
Abstract
Purpose
The elderly often use several drugs on a regular basis and are especially at risk for drug-related harm from side effects and interactions. The aim of this study was to explore the overall prevalence of and predictors for potentially inappropriate medication use among Norwegian elderly outpatients.
Methods
A pharmaco-epidemiological retrospective cross-sectional survey was undertaken based on data from the Norwegian Prescription Database. Prescriptions from all doctors in Norway, dispensed by pharmacies to home-dwelling elderly ≥70 years in 2008, were included for a total of 11,491,065 prescriptions from 24,540 prescribers to 445,900 individuals (88.3% of the Norwegian population in this age group, 58.9% females). We applied a list of criteria for pharmacological inappropriateness for elderly people (the NORGEP criteria) to determine the prevalence of potentially inappropriate medications (PIMs) and applied a multiple logistic regression model to identify predictors.
Results
According to our criteria, 34.8% of the study population (28.5% of the men, 39.3% of the women) was exposed to at least one PIM. Of these, 59.9% represented psychoactive substances. The odds of receiving potentially harmful prescriptions increased with the number of prescribers (OR 3.52, 99% CI 3.44–3.60 for those with ≥5 compared to those with 1 or 2 prescribers). Twenty percent were prescribed more than 10 medications; among these two-thirds had at least one PIM. Adjusted for differences in age distribution and the number of prescribers involved, women were more frequently exposed to PIMs than men, with an odds ratio of 1.60 (99% CI 1.58–1.64).
Conclusions
About one-third of the elderly Norwegian population is exposed to potentially inappropriate medications, and elderly females are at particular risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Modern pharmacotherapy can be a double-edged sword. While many have their lives prolonged and enjoy a better quality of life, there is always a risk of adverse drug reactions (ADRs). At present there is reason to characterize ADRs as a threat to public health: an estimated 5,000 hospital beds in England are at any time occupied by patients admitted for ADRs [1]. A Swedish study with data from 2001 estimated that 3% of deaths in the general population were caused by ADRs [2]. In a meta-analysis from 1998, Lazarou et al. found the incidence of fatal ADRs in the USA to be 0.32%, making ADRs the fourth to sixth most common cause of death [3], and in a study from a Norwegian department of internal medicine, every fifth death was considered to be at least partly caused by ADRs, with the oldest patients at particular risk [4].
The risk of ADRs increases with the number of drugs taken [5]. Older people have a higher prevalence of comorbidities, and only a few decades after the first pharmaceutical discoveries many elderly now use a substantial and still increasing number of drugs on a regular basis [6]. In 2008, persons 70 years or older represented 15% of the drug users in Norway but received 35% of the total amount of drugs dispensed on prescription [7]. The question is whether this substantial number of medications represents a new risk factor for disease in the elderly. There is some recent evidence that controlled medication discontinuation can improve the subjective quality of life in the elderly [8, 9].
Several drugs are especially known to cause ADRs in the elderly, due to their mechanism of action or due to potentially dangerous interactions [10]. In old age physiological changes such as reduced kidney function, altered distribution volumes, altered permeability of the blood-brain barrier, and comorbidities change the way the body handles medication. Thus efficacy may be altered and the elderly may be particularly prone to harm from ADRs [11], for instance from constipation, blurred vision, urinary retention, reduced salivation, and reduced cognition from anticholinergics [12–15], or from the increased risk of kidney failure, congestive heart failure, or gastrointestinal bleeding from NSAIDs [16–18]. Metabolism half-life of several agents is prolonged in the elderly, increasing the risk of accumulation of benzodiazepines and many other substances [19, 20].
Lists of explicit criteria have been developed as tools to investigate potentially inappropriate medications (PIMs) in the elderly [21, 22], among them the Beers’ criteria in the U.S. [23–25] and the STOPP/START criteria in Europe [26]. Studies from different countries applying these criteria have found proportions of 14–42% of home-dwelling elderly receiving PIMs [27–35]. Potentially inappropriate medication use in the elderly is shown to increase the risk of serious avoidable ADRs when measured by the STOPP criteria [36] and appears to have a negative impact on patient outcomes such as self-assessed health status [37] and health care costs [38].
A Norwegian list of criteria was recently developed for general practice. The resulting NORGEP criteria (shown in Table 3) form a list of explicit criteria for pharmacological inappropriateness [39], consisting of 36 statements, including 21 regarding single drugs and 15 regarding drug-drug combinations. The list is partly based on the American Beers’ criteria, adapted for the Norwegian pharmaceutical market, and was derived through a three-round Delphi consensus process involving 48 specialists in geriatrics, clinical pharmacology, and family medicine. The objective of the present study was to describe the prevalence of and explore predictors for potentially inappropriate medication use in elderly home-dwelling in a modern society, applying the NORGEP criteria to prescription data from the elderly Norwegian population.
Methods
Study design and sample
We conducted a pharmaco-epidemiological retrospective cross-sectional survey based on data from the Norwegian Prescription Database (NorPD), a national database established in 2004 holding data on all prescription drugs dispensed to outpatients by all Norwegian pharmacies [40]. We received information on all prescriptions made by physicians to home-dwelling elderly ≥70 years in 2008. A cut-off of 70 years was chosen as the home-dwelling 65-year-olds of today more often are in good health. In 2008 the population of elderly ≥70 years in Norway was 504,808 (11% of the total population), and among these were 299,575 females and 205,233 males [41]. The data set consists of a total of 11,491,065 dispensings from 24,540 prescribers (the number slightly exceeds the number of doctors residing in Norway in 2008, due to temporary work by doctors from other countries) to 445,900 identified individuals, equivalent to 88.3% of the total population ≥70 years (Fig. 1). NorPD holds no information on medication dispensed to individuals residing in institutions (e.g., hospitals and nursing homes) or medication sold over the counter. Prescriptions from dentists and veterinarians were not included in the data set. Prescriptions to patients not identified by their unique Social Security Number were excluded. Out of the recorded dispensings, 99.49% were included in our analyses.

Data were pseudonymized and include patients’ gender and year of birth. For the prescribed substance, data also include name, date, and information on the amount of medication prescribed, including number of defined daily doses (DDD) [42]. All substances were classified according to the WHO Anatomical Therapeutical and Chemical (ATC) Classification System [42]. No clinical data were available. No geographic data were provided (rural, urban) as this could threaten anonymity; Norway has many small communities and knowing the year of birth, gender, and domicile could potentially identify individuals. The study protocol was presented to and the study permitted by the Norwegian Social Sciences Data Services (NSD). Because all data were pseudonymous the study was assessed by the NSD not to need explicit approval by the Regional Committees for Medical and Health Research Ethics.
Data extraction and statistical analysis
As the original files were of a substantial size, we developed systematic methods by use of a Structured Query Language (SQL) server and PASW Statistics 18 (SPSS, Chicago, IL) statistical software to screen for errors in data and software and combined this with manual checks.
A software tool was developed to extract the relevant prescriptions. For each patient, the program aggregated synonymous prescriptions and calculated both the total amount of medication given for each substance and the estimated amount of time the prescriptions covered. For the substances on the NORGEP list, all dispensings of the same drug (ATC code) throughout the year were aggregated and counted as one hit. Thus, several dispensings of the same drug or the same combination of drugs to one person was still counted as one PIM.
For the two single-substance criteria addressing overuse, cut-off was set to include only those who had three or more dispensings, lasting 9+ months of the year, with an amount exceeding 35 mg/day for oxazepam and 8 mg/day for zopiclone throughout this period. This was done to avoid overestimating overuse. These substances can be dispensed in packages of 100 tablets. Two of these large dispensings in less than 3 months without further dispensings during the year was not recorded as overuse.
For the combination criteria, methods to estimate concomitant use were developed. Average dose between dispensings was calculated as DDD/day. For a drug to be categorized as in continuous use, average DDD/day had to be above a preset cut-off set at 80% of the lowest dose in the normal administration form available, or half of this if the drug in question was sold as a pill with a division mark. The drugs on this list are to a large extent drugs taken on a daily basis. The cut-off of 80% was set in order to avoid the exclusion of regular users of low doses with slight compliance errors thus consuming slightly less than prescribed, and those who had received new dispensings at the end of 2007.
One criterion concerns the concomitant prescription of three or more drugs within the groups of centrally acting analgesics, antipsychotics, antidepressants, and/or benzodiazepines. For this criterion to be met, we demanded a minimum of 3 months concomitant use of at least three substances according to the calculations mentioned above. This means there had to be more than one dispensing, or as a minimum one dispensing of the largest number of pills (normally 100) for the drug to be counted as being in regular use in this time period. As our data reflect the date when the drugs were dispensed from the pharmacy and not the date of ingestion, including the drugs that were calculated to last for less than 3 months would increase the risk of wrongly including cases where a person has, for instance, tried out several drugs without actually using more than one at the time. For this criterion, different combinations of drugs at different times through the year for one person were counted as one PIM.
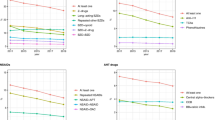
Statistical analysis was performed with PASW Statistics 18. Because of the large sample size, the level of confidence was set to 99%. Median and interquartile range were used to describe sample characteristics of the number of dispensings per person, number of ATC codes per person, and number of prescribers per person, due to the highly skewed distributions of the variables. Binary logistic regression was used to assess relations between inappropriate prescription(s) (yes/no) for a patient, and patient’s gender, age, and the number of doctors involved in the prescribing. The predictors were categorized since their relations to the log odds ratio were nonlinear. Age was categorized into 5-year age groups, and the number of doctors was categorized into three natural and approximately equally sized groups. The number of different ATC codes for each patient was categorized according to quintiles. Preliminary analyses indicated that the number of drugs acted as an intermediate variable for the number of doctors prescribing. In order to avoid overadjustment bias in the estimate of OR (number of doctors), the number of drugs was treated as an effect mediator and was omitted as a variable in the final regression model [43]. Bar graphs with confidence intervals were used to present mean proportions of PIMS in the quintile groups of number of drugs (measured by the number of different ATC codes). Analyses showed that the average number of PIMs and the number of ATC codes were closely linked (Fig. 2).

Proportion of patients receiving (one or more) potentially inappropriate medication (PIM) in relation to the total number of pharmaceutical substances received
Results
Sample characteristics
Study population characteristics are shown in Table 1. There were no missing values in the analyses.
Median number of prescriptions dispensed to each individual was 18 (IQR 10, 30; range 1–654). Median number of different drugs prescribed to each individual was 7 (IQR 4, 10; range 1–45), and one in five received more than 10 different ATC-coded drugs. Five percent of the elderly had 67 or more prescriptions processed in 1 year. Median number of prescribers for each individual was 2 (IQR 4, 10; range 1–24).
Prevalence of potentially inappropriate medication use
According to the NORGEP criteria, 155,341 persons ≥70 years [34.8% of the study population (99% CI 34.7–35.0)] received 1 or more PIM, 64,331 (14% of the study population) received 2 or more, and 3,360 people (0.8%) were affected by 5 or more PIMs with a maximum of 12 different indicator hits affecting 1 person (Table 2). The total number of hits was 259,653.
Prevalence of PIMs is shown in Table 3. Almost 1 in 10 (8.9%) was prescribed diazepam (Table 3); among these 84.5% had only one dispensing. One out of four (24%) was given zopiclone. Of the zopiclone users, 13.4% received too high a dosage; among these, the average daily dose was 10.7 mg/day. Approximately 5% were using three or more drugs from the groups of centrally acting analgesics, antipsychotics, antidepressants, and/or benzodiazepines concurrently.
More than half of PIMs in this survey (155,551 hits, 59.9%) were derived from the criteria associated with psychoactive substances, affecting 107,725 persons (24.2%). We found 864 patients (0.2%) that met five or more different criteria for potentially harmful psychoactive substances.
About 7% of the elderly used nonsteroidal anti-inflammatory drugs (NSAIDs) concurrently with angiotensin-converting enzyme (ACE ) inhibitors or angiotensin II receptor blockers (ARBs), a combination that is associated with increased risk of developing drug-induced kidney failure (Table 3). An equal 7% used NSAIDs and diuretics concurrently, reducing the effect of diuretics. Among the 62,987 who received NSAIDs + diuretics or NSAIDs + ACE (or ARB) inhibitors, 20,244 (32.1%) met both criteria.
Six of the indicators in the NORGEP list reflect inappropriate drug use that may lead to increased risk of bleeding (all four criteria involving warfarin and NSAIDs in combination with glucocorticoids and SSRIs, Table 3). We found that 22,838 (5.1%) persons were affected by at least one of these criteria, 1,800 (0.4%) by two, and 424 persons (0.1%) were concurrently exposed to three or more drug combinations where each one alone increases the risk of bleeding.
Predictors of potentially inappropriate medication use
The mean proportion of PIM (yes/no) increased almost linearly with the quintile of number of different drugs (measured by the number of different ATC-coded substances) given to each person (Fig. 2). Among those receiving 1–3 different drugs over the year, 9.0% had at least one PIM, whereas among the approximately one-fifth receiving more than 10 different drugs, two-thirds (65.5%) had at least one PIM.
Prevalence of PIMs among females was 39.3%, and among males 28.5% (Table 4). Bivariate analysis between gender and PIMs revealed a significant gender difference, where females were at higher risk for PIMs (OR 1.62, 99% CI 1.60–1.65). Multivariate analysis left this relationship unchanged (OR 1.60, 99% CI 1.58–1.64). Logistic regression considering only the criteria addressing psychoactive substances further increased the odds ratio of females versus males regarding PIMs (OR 1.90, 99% CI 1.86–1.93).
The risk of receiving PIMs first increased, then decreased with patients’ age, with OR rising to 1.33 (99% CI 1.29–1.36) for those 80–84 years old and subsequently falling to 1.16 (1.06–1.28) for the 95+ age group. The same tendency was seen in the multivariate analysis, but the age effect was reduced, leaving the oldest group at no higher risk than the youngest (OR 1.05, 99% CI 0.95–1.15) in this home-dwelling population.
The risk of PIMs increased with increasing number of doctors involved in prescribing to each patient, in bivariate (OR 3.54, 99% CI 3.45–3.62 for those in the group of 5+ prescribers compared to those with 1–2 prescribers) as well as multivariate (OR 3.52, 99% CI 3.44–3.60) analyses.
To further investigate the relationship between gender and other predictors, we ran a logistic regression stratified by gender (Table 5). Elderly males had gradually increasing odds of PIMs with age (adjusted OR 1.22 for the oldest group of 95+ years compared to the youngest), whereas for females the highest OR was seen for age group 85–89 years, and the adjusted OR then fell to 1.01 (99% CI 0.90–1.12) for the 95+ age group compared to the group of 70–74 year olds. Stratified logistic regression that included only criteria associated with psychoactive substances enhanced this gender difference and showed that elderly males had increasing odds for using potentially inappropriate psychoactive drugs with increasing age (adjusted OR 1.78, 99% CI 1.42–2.23).
Employing the alternative logistic regression model, including number of drugs as a factor, with interaction variables, not stratifying by gender, we found that increasing number of prescribers did not increase the odds for PIMs—an expected finding when over-adjusting with an intermediate variable.
Discussion
According to our estimates, approximately one-third of the elderly Norwegian home-dwelling population was exposed to potentially inappropriate medications in 2008. Due to the large number of cases the results are robust, with narrow confidence intervals. In a register study like this, the problem of recall bias is eliminated.
An important strength of this study is the access to such comprehensive data—the total prescription-based medication dispensed outside institutions to a large proportion of the elderly population in a society, regardless of prescriber. Data on drugs sold over-the-counter are not included, but Norway has strict limitations to drug detailing, and few drugs can be bought without a prescription. The only over-the-counter drugs relevant for these criteria are NSAIDs, including ibuprofen; 17 million DDDs of this drug were traded without prescriptions in 2008. Thus, the true rate of the criteria concerning NSAIDs will be higher than recorded here, whereas for the other criteria data are comprehensive.
A limitation to this study is the lack of clinical data and data on sociodemographic characteristics as possible predictors for PIMs. So far no studies on the clinical relevance of the NORGEP criteria have been performed. The problem of under-prescribing is also an important issue that is not addressed through the NORGEP criteria; in many cases, there is a need not only to discontinue inappropriate medications, but also to add other, appropriate medications.
The NORGEP criteria is a list of pharmacological rather than clinical inappropriateness; the list does not include drugs such as hypoglycemic medications or digoxin, drugs that carry a high risk of serious adverse effects [44], have a narrow therapeutic spectrum and need monitoring, but that are not in themselves inappropriate. Questions left unanswered are whether or not monitoring of such drugs is sufficient or indeed whether medications are given at a correct indication or at a correct dose. Given a certain percentage of errors in these areas, the true amount of problematic drug use in the elderly population is likely to be even higher than found in this study.
However, extra measures can be undertaken by doctors before prescribing drugs, measures such as altering warfarin dose and/or intensifying monitoring during and after a course of erythromycin. Adequate interventions such as these will not be registered in this survey. It is also important to bear in mind that in some instances, a drug on the NORGEP criteria list may be a rational choice for an individual patient. There will be situations where the prescriber will have to choose the lesser of two evils—situations more frequently encountered in the very old and frail. Quality indicators can never replace clinical judgment. Yet doctors should always be aware of the risks associated with the use of PIMs, try to minimize the use of such drugs, and monitor carefully for harmful side effects when they still choose to prescribe them.
This study found elderly women to be at particular risk for PIMs. Some earlier studies [35, 45] looking at gender differences have also found that elderly females were more frequently exposed, whereas a review article by Aparasu et al. [27] found this relationship to hold only in the univariate analysis, with a multivariate analysis showing the true relationship to be between the number of drugs and PIMs, not gender and PIMs. In the statistical model used here, the number of different ATC-coded drugs was regarded as an intermediate variable and thus excluded from the analysis. However, in order to test the stability of the results different logistic regression models were tested, including a model where the number of drugs was included as a factor in the regression. We found remarkably stable estimates for gender differences regardless of statistical model tested; all models had adjusted ORs within the range 1.53–1.66.
The finding of 35% prevalence of PIMs in this population reveals large potentials for quality improvement and a need for increased focus on the topic of inappropriate medication use in the elderly. Revising medication lists will become an increasingly important task for doctors in the years to come, in a post-demographic transition setting with an increasing number of drugs available for the old and frail. Family physicians are in a particular position to survey the overall medication use for their older patients, and this task should have priority in clinical general practice. Computer-based systems such as the one used in this survey can be implemented as decision resources, similar to the system found to be effective by Mattison et al. [46], for instance as a pop-up window in electronic medical records systems.
The extensive amount of potentially harmful medication use in today’s elderly brings up the question of whether what is good for the disease is necessarily good for the patient. Single-disease guidelines for prescribing that now prevail may not always be the best suited decision tools, especially in the case of elderly patients with multi-comorbidities. There is a need for new, global assessment tools for prescribing that take into consideration the total situation of each individual.
Conclusions
One in three elderly ≥70 years in the Norwegian home-dwelling population were exposed to potentially inappropriate medications in 2008. Among the one-fifth of the study population using more than 10 different drugs, two-thirds were exposed to at least one inappropriate drug. Elderly females were at particular risk for drug-related harm, especially from use of psychoactive substances.
This study shows a need for stronger emphasis on the dangers of polypharmacy and possible negative side effects from medication use in elderly people. Further research is needed to explore the clinical significance of this considerable level of potentially inappropriate medication use, including the gender differences revealed here.
References
Pirmohamed M, James S, Meakin S, Green C, Scott AK, Walley TJ, Farrar K, Park BK, Breckenridge AM (2004) Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 329(7456):15–19. doi:10.1136/bmj.329.7456.15
Wester K, Jonsson AK, Spigset O, Druid H, Hagg S (2008) Incidence of fatal adverse drug reactions: a population based study. Br J Clin Pharmacol 65(4):573–579. doi:10.1111/j.1365-2125.2007.03064.x
Lazarou J, Pomeranz BH, Corey PN (1998) Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 279(15):1200–1205
Ebbesen J, Buajordet I, Erikssen J, Brors O, Hilberg T, Svaar H, Sandvik L (2001) Drug-related deaths in a department of internal medicine. Arch Intern Med 161(19):2317–2323. doi:ioi00941
Viktil KK, Blix HS, Moger TA, Reikvam A (2007) Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol 63(2):187–195. doi:10.1111/j.1365-2125.2006.02744.x
Lapi F, Pozzi C, Mazzaglia G, Ungar A, Fumagalli S, Marchionni N, Geppetti P, Mugelli A, Di Bari M (2009) Epidemiology of suboptimal prescribing in older, community dwellers: a two-wave, population-based survey in Dicomano, Italy. Drugs Aging 26(12):1029–1038. doi:10.2165/11319390-000000000-00000
Rønning M, Berg C, Furu K, Litleskare I, Mahic M, Sakshaug S, Selmer R, Strøm H (2009) The Norwegian Prescription Database 2004–2008. Norwegian Institute of Public Health, Oslo
Garfinkel D, Mangin D (2010) Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med 170(18):1648–1654. doi:10.1001/archinternmed.2010.355
Iyer S, Naganathan V, McLachlan AJ, Le Couteur DG (2008) Medication withdrawal trials in people aged 65 years and older: a systematic review. Drugs Aging 25(12):1021–1031. doi:10.2165/0002512-200825120-00004
Hilmer SN, Mager DE, Simonsick EM, Cao Y, Ling SM, Windham BG, Harris TB, Hanlon JT, Rubin SM, Shorr RI, Bauer DC, Abernethy DR (2007) A drug burden index to define the functional burden of medications in older people. Arch Intern Med 167(8):781–787. doi:10.1001/archinte.167.8.781
Grahame-Smith DG, Aronson JK (eds) (2002) Oxford textbook of clinical pharmacology and drug therapy, 3rd edn. Oxford University Press, Oxford
Gerretsen P, Pollock BG (2011) Drugs with anticholinergic properties: a current perspective on use and safety. Expert Opin Drug Saf 10(5):751–765. doi:10.1517/14740338.2011.579899
Fox C, Richardson K, Maidment ID, Savva GM, Matthews FE, Smithard D, Coulton S, Katona C, Boustani MA, Brayne C (2011) Anticholinergic medication use and cognitive impairment in the older population: the Medical Research Council Cognitive Function and Ageing Study. J Am Geriatr Soc 59(8):1477–1483. doi:10.1111/j.1532-5415.2011.03491.x
Aizenberg D, Sigler M, Weizman A, Barak Y (2002) Anticholinergic burden and the risk of falls among elderly psychiatric inpatients: a 4-year case-control study. Int Psychogeriatr 14(3):307–310
Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE (2008) The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med 168(5):508–513. doi:10.1001/archinternmed.2007.106
Page J, Henry D (2000) Consumption of NSAIDs and the development of congestive heart failure in elderly patients: an underrecognized public health problem. Arch Intern Med 160(6):777–784
Blix HS, Viktil KK, Moger TA, Reikvam A (2006) Use of renal risk drugs in hospitalized patients with impaired renal function–an underestimated problem? Nephrol Dial Transplant 21(11):3164–3171. doi:10.1093/ndt/gfl399
Griffin MR, Piper JM, Daugherty JR, Snowden M, Ray WA (1991) Nonsteroidal anti-inflammatory drug use and increased risk for peptic ulcer disease in elderly persons. Ann Intern Med 114(4):257–263
Wang PS, Bohn RL, Glynn RJ, Mogun H, Avorn J (2001) Hazardous benzodiazepine regimens in the elderly: effects of half-life, dosage, and duration on risk of hip fracture. Am J Psychiatry 158(6):892–898
Pariente A, Dartigues JF, Benichou J, Letenneur L, Moore N, Fourrier-Reglat A (2008) Benzodiazepines and injurious falls in community dwelling elders. Drugs Aging 25(1):61–70
Chang CB, Chan DC (2010) Comparison of published explicit criteria for potentially inappropriate medications in older adults. Drugs Aging 27(12):947–957. doi:10.2165/11584850-000000000-00000
Dimitrow MS, Airaksinen MS, Kivela SL, Lyles A, Leikola SN (2011) Comparison of prescribing criteria to evaluate the appropriateness of drug treatment in individuals aged 65 and older: a systematic review. J Am Geriatr Soc 59(8):1521–1530. doi:10.1111/j.1532-5415.2011.03497.x
Beers MH (1997) Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Arch Intern Med 157(14):1531–1536
Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH (2003) Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med 163(22):2716–2724. doi:10.1001/archinte.163.22.2716
Beers MH, Ouslander JG, Rollingher I, Reuben DB, Brooks J, Beck JC (1991) Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med 151(9):1825–1832
Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D (2008) STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 46(2):72–83
Aparasu RR, Mort JR (2000) Inappropriate prescribing for the elderly: Beers criteria-based review. Ann Pharmacother 34(3):338–346
van der Hooft CS, Jong GW, Dieleman JP, Verhamme KM, van der Cammen TJ, Stricker BH, Sturkenboom MC (2005) Inappropriate drug prescribing in older adults: the updated 2002 Beers criteria—a population-based cohort study. Br J Clin Pharmacol 60(2):137–144. doi:10.1111/j.1365-2125.2005.02391.x
Ryan C, O’Mahony D, Kennedy J, Weedle P, Byrne S (2009) Potentially inappropriate prescribing in an Irish elderly population in primary care. Br J Clin Pharmacol 68(6):936–947. doi:10.1111/j.1365-2125.2009.03531.x
Maio V, Del Canale S, Abouzaid S (2010) Using explicit criteria to evaluate the quality of prescribing in elderly Italian outpatients: a cohort study. J Clin Pharm Ther 35(2):219–229. doi:10.1111/j.1365-2710.2009.01094.x
Fialova D, Topinkova E, Gambassi G, Finne-Soveri H, Jonsson PV, Carpenter I, Schroll M, Onder G, Sorbye LW, Wagner C, Reissigova J, Bernabei R, Ad HOC PRG (2005) Potentially inappropriate medication use among elderly home care patients in Europe. JAMA 293(11):1348–1358
Straand J, Rokstad KS (1999) Elderly patients in general practice: diagnoses, drugs and inappropriate prescriptions. A report from the More & Romsdal Prescription Study. Fam Pract 16(4):380–388
Zhan C, Sangl J, Bierman AS, Miller MR, Friedman B, Wickizer SW, Meyer GS (2001) Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. [See comment]. JAMA 286(22):2823–2829
Brekke M, Rognstad S, Straand J, Furu K, Gjelstad S, Bjorner T, Dalen I (2008) Pharmacologically inappropriate prescriptions for elderly patients in general practice: how common? Baseline data from The Prescription Peer Academic Detailing (Rx-PAD) study. Scand J Prim Health Care 26(2):80–85
Carey IM, De Wilde S, Harris T, Victor C, Richards N, Hilton SR, Cook DG (2008) What factors predict potentially inappropriate primary care prescribing in older people? Analysis of UK primary care patient record database. Drugs Aging 25(8):693–706. doi:2586
Hamilton H, Gallagher P, Ryan C, Byrne S, O’Mahony D (2011) Potentially inappropriate medications defined by STOPP criteria and the risk of adverse drug events in older hospitalized patients. Arch Intern Med 171(11):1013–1019. doi:10.1001/archinternmed.2011.215
Fu AZ, Liu GG, Christensen DB (2004) Inappropriate medication use and health outcomes in the elderly. J Am Geriatr Soc 52(11):1934–1939. doi:10.1111/j.1532-5415.2004.52522.x
Stockl KM, Le L, Zhang S, Harada AS (2010) Clinical and economic outcomes associated with potentially inappropriate prescribing in the elderly. Am J Manag Care 16(1):e1–e10
Rognstad S, Brekke M, Fetveit A, Spigset O, Wyller TB, Straand J (2009) The Norwegian General Practice (NORGEP) criteria for assessing potentially inappropriate prescriptions to elderly patients. A modified Delphi study. Scand J Prim Health Care 27(3):153–159. doi:10.1080/02813430902992215
Furu K (2008) Establishment of the nationwide Norwegian Prescription Database (NorPD)—new opportunities for research in pharmacoepidemiology in Norway. Nor Epidemiol 18(2):129–136
Statistics Norway(2011) Statbank. http://statbank.ssb.no/statistikkbanken/Default_FR.asp?PXSid=0&nvl=true&PLanguage=0&tilside=selectvarval/define.asp&Tabellid=07459. Accessed March 10, 2011
WHO Collaborating Centre for Drug Statistics Methodology and The Norwegian Institute of Public Health (2011) ATC/DDD Index. http://www.whocc.no/atc_ddd_index/. Accessed March 24, 2011
Schisterman EF, Cole SR, Platt RW (2009) Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology 20(4):488–495. doi:10.1097/EDE.0b013e3181a819a1
Budnitz DS, Shehab N, Kegler SR, Richards CL (2007) Medication use leading to emergency department visits for adverse drug events in older adults. Ann Intern Med 147(11):755–765
Goulding MR (2004) Inappropriate medication prescribing for elderly ambulatory care patients. Arch Intern Med 164(3):305–312. doi:10.1001/archinte.164.3.305
Mattison ML, Afonso KA, Ngo LH, Mukamal KJ (2010) Preventing potentially inappropriate medication use in hospitalized older patients with a computerized provider order entry warning system. Arch Intern Med 170(15):1331–1336. doi:10.1001/archinternmed.2010.244
Acknowledgments
Dr. Nyborg has had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. MD Svein Gjelstad, Mediata AS, Tønsberg, Norway developed the computer software used in the analyses in this work and was compensated for this work from the project’s funds. Dr. Gjelstad is also a researcher at the Department of Family Medicine, Institute of Health and Society, University of Oslo, Norway but has not been a part of this project group. Contributions to the study were also made by statisticians Ingvild Dalen and Magne Thoresen, both at the Department of General Practice/Family Medicine, Institute of Health and Society, University of Oslo, Norway.
Funding
The project was funded by the Allmennmedisinsk forskningsfond (AMFF), a foundation founded and sponsored by the Norwegian Medical Association. The AMFF had no role in the design, conduct, analyses, or reporting of this study.
Conflicts of interest
The authors report no conflict of interest relevant to the topic of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nyborg, G., Straand, J. & Brekke, M. Inappropriate prescribing for the elderly—a modern epidemic?. Eur J Clin Pharmacol 68, 1085–1094 (2012). https://doi.org/10.1007/s00228-012-1223-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-012-1223-8