
Abstract
Introduction
Early assessment of the pyramidal tracts is important for intracerebral hemorrhage (ICH) patients in order to decide the optimal treatment or to assess appropriate rehabilitation strategies, and management of patient expectations and goals. The purpose of this study was to systematically review and summarize the current available literature on the value of Fractional Anisotropy (FA) parameter of the diffusion tensor imaging (DTI) in predicting upper extremity (UE) motor recovery after subacute ICH.
Methods
PubMed, EMBASE, MEDLINE, Google Scholar, and Cochrane CENTRAL searches were conducted from 1 January 1950 to 31 March 2016 which were supplemented with relevant articles identified in the references. Pooled estimate using correlation between DTI parameter FA and UE motor recovery was done using comprehensive meta-analysis software.
Results
Out of 97 citations, only eight studies met the criteria for inclusion in the systematic review and six studies were included in the meta-analysis. A random effects model revealed that DTI parameter FA is a significant predictor for UE motor recovery after subacute ICH (correlation coefficient = 0.56; 95 % confidence interval 0.44 to 0.65, P value <0.001). However, moderate heterogeneity was observed between the studies (Tau-squared = 0.28, I-squared = 70.3).
Conclusion
The studies reported so far on correlation between FA parameter of DTI and UE motor recovery in ICH patients are few with small sample sizes. This meta-analysis suggests a strong correlation between DTI parameter FA and UE motor recovery in ICH patients. Further well-designed prospective studies embedded with larger sample size are needed to confirm these findings.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Primary intracerebral hemorrhage (ICH) is the most common type of hemorrhage in adults and often causes severe motor weakness and functional disability [1]. Prediction of the motor prognosis in these patients is important for designing an appropriate rehabilitation program. One of the commonest mechanisms of neuronal injury following an ICH is due to Wallerian degeneration in the corticospinal tract (CST) in the immediate vicinity and remote from the site of the hematoma. This injury results directly from injury to the neuronal structures in white or gray matter. Apart from the mechanical mass effect, inflammation and edema around the periphery of the hematoma takes place in the acute phase [2, 3]. There are other mechanisms mediating injury to the neural structures of the white matter [2, 4]. In the early phase, there is neuronal damage mediated by blood components and the hemoxygenase enzymes that cleave heme. Heme degradation products then diffuse out into the tissues causing cellular toxicity [5, 6].
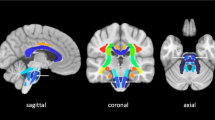
CST is an important white matter tract made up of pyramidal tract, internal capsule, and the cerebral peduncle, and the extent of its damage is correlated with the motor outcome after an acute ICH [7]. Therefore, an evaluation of the CST integrity after ICH may be helpful for motor outcome prediction. However, computed tomography or conventional magnetic resonance imaging (MRI) are based on registering signal from a volume of tissue by repeated rephasing and dephasing of processing protons in the particular volume imaged and has limitations to precisely assess the microstructural damage of the CST. Diffusion tensor imaging (DTI) is one of the noninvasive method which can detect the direction and degree of water molecule diffusion and can be used to delineate the anatomical orientation and integrity of the white matter tracts [8]. Water molecules in most tissues diffuse equally in all directions (isotropic diffusion), but in white matter tracts, the diffusion is along the direction of the tract (anisotropic).
Several indices can be derived from DTI: Fractional anisotropy (FA) is a relative measure which describes the extent of directionality of water diffusion. FA of the entire tract, acquired early after stroke, reflects acute and permanent damage to pyramidal tracts to determine clinical motor deficit and outcome. Findings from recent studies have suggested the predictive value of DTI for motor outcome after ICH [9–16]; however, it is not yet routinely used to make a prognosis, but there have been some interesting recent developments in this area. Therefore, the purpose of this review was to establish the predictive value of DTI for upper extremity (UE) motor recovery in ICH patients.
Materials and methods
Search strategy
PubMed, EMBASE, MEDLINE, Google Scholar, and Cochrane CENTRAL searches were conducted from 1 January 1950 to 31 March 2016. The search terms were “diffusion tensor imaging,” “motor recovery,” and “upper extremity” combined with “Intracerebral hemorrhage.” Manual searches of the reference lists of retrieved articles and pertinent reviews were also conducted. No language restrictions were imposed. Reference list of the included studies was also searched. The studies were selected if they included patients of ICH with UE motor deficit and had DTI done and measurement of clinical recovery on follow-up.
Inclusion criteria
-
1.
Full text published article
-
2.
Observational study that investigated a DTI parameter (FA) measured at baseline and its relationship with a measure of UE recovery measured at a future time point
-
3.
The study population included individuals with UE deficits following ICH
-
4.
Outcomes included UE function/functional improvement or impairment
Exclusion criteria
-
1.
No extractable data was available for independent variables
-
2.
It explored response to treatment with DTI
-
3.
They were case-reports or review articles
-
4.
Included patients who were in the chronic phase (inclusion of patients > 1 month of ICH onset)
Data extraction
According to the Preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines [17], two investigators PK and AKY independently searched and evaluated the literature for inclusion of studies based on the titles and abstracts/full articles. We extracted the following data from eligible studies: surname of first author, year of publication, number of patients, mean age, sex ratio, lesion location, hemisphere affected, timing of DTI, UE scale used, DTI parameters, location of FA, and duration of follow-up. The imaging parameters such as acquisition matrix, echo time, repetition time, DTI direction, field of view, b-value, MRI system used, number of slices, slice thickness, imaging software, region of interest (ROI) area, hematoma volume, and FA ratio was also extracted. All discrepancies were resolved after rechecking the source papers and further discussion among all the authors.
Quality assessment
To evaluate the methodological quality of included studies, checklist provided by Tooth et al. [18] was used and focused on the basic elements of quality assessment. The quality of each study was assessed according to whether the information was provided regarding 30 items present in the list. The methodological assessment was done independently by two authors (PK and AKY), and the disagreements were resolved by discussion among all the authors. Assessments were expressed in terms of “Yes” if description was available and “No” if the description was not available. The scores of quality assessment of all characteristics were out of 30, Yes was given score “1” and No was given score “0.” This quality assessment method records the numbers, and reasons for, eligibility, consent, participation in each wave, and attrition. These main elements were chosen because they provide information at a glance on probable selection-driven threats to internal and external validity.
Statistical analysis
The correlation between DTI parameter FA and UE motor recovery measure was done using trial version of Comprehensive Meta-analysis Software (https://www.meta-analysis.com). For one study, Koyoma et al. [11] correlation coefficient was calculated from individual patient data provided in the paper. The data for ICH patients with lesion location in cerebral peduncle was used for this calculation. There was no duplication of patient’s data while performing the analysis. Heterogeneity was examined using Higgins I-squared and Tau-squared test [19]. Summary of correlation coefficient was determined using random effects model.
Results
Identification of relevant studies
A total of 97 published articles were identified using the prespecified search strategy. Figure 1 represents a flow chart of retrieved and excluded studies with their reasons for exclusion. Out of 97 retrieved articles, 73 were irrelevant studies as their objective were (1) not to predict upper limb motor recovery, (2) not associated with ICH (3) were conducted in animal models, and (4) were based on rehabilitation strategies, nine studies were in duplicate records, five studies were excluded as they were not about the prediction of UE motor recovery, and two studies were excluded as they were review article. Finally, total eight studies were included for the systematic review and six studies were included for the meta-analysis. The general characteristics of the included studies, relative methodological details, and imaging parameters are presented in Tables 1 and 2.

Flow diagram of the selection of studies and specific reasons for exclusion from the present meta-analysis
Characteristics of studies
Eight studies included a total of 229 patients with subacute ICH with the sample size ranged from 15 to 48 participants. The DTI measurement parameters reported were FA, mean diffusitivity (MD), and apparent diffusion coefficient (ADC). Discrepancies emerged in terms of lesion location DTI evaluation in the included studies. The studies also used a wide range of scales to measure upper limb motor outcome measures such as modified National Institutes of Health Stroke Scale (mNIHSS) (1/8), Medical Research Council (MRC) (2/8), Manual Muscle Test (MMT) (1/8), Motricity Index (MI) (1/8), and Brunstrom Scale (BRS) (1/8). We have excluded two studies from the meta-analysis—one studies by Tao et al. (2014) as they used modified Rankin Scale (mRS) which were not specific for upper limb motor outcome and another study by Kusano et al. (2009)—they did not provide the data for the correlation for upper limb motor outcome. The follow-up period ranged from 1 to 18 months (Table 1).
Methodological quality
Table 3 represents the quality assessment results for the included studies. There was 90 % agreement between the two authors (PK and AKY). All studies described the study population, the eligibility criteria, number of patients in the beginning, and absolute effect sizes. All the eight included studies described the method of data collection and type of analysis done. Only one study reported reasons for loss to follow-up. However, loss to follow-up and confounders were not taken into account in any of the studies. No study assessed the impact of biases on the analysis.
Meta-analysis
The results of the meta-analysis are presented in Fig. 2 using random effects model. Out of eight studies, six studies provided data to allow determination of summary of correlation coefficient. FA was presented either as ratio of affected vs. unaffected side or mean. A random effects model revealed that DTI parameter FA is a significant predictor for UE motor recovery after subacute ICH (correlation coefficient = 0.56; 95 % confidence interval 0.44 to 0.65, P value <0.001). However, moderate heterogeneity was observed between the studies (Tau-squared = 0.28, I-squared = 70.3).

Forest plot: correlation coefficient for the prediction of upper extremity motor recovery after subacute ICH
Discussion
In this study, we reviewed relevant studies on prediction of UE motor recovery outcome in subacute ICH patients to determine whether the integrity of the CST, as determined by DTI parameter FA obtained during the early stage of ICH, can positively predict the UE motor recovery. The present meta-analysis showed a significant positive correlation between DTI parameter FA and UE motor recovery in ICH patients. A method to reliably predict UE recovery would help to optimize rehabilitation, to inform patients about prognosis and to design clinical trials to identify appropriate interventions. DTI is now reaching a point when the resolution and ability to track fibers optimally are very reliable. Secondary injuries to the brain tissue at the periphery of the hematoma after ICH are mediated by both the mass effect of the new hemorrhage and the toxicity that is associated with hematoma degradation and organization and the consequent release of inflammatory and free radical mediators. Iron has been shown to be responsible for cerebral toxicity [5].
To begin with, there is a huge potential for demonstrating DTI as a reliable imaging surrogate of impending neuronal toxicity in patients with hemorrhagic stroke. The next step would be to demonstrate reliable correlation of DTI with functional outcome to be able to stratify risk in patients suffering from ICH. The use of DTI FA measures, in combination with other quantitative imaging modalities (e.g. spectroscopy, perfusion), may help to improve the specificity of tissue pathology. The advancement of tools for tractography, image segmentation and co-registration (between subject normalization), and anatomical templates will help to improve anatomic specificity of DTI characterization in both clinical and research settings. For patients in whom transcranial magnetic stimulation fails to elicit responses in the affected UE, DTI provides a useful measure of CST integrity. Those patients with FA asymmetry of <0.25 have greater functional potential and are more likely to lateralize cortical activity toward the ipsilesional motor cortex during affected UE use. This ipsilesional lateralization may be enhanced by interventions designed to increase the excitability and plasticity of the ipsilesional cortex. Priming the ipsilesional cortex, as an adjuvant therapy, may improve functional outcomes in this group [20, 21]. Patients without motor evoked potential responses to transcranial magnetic stimulation in the affected UE, and FA asymmetry of >0.25, are likely to have low functional potential and poor recovery of UE function [22]. The degree of impairment in FA during the early stages of ICH appears to have the potential to predict motor outcome [7, 23–25].
The studies included in the meta-analysis reported heterogeneous data, which could be a major limitation to our results. The assessment parameters differ for included study in the analysis, e.g., UE assessment scales, use of different DTI softwares, MRI system, and different location of FA. The region of interest selection technique is operator-dependent which might have also affected the results. DTI may underestimate the fiber tracts than electrophysiological test. DTI is a powerful anatomic imaging tool that can demonstrate the gross fiber architecture, but not the functional or synaptic connections. Therefore, major fiber bundles such as the CST can be the real fiber pathways on DTI, relaying fibers cannot be depicted with DTI. Although FA is likely to be adequate for many applications and appears to be quite sensitive to a broad spectrum of pathological conditions, the full tensor shape cannot be simply described using a single scalar measure. As it does not describe the full tensor shape or distribution. This is because different Eigen value combinations can generate the same values of FA. However, the tensor shape can be described completely using a combination of spherical, linear, and planar shape measures. In particular, FA is highly sensitive to microstructural changes, but not very specific to the type of changes (e.g., radial or axial). Moreover, there are various analysis techniques such as streamline and probabilistic techniques. Streamline method provides a single estimate of a virtual fiber track without incorporating the uncertainty introduced by noise, whereas probabilistic methods attempt to address this limitation by providing a confidence measure. Streamline method generates a unique virtual fiber track, whereas probabilistic method produces an arbitrary number of virtual fiber tracks that are reconstructed [26].
Therefore, combined studies using other brain mapping techniques, such as transcranial magnetic stimulation or functional magnetic resonance imaging, would be necessary to compensate for the limitations of DTI [27]. The advantages of each of the methods for evaluation of a neural tract allow more accurate estimation when they are employed concomitantly, because combination can compensate for the limitations of a certain evaluation method and more accurate information can be obtained. The most ideal evaluation method for assessment of the CST would be capable of (1) obtaining information about the integrity and course of the CST and quantification of the CST at the subcortical level using DTI with diffusion tensor tractography, (2) obtaining information on the origin of the CST at the cortical level using functional magnetic resonance imaging, and (3) obtaining information on the quantification and characteristics of the CST using motor evoked potential determined by transcranial magnetic stimulation. However, further improvements in the technique and in post processing analysis are needed to increase the widespread utility of DTI in both research and clinical applications.
Conclusion
In the acute and subacute phase, there is an unexplained variability in the extent to which patients recover after ICH. DTI has emerged as a promising tool for CST integrity mapping to predict UE motor outcome. The studies reported so far on correlation between FA parameter of DTI and UE motor recovery in ICH patients are few with small sample sizes. This meta-analysis suggests a strong correlation between DTI parameter FA and UE motor recovery in ICH patients. Further well-designed prospective studies embedded with larger sample size are needed to confirm these findings.
References
Grysiewicz RA, Thomas K, Pandey DK (2008) Epidemiology of ischemic and hemorrhagic stroke: incidence, prevalence, mortality, and risk factors. Neurol Clin 26(871–95):vii
Zhou Y, Wang Y, Wang J, Anne Stetler R, Yang Q-W (2014) Inflammation in intracerebral hemorrhage: from mechanisms to clinical translation. Prog Neurobiol 115:25–44
Hatakeyama T, Okauchi M, Hua Y, Keep RF, Xi G (2013) Deferoxamine reduces neuronal death and hematoma lysis after intracerebral hemorrhage in aged rats. Translat Stroke Res 4:546–53
Gu Y, Hua Y, Keep RF, Morgenstern LB, Xi G (2009) Deferoxamine reduces intracerebral hematoma-induced iron accumulation and neuronal death in piglets. Stroke J Cereb Circ 40:2241–3
Xi G, Keep RF, Hoff JT (2006) Mechanisms of brain injury after intracerebral haemorrhage. Lancet Neurol 5:53–63
Zhao X, Sun G, Zhang H, Ting S-M, Song S, Gonzales N et al (2014) Polymorphonuclear neutrophil in brain parenchyma after experimental intracerebral hemorrhage. Translat Stroke Res 5:554–61
Cho S-H, Kim SH, Choi BY, Cho SH, Kang JH, Lee C-H et al (2007) Motor outcome according to diffusion tensor tractography findings in the early stage of intracerebral hemorrhage. Neurosci Lett 421:142–6
Pierpaoli C, Jezzard P, Basser PJ, Barnett A, Di Chiro G (1996) Diffusion tensor MR imaging of the human brain. Radiology 201:637–48
Cheng C-Y, Hsu C-Y, Huang Y-C, Tsai Y-H, Hsu H-T, Yang W-H et al (2015) Motor outcome of deep intracerebral haemorrhage in diffusion tensor imaging: comparison of data from different locations along the corticospinal tract. Neurol Res 37:774–81
Tao W-D, Wang J, Schlaug G, Liu M, Selim MH (2014) A comparative study of fractional anisotropy measures and ICH score in predicting functional outcomes after intracerebral hemorrhage. Neurocrit Care 21:417–25
Koyama T, Tsuji M, Nishimura H, Miyake H, Ohmura T, Domen K (2013) Diffusion tensor imaging for intracerebral hemorrhage outcome prediction: comparison using data from the corona radiata/internal capsule and the cerebral peduncle. J Stroke Cerebrovasc Dis Off J Nat Stroke Assoc 22:72–9
Koyama T, Tsuji M, Miyake H, Ohmura T, Domen K (2012) Motor outcome for patients with acute intracerebral hemorrhage predicted using diffusion tensor imaging: an application of ordinal logistic modeling. J Stroke Cerebrovasc Dis Off J Nat Stroke Assoc 21:704–11
Koyama T, Marumoto K, Uchiyama Y, Miyake H, Domen K (2015) Outcome assessment of hemiparesis due to intracerebral hemorrhage using diffusion tensor fractional anisotropy. J Stroke Cerebrovasc Dis Off J Nat Stroke Assoc 24:881–9
Wang D-M, Li J, Liu J-R, Hu H-Y (2012) Diffusion tensor imaging predicts long-term motor functional outcome in patients with acute supratentorial intracranial hemorrhage. Cerebrovasc Dis Basel Switz 34:199–205
Kusano Y, Seguchi T, Horiuchi T, Kakizawa Y, Kobayashi T, Tanaka Y et al (2009) Prediction of functional outcome in acute cerebral hemorrhage using diffusion tensor imaging at 3T: a prospective study. AJNR Am J Neuroradiol 30:1561–5
Yoshioka H, Horikoshi T, Aoki S, Hori M, Ishigame K, Uchida M et al (2008) Diffusion tensor tractography predicts motor functional outcome in patients with spontaneous intracerebral hemorrhage. Neurosurgery 62:97–103, discussion 103
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4:1
Tooth L, Ware R, Bain C, Purdie DM, Dobson A (2005) Quality of reporting of observational longitudinal research. Am J Epidemiol 161:280–8
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–60
Stefan K, Kunesch E, Cohen LG, Benecke R, Classen J (2000) Induction of plasticity in the human motor cortex by paired associative stimulation. Brain J Neurol 123:572–84
Smith AL, Staines WR (2006) Cortical adaptations and motor performance improvements associated with short-term bimanual training. Brain Res 1071:165–74
Stinear CM, Barber PA, Smale PR, Coxon JP, Fleming MK, Byblow WD (2007) Functional potential in chronic stroke patients depends on corticospinal tract integrity. Brain J Neurol 130:170–80
Kwak SY, Yeo SS, Choi BY, Chang CH, Jang SH (2010) Corticospinal tract change in the unaffected hemisphere at the early stage of intracerebral hemorrhage: a diffusion tensor tractography study. Eur Neurol 63:149–53
Cho S-H, Kim DG, Kim D-S, Kim Y-H, Lee C-H, Jang SH (2007) Motor outcome according to the integrity of the corticospinal tract determined by diffusion tensor tractography in the early stage of corona radiata infarct. Neurosci Lett 426:123–7
Jang SH, Bai D, Son SM, Lee J, Kim D-S, Sakong J et al (2008) Motor outcome prediction using diffusion tensor tractography in pontine infarct. Ann Neurol 64:460–5
Alexander AL, Lee JE, Lazar M, Field AS (2007) Diffusion tensor imaging of the brain. Neurother J Am Soc Exp Neurother 4:316–29
Stinear CM, Byblow WD, Ward SH (2014) An update on predicting motor recovery after stroke. Ann Phys Rehabil Med 57:489–98
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
We declare that this manuscript does not contain clinical studies or patient data.
Conflict of Interest
We declare that we have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kumar, P., Yadav, A.K., Misra, S. et al. Prediction of upper extremity motor recovery after subacute intracerebral hemorrhage through diffusion tensor imaging: a systematic review and meta-analysis. Neuroradiology 58, 1043–1050 (2016). https://doi.org/10.1007/s00234-016-1718-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-016-1718-6