal aortic aneurysmectomy. J Vasc Surg 35:262–268
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for this study.
Conflict of interest
KA, SJ and YS are employees of Toshiba Medical Systems Corporation. KY and RT have a contract to conduct academic research in cooperation with Toshiba Medical Systems Corporation.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Yoshioka, K., Tanaka, R., Takagi, H. et al. Ultra-high-resolution CT angiography of the artery of Adamkiewicz: a feasibility study. Neuroradiology 60, 109–115 (2018). https://doi.org/10.1007/s00234-017-1927-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-017-1927-7