
Abstract
Aim
(1) To describe the prevalence of benzodiazepine use in Belgian nursing homes, with specific attention to indications and dosages. (2) To compare actual and recommended dosages of benzodiazepines for anxiety and insomnia. (3) To explore the risk profile for chronic benzodiazepine use in institutionalised older adults.
Methods
Medication charts of 1,730 residents from 76 nursing homes in Belgium were collected and analysed, using the ATC classification. Drug name, indication and daily dosage were recorded. From authoritative international sources, we extracted for each drug and each indication a daily dosage recommended not to be exceeded in older adults for comparison with observed actual dosages.
Results
Among the chronic benzodiazepine or z-drug (BZD/Z) users (50% of the residents), the leading indication was ‘insomnia’ (59% of the users) followed by ‘anxiety’ (17%) and ‘unrest’ (10%). In the chronic prescriptions of BZD/Zs indicated for insomnia, the actual daily dose exceeded the geriatric upper limit in 95% of lormetazepam prescriptions, 82% of zolpidem, 78% of zopiclone and 35% of lorazepam prescriptions. For anxiety, daily doses also exceeded the limit but not to the same extent. Multivariate analysis showed BZD/Z use was positively associated with pain (OR 1.58, 95% CI 1.27–1.97), constipation (OR 1.43, 95% CI 1.16–1.76) and depression (OR 1.68, 95% CI 1.35–2.08). Residents with dementia were less likely to receive a BZD/Z (OR 0.60, 95% CI 0.48–0.74).
Conclusion
Efforts to reduce the use of BZD/Zs in nursing homes should concentrate on insomnia, with interventions aimed at reducing too high prevalence of chronic use and too high daily dosages in this indication.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Benzodiazepine utilisation in older adults is high, with intake rates ranging from 28 to 55% in European nursing homes [1–4].
Benzodiazepines are mainly indicated for the short-term treatment of insomnia and anxiety [5, 6]. Long-term use of benzodiazepines is discouraged in guidelines [5, 7, 8] because of the lack of effectiveness after 4 weeks [9, 10], the increased risk of dependence and abuse, and withdrawal syndromes [11, 12]. Moreover, it has been hypothesized that long-term use might have a detrimental effect on cognition and a potential acceleration of cognitive impairment [13–15].
High benzodiazepine utilisation in older adults is especially worrying, since age-related pharmacokinetic and dynamic alterations may lead to an increased risk of amnesia, confusion, sedation [16, 17], hangover effects [18, 19] and subsequent risk of falling [20].
International drug formularies [21–23] recommend dose reduction when using benzodiazepines in older adults. Moreover, in several attempts to develop prescribing quality indicators, upper limits for dosages in older adults have been established for some benzodiazepines as part of lists with explicit criteria for inappropriate prescribing [24–26]. In addition, benzodiazepines are the most recurring group of drugs in terms of chronic prescribing and in terms of inappropriate psychotropic polypharmacy. Numerous studies have explored benzodiazepine utilisation in older adults, but they are often limited to the description of crude utilisation data, without looking deeper into active substances, dosages and indications. Previous articles indicate the need for documentation of indications to properly evaluate the appropriateness of psychotropic drug use [27, 28]. Therefore, the aim of this study was to describe the prevalence of benzodiazepine use in Belgian nursing homes, with attention to indications and dosages for each of the commonly used drugs. Furthermore, we compared actual dosages with recommended dosages in older adults and explored the risk profile for chronic benzodiazepine use.
Methods
Data for this secondary analysis study were obtained from a multicentre study, investigating the overall drug utilisation in Belgian nursing homes. A detailed description of the methods and findings of this study was published elsewhere [1, 29].
Setting
Belgium has a mixed, public/private health care system. The system is fee for service. An essential principle of the Belgian health care system is the patient’s freedom of choice between a wide range of independent care providers without a listing system. In particular, the Belgian long-term residential care structure consists of residential and/or nursing homes for older people, which offer a home alternative with or without nursing care. Governance of nursing homes for older people is either public (community health services) or private (predominantly non-profit). Each nursing home has a medical coordinator who is a general practitioner, additionally educated in care for older people. Most of the residents are still treated by their former GP, with an average of 32 visiting GPs per nursing home. Thereby, the GP has the responsibility for the treatment and medication policy. Periodic reassessment of the medication charts (i.e. a protocol for monitoring and discontinuation of therapy) is not mandatory.
Data collection
The PHEBE study (Prescribing in Homes for the Elderly in BElgium) was a cross-sectional, descriptive study of a representative, stratified random sample of 76 Belgian nursing homes. Data collection at the resident level included administrative, clinical and medication data. To score the activities of daily living (ADL), we used the Katz scale [30], which is a mandatory instrument in Belgian nursing homes. The progression of disorientation as proxy for dementia severity was also scored by this instrument, ranging from a score of 1 (no dementia) to 5 (severe dementia).
For collecting clinical data, a checklist with 28 items, focusing on clinical problems (e.g. diseases with a clear cut diagnosis such as COPD, cardiovascular diseases) and on care problems (e.g. problems associated predominantly with nursing care burden such as incontinence, pain, risk of falling) was sent to the general practitioner (GP) of each included resident. The 28-item checklist of clinical conditions was designed specifically for this study, with the items selected based on existing prescribing quality indicators for the elderly (BEERS, BEDNURS, ACOVE). It was pilot tested in two nursing homes.
The GP received a printout of the medication chart for verification of the medication use and was asked to tick a predefined list of main indications for each medication. Residents considered by their GP as having a palliative status were excluded from the analysis.
Classification of benzodiazepines
Benzodiazepines (BZD), a group of psychoactive drugs with sedative, hypnotic, anxiolytic, anticonvulsant, muscle relaxant and amnesic action [5], were coded according to the Anatomical Therapeutic and Chemical (ATC) classification [31]. We investigated the benzodiazepines available on the Belgian pharmaceutical market of the ATC classes hypnotics (N05CD), anxiolytics (N05BA) and also the related z-drugs (N05CF). This classification is not strictly linked to the clinical indication, as most of the benzodiazepines have a mix of different pharmacological actions. Clonazepam (N03AE01), mostly used for the indications ‘restless legs’ and ‘epilepsy’, and tetrazepam (M03BX07), used as a muscle relaxant, were not included in this study. Duplicate use therapy was defined as the concomitant use of two or more different benzodiazepines or z-drugs (BZD/Z). The focus of this study was chronic use, which was defined as daily use for at least 3 months. We analysed two levels describing BZD/Z use: the prescription (medication) and the resident level. Indications were analysed at resident and prescription level and dosages at prescription level only.
Indications and dosages
The indication for each BZD/Z drug was obtained from the GP who ticked an item on a predefined list of indications: anxiety, insomnia, unrest, epilepsy, muscle tension and acute agitation. Only the indications anxiety, insomnia and unrest were analysed in depth, as the other indications were not prevalent enough. Unrest is the symptom targeted by mild sedatives, intended to calm a restless patient. It is to be distinguished from the narcotic sedation used in the palliative setting. When a physician ticked two or more indications for the same BZD/Z, we classified this as ‘multiple indications’. Only BZD/Zs with a minimum frequency of 15 prescriptions were reported in this study.
The daily dosage of each BZD/Z in each patient was recorded by summing the doses taken at the different points of intake during 1day. Comparison between prescribed daily dosages of a BZD/Z for different indications was made when at least five prescriptions for each indication were present. We also analysed the different points of intake to see fractionation.
Determination of the daily dose recommended not to be exceeded in older adults
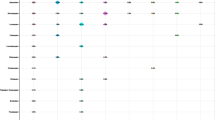
Reviewing several international pharmaceutical sources with dose recommendations for older adults, we selected three international formularia [21–23] and three explicit criteria for inappropriate prescribing for older adults [24–26] that mentioned detailed information per active substance. These sources were the basis of selecting ‘the geriatric upper limit’ i.e. the daily dose recommended not to be exceeded in the geriatric population. We focused on specific doses associated with the indications ‘insomnia’ and ‘anxiety’ and selected the dose which was advised by the majority of the sources. Specific dose recommendations for sedative action for the indication ‘unrest’ were not found in these sources.
For lorazepam only, we found separate doses for insomnia and for anxiety. For alprazolam, bromazepam and prazepam, our sources only mentioned a dose for the indication of anxiety. For the indication of insomnia, we found specific dose recommendations for lormetazepam, zolpidem and zopiclone. The recommendations retrieved from the various sources, the selected geriatric upper limit and the relation with the defined daily dose (DDD) and diazepam equivalent are presented in Fig. 1.

Recommended daily doses not to be exceeded in older adults
To calculate the percentage of prescriptions exceeding the geriatric upper limit, we compared the actual daily dosages for each prescription identified in the study with the geriatric upper limit.
Statistics
The data were analysed using the statistical package SPSS version 18. The alpha level of significance was set at p < 0.05.
In a preliminary analysis investigating BZD and z-drug use separately, we found no differences in resident characteristics. Consequently, all users were grouped together in one “BZD/Z” group for further analysis.
We used descriptive statistics to explore indications and dosages. To detect differences in prescribed daily doses for different indications, we used non-parametric statistics (medians and the Mann-Whitney U-test). To explore a risk profile for BZD/Z use, we compared users and non-users. In univariate analysis, we used the chi-squared test for dichotomous variables and independent t-tests for continuous variables. For multivariate analysis, we used a stepwise regression model with the statistically significant variables from the univariate analysis. To compare the characteristics of chronic users of BZD/Zs in different indications (anxiety, insomnia, unrest), we used the chi-squared test for dichotomous variables and one-way ANOVA for continuous variables.
Results
Description of the study population
Medication data and clinical information of 1,730 residents were included in the analysis. The mean age was 85 years (range 60–104) and 78% of residents were female. In 48% of the population, the treating physician diagnosed dementia and in 36% depression (Table 1). A combination of these two care problems was seen in 15% of the residents.
The residents used a mean of seven chronic medications per resident, ranging from no medication (in less than 1% of the residents) to 22 medications. The most frequently used drugs were central nervous system drugs with benzodiazepines and z-drugs (BZD/Z) antidepressants, antipsychotics and anti-dementia drugs at frequencies among all residents of 53, 40, 33 and 8% respectively (Table 1).
Descriptive analysis at the resident level: prevalence of BZD/Z users and indications
The prevalence of BZD/Z drug utilisation among Belgian nursing home residents (n = 1,730) was 53% (n = 918). Chronic use was present in 50% (n = 859) of the residents, and 3% used a BZD/Z only occasionally. The use of a single chronic BZD/Z was seen in 42% of the residents, while 8% had two to three chronic BZD/Zs on their medication chart (Table 2).
Among the chronic users using a single BZD/Z (n = 729), the indication was missing in 126 residents. An analysis of the characteristics of residents for whom the indication was missing revealed no significant differences. Hence, the distribution of indications was extrapolated to the group of chronic users of a single BZD/Z.
The leading indication was insomnia (59%), followed by anxiety (17%), unrest (10%), and ‘other indications’ (4%); the use of one BZD/Z for multiple indications was 10% (Table 2). When a resident received two or three chronic BZD/Zs, there was mostly a different indication for each of the prescribed BZD/Zs, most often a mix of anxiety, insomnia or unrest.
Descriptive analysis at the prescription level: prevalence and dose analysis per indication
The 859 residents on chronic BZD/Zs received a total of 1,001 chronic BZD/Z prescriptions for different indications (Table 3).
Of a total of 448 chronic prescriptions for insomnia, physicians prescribed 16 different BZD/Z drugs: 46% hypnotics (N05CD) and 27% z-drugs (N05CF), but also 27% anxiolytics (N05BA). The dominant sleeping pill was the hypnotic lormetazepam (38%), followed by zolpidem (23%). Of a total of 186 prescriptions to treat anxiety, physicians prescribed 13 different BDZ/Zs, predominantly anxiolytics (alprazolam 36% and lorazepam 27%). Of a total of 94 prescriptions to treat unrest, 16 different BZD/Zs were prescribed with a wide variety of anxiolytics (but predominantly lorazepam 39%) and also some typical hypnotics and z-drugs (27%) (Table 3).
When comparing the dosages of the prescriptions of an individual BZD/Z used for different indications, the prescribed daily dosages of prescriptions for insomnia were similar to the dosages of prescriptions for unrest, while for anxiety the daily dosages were higher (Table 3). For the treatment of anxiety, the daily dosage was divided into two to four administrations per day in 37% of these prescriptions. For the treatment of unrest, we saw fractionation in only 8% and no fractionation for insomnia as all prescriptions mentioned one dose at bedtime.
Compliance with ‘the geriatric upper limit’
In Table 4 we give the percentage of prescriptions with a dose higher than ‘the geriatric upper limit’. In the prescriptions for insomnia, this limit was exceeded for lormetazepam in 95%, zolpidem in 82%, zopiclone in 78% and for lorazepam in 35% of all chronic prescriptions. In the prescriptions for anxiety the ‘geriatric upper limit’ was also exceeded but not in such high percentages: for alprazolam in 30%, lorazepam in 12%, bromazepam in 11% and for prazepam in 5% of all chronic prescriptions.
Comparison between BZD/Z users and non-users
Univariate analysis showed that BZD/Z users had a significantly higher usage of chronic medications and antidepressants; a higher frequency of care problems such as constipation, depression and chronic pain; and a lower frequency of dementia and incontinence. We found no association between BZD/Z use and the physicians’ perception of the risk of falling, nor with the frequency of clinical problems such as cardiovascular diseases, diabetes and COPD (Table 5).
In multivariate analysis, BZD/Z use was more frequent in female residents (OR 1.32, 95% CI 1.03–1.68) and residents with chronic pain (OR 1.58, 95% CI 1.27–1.97), constipation (OR 1.43, 95% CI 1.16–1.76) and depression (OR 1.68, 95% CI 1.35–2.08), and less frequent in residents with incontinence (OR 0.71, 95% CI 0.57–0.88) and dementia (OR 0.60, 95% CI 0.48–0.74 (Table 5).
Comparison between BZD/Z users for the different indications
Depression, chronic medication, antidepressant and antipsychotic use were significantly more likely to be present when a resident took a BZD/Z for anxiety rather than for insomnia and unrest. We found no significant differences in the risk profiles of residents with BZD/Z use for insomnia versus use for unrest (Table 6).
Especially among users with the indication of insomnia, we observed a gradual decrease in BZD/Z use as dementia progressed (Fig. 2).

Changes in indication for benzodiazepine and z-drug use in relation to increasing dementia
Relationship with institutional characteristics
BZD/Z drug use was not associated with institutional characteristics such as private or public facility, size or staffing.
Discussion
Originality of the study
In this observational cross-sectional study of chronic use of benzodiazepines and z-drugs (BZD/Z) in Belgian nursing homes, the prevalence of usage of these drugs has been examined in depth per indication, and differences in dosing practices per indication have been analysed.
We confirmed the high prevalence of chronic BZD/Z use (half of the residents) in this setting, as found in numerous other studies [2, 4, 32]. We found that insomnia was the main indication for chronic use and was treated at higher dosages than recommended in older adults [21, 23, 25, 26]. This finding is not striking, but our study is the first to scientifically confirm the assumption that insomnia is the most prevalent indication for BZD/Z use. We were able to determine interesting elements for a risk profile of BZD/Z use in multivariate analysis, such as positive associations with female gender, obstipation, depression, chronic pain and polypharmacy (including polypharmacy with other psychotropics), and negative associations with dementia and incontinence. There was a puzzling absence of association with age, risk of falling, clinical problems and institutional characteristics.
This study in a large representative sample of Belgian nursing home residents provides long-awaited information on indications and dosages of benzodiazepines [33]. Actual daily dosages were compared to the geriatric upper limit, a pragmatic threshold determined from authoritative international pharmaceutical sources.
Strengths and limitations
One strength of our study was the substantial and representative sample of Belgian nursing home residents [29]. In neighbouring European countries [2–4], similar prevalence numbers of benzodiazepine use have been found. In the United States [27], there is a lower use of benzodiazepines due to the safety warnings issued in the late 1980s and due to specific actions tackling the high use of these drugs (Medicare Part D). Another strength of this study is that our data collection was based on reliable recording from primary sources, namely medication charts and direct clinical information from the treating GP. Another strong aspect of this study was our attempt to list most of the existing recommendations for older adults regarding dosages of BZD/Zs. However, we did not use an explicit method to extract the geriatric upper limit and we limited ourselves to the most abundantly prescribed BZD/Zs in Belgium. This geriatric upper limit is a threshold based on a pragmatic analysis of different sources, and therefore not a gold standard nor a rigid criterion for inappropriate prescribing.
One limitation was that we did not use internationally validated criteria to evaluate (severity of) dementia. In this cross-sectional study, we were not able to investigate the distribution of the duration of chronic use, nor it was possible to investigate temporal changes and the relationship between process and outcome. Indications for BZD/Z drugs were collected by interviewing the GP, which may have influenced data reliability. To reduce the complexity of the analysis, we narrowed our in-depth analysis of indications to chronic users with only one BZD/Z and therefore only one indication and disregarded residents on multiple BZD/Zs (8% of all residents) or residents on a BZD/Z with more than one indication (10% of the residents on a single chronic BZD/Z). In addition, there was a large number of missing indication data (17%), which might reflect an uncertainty of the treating GPs when discriminating among the indications of anxiety, insomnia, and unrest. This pragmatic approach might have introduced some bias in the estimation of the prevalence.
Critical discussion of the main findings
Insomnia
Our study showed that the number one indication for BZD/Z drugs in this setting was insomnia and to a far lesser extent anxiety and unrest.
A striking finding was that almost all use of BDZ/Z drugs for insomnia was chronic, which is generally considered to be inappropriate [25, 34]. In order to avoid chronic prescribing, guidelines such as the British National Formulary and the Belgian drug code [21, 35] point out that before prescribing a hypnotic, the cause of the insomnia should be established and, where possible, underlying factors (such as depression or ‘restless legs’ ) should be treated [36, 37]. Establishing a good sleep hygiene is the first choice but is not easy to implement in nursing homes. When a pharmacological treatment seems necessary, hypnotics should be reserved for short courses (<3 weeks) in the acutely distressed, and routine/chronic prescribing is undesirable [21].
With regard to the drug choice within the benzodiazepine drug class (with hypnotic, anxiolytic, sedative, muscle-relaxant and amnesic action) for the indication of insomnia, hypnotic benzodiazepines and z-drugs were mainly used, but also the anxiolytics lorazepam and bromazepam.
With regard to dosages for the different indications, we found that, especially in patients treated for insomnia, the daily dosages of the hypnotic benzodiazepines, the z-drugs, and the anxiolytic lorazepam exceeded the geriatric upper limit. However, in terms of diazepam equivalence, the dosages were still considerably lower than the dosages used when treating patients with anxiety.
It is generally known that older adults need a dose reduction, but specific information about this reduction is hard to find. Most sources stay vague and point at a dose reduction of 50% and a slow titration. Hence, it is no surprise that there are no clear guidelines and that GPs are not aware of geriatric optimal dosing. A comparison of the geriatric upper limit with the defined daily dose (DDD) revealed that the two values coincided for anxiety, but for insomnia, the geriatric upper limit was half the DDD (Fig. 1). This may be one methodological explanation for the high prevalence of dosages exceeding the limit in prescriptions indicated for insomnia. Another explanation is that physicians titrate the dosage upwards when tolerance sets in, as expected for benzodiazepine use. Also, one culprit may be the unavailability of dosages packaged for the geriatric patient. Lormetazepam, for example, is on the Belgian market in package doses of 1 or 2 mg and consequently exceeds the recommended 0.5 mg/day for older adults. This is also the case for the package dosages of zolpidem (only packages of 10 mg on the market).
In our study, the hypnotics users, and especially the residents receiving a BZD to treat anxiety, were more likely to suffer from depression and to be receiving a prescription for an antidepressant. This chronic concomitant use of psychotropic drugs to treat depression is not appropriate in geriatric patients, who are already at an increased risk of interactions and adverse drug reactions. On the one hand, it is not surprising that we found an association between depression and BZD/Z use because depression can be the reason for initiating a BZD/Z drug, especially when depression is related to a disturbed sleep pattern and anxiety [38]. On the other hand, a study in 2007 revealed that the use of hypnotics was associated with an increased incidence of depression, suggesting hypnotics may be contra-indicated when there is a risk for depression [39].
Unexpectedly, we saw a gradual decrease in the use of sleeping pills when dementia progressed, although it is well known that patients with dementia often have nocturnally disturbed sleep [40]. As a sleeping problem is frequently an explicit complaint, uttered by the patient [41], it is possible that prescribing sleeping pills is demand-driven. Thus, when residents with severe dementia lose the ability to express the need for sleeping pills, their prescription might not get renewed.
Anxiety
In patients using only a single BZD/Z chronically, an indication of anxiety alone occurred in fewer than one in five patients. However, this indication was also present in patients using multiple BDZ/Z drugs or a single BZD/Z drug for multiple indications. Using BZDs chronically to treat mild anxiety is considered to be inappropriate [8]. At the onset of treatment of depression, a benzodiazepine could be used as an adjuvant, as the anti-anxiety effect of some antidepressants can take 2 to 4 weeks [42]. However, to avoid chronic use, this dual therapy should be tapered over time [43].
For this indication, the drugs of choice were exclusively the anxiolytic ATC-class drugs, used in daily dosages higher than the dosages used when indicated for insomnia, but closer to the geriatric upper limit (and to the DDD). It is logical that daily dosages are higher for anxiety as they are more frequently dispensed during the day, unlike sleeping pills, which are administered once daily in the evening.
The indication of anxiety was associated with a more intense polypharmacy, more antidepressants (and more depression), and more antipsychotics. Hence, efforts to withdraw from BDZ/Z drug usage should be seen in the broader context of mental health, and treatment of behavioural and psychological symptoms of dementia.
Unrest
A variety of benzodiazepines in different ATC classes were used to treat unrest. The prescribed daily doses of these BZD/Z drugs for this indication were similar to the prescribed daily doses of these BZD/Z drugs used for the treatment of insomnia. Furthermore, we observed no differences in characteristics between a resident using a BZD/Z drug for insomnia and unrest. Sedative action in this setting is considered to provide calming effects (different from the narcotic aim in a palliative care context and different from control of acute agitation). This suggests some semantic overlap between the terms ‘sedative’ and ‘hypnotic’ action, not only in literature but also in daily practice.
Risk profile of BDZ/Z drug users
Our multivariate comparison of users versus non-users revealed positive associations with care problems such as obstipation and chronic pain, possible causes of irritation and sleeplessness leading to BZD/Z use. The negative association between incontinence and BZD/Z use might be explained by covariance with dementia and the use of nocturnal incontinence material.
The association with polypharmacy (more specifically psychotropic polypharmacy) calls for a comprehensive approach to assure the quality of psychotropic pharmacotherapy for mental health in nursing homes [44].
In other studies an association was found between BZD/Z use and risk of falling [20, 45–47]. In this cross-sectional study we did not observe this, possibly because treating physicians failed to perceive the risk of falling as a consequence of BZD/Z use or because of the multifactorial nature of this association.
We did not find significant associations between BDZ/Z drug use and institutional characteristics (including staffing), contradicting the popular belief that high hypnotic usage is associated with low staffing [48].
Implications for practice and research
The contradiction between recommendations against long-term use of BDZ/Z drugs and the high prevalence in older adults has already been discussed often but seldom explained. Prescribers seem to be convinced of the detrimental long-term effects of benzodiazepines in older adults [49], but it seems very hard to change habitual prescribing and to overcome the fear of possible relapse and withdrawal effects for both prescribers and caregivers and for patients [50].
It is difficult to persuade patients and their physicians to stop chronic use of BDZ/Z drugs. However, a small intervention study in primary care showed that sending a letter from the physician to the BZD/Z user could have a positive impact on successful withdrawal [51, 52]. Motivation together with gradual tapering seems to be the best strategy for discontinuation [11, 53].
Previous articles on BZDs supported non-pharmacological ways to address insomnia and to avoid the initiation of benzodiazepine use [54–56]. More efforts to motivate the residents as well as the care-giving staff to do physical exercises and other activities to improve the sleep quality of older adults must be made in order to reduce persistent sleep problems and sleeping pill use [57, 58].
More emphasis should be given to at least avoiding high dosages during chronic use for older patients. This study found that prescribers do not pay attention to reducing the dosage according to existing recommendations, especially in patients treated for insomnia. We do not know whether this reluctance indirectly leads to a higher mortality [59], but several studies have described the existence of adverse effects, such as cognitive impairment [14, 15], addiction and possible withdrawal effects. The pharmaceutical companies should produce packages with appropriate dosages for older adults. But nurses and pharmacists could also play an important role in the correct administration of these drugs in older adults [60, 61].
Future research on benzodiazepines should differentiate between insomnia and anxiety or other indications. Our findings suggest that insomnia, given its high prevalence as a primary indication, deserves priority. Efforts to reduce chronic use should concentrate on reducing initiation, long-term use and excessively high dosages for this indication.
Furthermore, there is a need to strengthen the evidence base regarding the absence of long-term efficacy and the significance of adverse effects in order to persuade physicians, nurses, caregivers and patients of the positive risk-benefit balance of discontinuation attempts.
References
Azermai M, Elseviers M, Petrovic M, Van Bortel L, Stichele RV (2011) Geriatric drug utilisation of psychotropics in Belgian nursing homes. Hum Psychopharmacol. doi:10.1002/hup.1160
Gobert M, D'Hoore W (2005) Prevalence of psychotropic drug use in nursing homes for the aged in Quebec and in the French-speaking area of Switzerland. Int J Geriatr Psychiatr 20(8):712–721. doi:10.1002/gps.1349
Hosia-Randell H, Pitkala K (2005) Use of psychotropic drugs in elderly nursing home residents with and without dementia in Helsinki, Finland. Drugs Aging 22(9):793–800
Petek Ster M, Cedilnik Gorup E (2011) Psychotropic medication use among elderly nursing home residents in Slovenia: cross-sectional study. Croat Med J 52(1):16–24
Ashton H (1994) Guidelines for the rational use of benzodiazepines—when and what to use. Drugs 48(1):25–40
Neutel CI (2005) The epidemiology of long-term benzodiazepine use. Int Rev Psychiatry 17(3):189–197. doi:10.1080/09540260500071863
Canadian Agency for Drugs and Technologies in Health (CADTH) (2010) Benzodiazepines in older adults: a review of clinical effectiveness, cost-effectiveness, and guidelines. http://www.cadth.ca/media/pdf:M0022_Benzodiazepines_Elderly.pdf. Accessed 10 Aug 2011
National Institute for Health an Clinical Excellence (NICE) (2011) Generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults. http//www.nice.org.uk/nicemedia/live/13314/52599/52599.pdf. Accessed 10 Aug 2011
Martin JL, Sainz-Pardo M, Furukawa TA, Martin-Sanchez E, Seoane T, Galan C (2007) Benzodiazepines in generalized anxiety disorder: heterogeneity of outcomes based on a systematic review and meta-analysis of clinical trials. J Psychopharmacol 21(7):774–782. doi:10.1177/0269881107077355
Beland SG, Preville M, Dubois MF, Lorrain D, Voyer P, Bosse C, Grenier S, Moride Y (2011) The association between length of benzodiazepine use and sleep quality in older population. Int J Geriatr Psychiatr 26(9):908–915. doi:10.1002/gps.2623
Lader M, Tylee A, Donoghue J (2009) Withdrawing benzodiazepines in primary care. CNS Drugs 23(1):19–34. doi:10.2165/0023210-200923010-00002
Voyer P, Preville M, Cohen D, Berbiche D, Beland SG (2010) The prevalence of benzodiazepine dependence among community-dwelling older adult users in Quebec according to typical and atypical criteria. Can J Aging 29(2):205–213. doi:10.1017/S0714980810000115
Verdoux H, Lagnaoui R, Begaud B (2005) Is benzodiazepine use a risk factor for cognitive decline and dementia? A literature review of epidemiological studies. Psychol Med 35(3):307–315. doi:10.1017/s0033291704003897
Wu CS, Wang SC, Chang IS, Lin KM (2009) The association between dementia and long-term use of benzodiazepine in the elderly: nested case–control study using claims data. Am J Geriatr Psychiatry 17(7):614–620
Barker MJ, Greenwood KM, Jackson M, Crowe SF (2004) Cognitive effects of long-term benzodiazepine use—a meta-analysis. Cns Drugs 18(1):37–48
Klotz U (1998) Effect of age on pharmacokinetics and pharmacodynamics in man. Int J Clin Pharmacol Therapeut 36(11):581–585
Petrovic M, Mariman A, Warie H, Afschrift M, Pevernagie D (2003) Is there a rationale for prescription of benzodiazepines in the elderly? Review of the literature. Acta Clin Belg 58(1):27–36
Madhusoodanan SBOJ (2004) Safety of benzodiazepines in the geriatric population. Expert Opin Drug Saf 3(5):485–493
Cook PJ, Huggett A, Graham-Pole R, Savage IT, James IM (1983) Hypnotic accumulation and hangover in elderly inpatients: a controlled double-blind study of temazepam and nitrazepam. Br Med J (Clin Res Ed) 286(6359):100–102
Mustard CA, Mayer T (1997) Case-control study of exposure to medication and the risk of injurious falls requiring hospitalization among nursing home residents. Am J Epidemiol 145(8):738–745
The British National Formularium (BNF). British Medical Association and the Royal Pharmaceutical Society. http://bnf.org:bnf:index.htm. Accessed 10 Aug 2011
KNMP (Royal Dutch Society of Pharmacy) (2009) Informatorium Medicametorum. Koninklijke Nederlandse Maatschappij ter bevordering van de Farmacie. www.knmp.nl. Accessed 8 June 2011
Sweetman SC (ed) Martindale: the complete drug reference, 36th ed. Pharmaceutical Press, London
Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH (2003) Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med 163(22):2716–2724. doi:10.1001/archinte.163.22.2716163/22/2716
Rancourt CMJ, Baillargeon L, Verreault R, Laurin D, Grégoire JP (2004) Potentially inappropriate prescriptions for older patients in long-term care. BMC Geriatr 4:9
Laroche ML, Charmes JP, Merle L (2007) Potentially inappropriate medications in the elderly: a French consensus panel list. Eur J Clin Pharmacol 63(8):725–731. doi:10.1007/s00228-007-0324-2
Stevenson DG, Decker SL, Dwyer LL, Huskamp HA, Grabowski DC, Metzger ED, Mitchell SL (2010) Antipsychotic and benzodiazepine use among nursing home residents: findings from the 2004 National Nursing Home Survey. Am J Geriatr Psychiatry 18(12):1078–1092. doi:10.1097/JGP.0b013e3181d6c0c6
Holmquist IB, Svensson B, Hoglund P (2003) Psychotropic drugs in nursing- and old-age homes: relationships between needs of care and mental health status. Eur J Clin Pharmacol 59(8–9):669–676. doi:10.1007/s00228-003-0679-y
Elseviers MVSR, Soenen K, Gobert M, Van Bortel L, Van De Voorde C (2010) Drug utilisation in Belgian nursing homes: impact of residents' and institutional characteristics. Pharmacoepidemiol Drug Safety 19:1041–1048
Katz S, Akpom CA (1976) 12. Index of ADL. Med Care 14(5 Suppl):116–118
WHO Collaborating Centre for Drug Statistics Methodology (2009) ATC/DDD system. http://www.whocc.no. Accessed 20 June 2011
Westbury J, Jackson S, Gee P, Peterson G (2010) An effective approach to decrease antipsychotic and benzodiazepine use in nursing homes: the RedUse project. Int Psychogeriatr 22(1):26–36. doi:10.1017/s1041610209991128
Bartlett G, Abrahamowicz M, Tamblyn R, Grad R, Capek R, du Berger R (2004) Longitudinal patterns of new benzodiazepine use in the elderly. Pharmacoepidemiol Drug Saf 13(10):669–682. doi:10.1002/pds.908
Gallagher P, Ryan C, Byrne S, Kennedy J, O'Mahony D (2008) STOPP (Screening Tool of Older Person's Prescriptions) and START (Screening Tool to Alert Doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Therapeut 46(2):72–83
BCFI (Belgian Centre for Pharmacotherapeutic Information) (2010) Home page. http://www.bcfi.be/. Accessed 8 June 2011
B Terluin FBVH, K Van der Meer, GJH Neomagus, J Hekman, L P J Aulbers, J S Starreveld and M H Grol (2009) NHG-Standaarden Angststoornissen In: NHG-Standaarden voor huisartsened. Nederlandse huisartsen genootschap
Morin AK (2006) Strategies for treating chronic insomnia. Am J Manag Care 12(8 Suppl):S230–S245
van Vliet P, van der Mast RC, van den Brock M, Westendorp RGJ, de Craen AJM (2009) Use of benzodiazepines, depressive symptoms and cognitive function in old age. Int J Geriatr Psychiatr 24(5):500–508. doi:10.1002/gps.2143
Kripke DF (2007) Greater incidence of depression with hypnotic use than with placebo. BMC Psychiatry 7:42. doi:10.1186/1471-244X-7-42
Bliwise DL (2004) Sleep disorders in Alzheimer's disease and other dementias. Clin Cornerstone 6(Suppl 1A):S16–S28
Cook JM, Marshall R, Masci C, Coyne JC (2007) Physicians' perspectives on prescribing benzodiazepines for older adults: a qualitative study. J Gen Intern Med 22(3):303–307. doi:10.1007/s11606-006-0021-3
Manji HK, Drevets WC, Charney DS (2001) The cellular neurobiology of depression. Nat Med 7(5):541–547. doi:10.1038/8786587865
Cloos JM, Ferreira V (2009) Current use of benzodiazepines in anxiety disorders. Curr Opin Psychiatry 22(1):90–95. doi:10.1097/YCO.0b013e32831a473d
Ruths S, Straand J, Nygaard HA (2003) Multidisciplinary medication review in nursing home residents: what are the most significant drug-related problems? The Bergen District Nursing Home (BEDNURS) study. Qual Saf Health Care 12(3):176–180
Berdot S, Bertrand M, Dartigues JF, Fourrier A, Tavernier B, Ritchie K, Alperovitch A (2009) Inappropriate medication use and risk of falls—a prospective study in a large community-dwelling elderly cohort. BMC Geriatr 9:30. doi:10.1186/1471-2318-9-30
Ensrud KE, Blackwell TL, Mangione CM, Bowman PJ, Whooley MA, Bauer DC, Schwartz AV, Hanlon JT, Nevitt MC (2002) Central nervous system-active medications and risk for falls in older women. J Am Geriatr Soc 50(10):1629–1637
Boyle N, Naganathan V, Cumming RG (2010) Medication and falls: risk and optimization. Clin Geriatr Med 26(4):583–605. doi:10.1016/j.cger.2010.06.007
Svarstad BL, Mount JK (2001) Chronic benzodiazepine use in nursing homes: effects of federal guidelines, resident mix, and nurse staffing. J Am Geriatr Soc 49(12):1673–1678
Anthierens S, Pasteels I, Habraken H, Steinberg P, Declercq T, Christiaens T (2010) Barriers to nonpharmacologic treatments for stress, anxiety, and insomnia. Family physicians' attitudes toward benzodiazepine prescribing. Can Fam Phys 56(11):E398–E406
Iliffe S, Curran HV, Collins R, Kee SCY, Fletcher S, Woods B (2004) Attitudes to long-term use of benzodiazepine hypnotics by older people in general practice: findings from interviews with service users and providers. Aging Mental Health 8(3):242–248. doi:10.1080/13607860410001669778
Cormack MA, Owens RG, Dewey ME (1989) The effect of minimal interventions by general practitioners on long-term benzodiazepine use. J R Coll Gen Pract 39(327):408–411
Gorgels WJ, Oude Voshaar RC, Mol AJ, van de Lisdonk EH, van Balkom AJ, van den Hoogen HJ, Mulder J, Breteler MH, Zitman FG (2005) Discontinuation of long-term benzodiazepine use by sending a letter to users in family practice: a prospective controlled intervention study. Drug and Alcohol Depend 78(1):49–56. doi:10.1016/j.drugalcdep.2004.09.001
Denis C, Fatseas M, Lavie E, Auriacombe M (2006) Pharmacological interventions for benzodiazepine mono-dependence management in outpatient settings. Cochrane Database Syst Rev 3: CD005194 doi:10.1002/14651858.CD005194.pub2
Morin CM, Bootzin RR, Buysse DJ, Edinger JD, Espie CA, Lichstein KL (2006) Psychological and behavioral treatment of insomnia: update of the recent evidence (1998–2004). Sleep 29(11):1398–1414
Mendelson WB (1995) Long-term follow-up of chronic insomnia. Sleep 18(8):698–701
Bain KT (2006) Management of chronic insomnia in elderly persons. Am J Geriatr Pharmacother 4(2):168–192. doi:10.1016/j.amjopharm.2006.06.006
Alessi CA, Schnelle JF (2000) Approach to sleep disorders in the nursing home setting. Review article. Sleep Med Rev 4(1):45–56. doi:10.1053/smrv.1999.0066
Lyne J, Quinlivan L, Byrne CA, Malone K, Walsh C (2011) Sleep hygiene use in a psychiatry outpatient setting. Ir Med J 104(2):49–50
Charlson F, Degenhardt L, McLaren J, Hall W, Lynskey M (2009) A systematic review of research examining benzodiazepine-related mortality. Pharmacoepidemiol Drug Saf 18(2):93–103. doi:10.1002/pds.1694
Anthierens S, Grypdonck M, De Pauw L, Christiaens T (2009) Perceptions of nurses in nursing homes on the usage of benzodiazepines. J Clin Nurs 18(22):3098–3106. doi:10.1111/j.1365-2702.2008.02758.x
Verrue CL, Petrovic M, Mehuys E, Remon JP, Vander Stichele R (2009) Pharmacists' interventions for optimization of medication use in nursing homes: a systematic review. Drugs Aging 26(1):37–49. doi:10.2165/0002512-200926010-000032613
Acknowledgements
We thank Prof. Dr. Thierry Christiaens from the Department of Family Medicine and Primary Care and Dr. Hans Debruyne, psychiatrist at the Dr. Guislain Centre for Psychiatry, for their contribution.
Competing interest
There are no competing interests to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bourgeois, J., Elseviers, M.M., Azermai, M. et al. Benzodiazepine use in Belgian nursing homes: a closer look into indications and dosages. Eur J Clin Pharmacol 68, 833–844 (2012). https://doi.org/10.1007/s00228-011-1188-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-011-1188-z