
Abstract
Purpose
Cerebral vasospasm (CVS) is a frequent and unpredictable complication in patients with subarachnoid hemorrhage (SAH) and often leads to poor outcomes. This study was aimed at evaluating the efficacy and safety of fasudil in the treatment of CVS in patients with SAH.
Methods
A search was conducted using the full-text database of Chinese scientific journals, the Wanfang Database (January 1999 to November 2010), the Chinese Medical Association Digital Journal Database, PubMed, the Cochrane library, OVID, and EMBase (searching through November 2010).
Results
A total of 8 studies met the inclusion criteria. The incidence rates of symptomatic CVS and CVS confirmed by angiography among the patients in the fasudil group were only 48% (odds ratio [OR] = 0.48, 95% confidence interval [CI]: 0.32–0.72, P = 0.0005) and 40% (OR = 0.40, 95% CI: 0.24-0–67, P = 0.0004) respectively of that of the control group. The odds ratios of cerebral infarction for all cases and cerebral infarction for CVS cases in the fasudil group were only 50% (OR = 0.50, 95% CI: 0.34–0.76, P = 0.0009) and 43% (OR = 0.43, 95% CI: 0.26–0.70, P = 0.0008) respectively of that of the control group.
Conclusions
Fasudil greatly reduces the occurrence of CVS and cerebral infarction in SAH patients, significantly improves the clinical outcomes of the patients (as assessed by the Glasgow Outcome Scale). Because of the limited number of trials and samples available for analysis, the conclusions from the present study still need to be validated with results from large randomized, controlled clinical trials.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Cerebral vasospasm (CVS) is a frequent and unpredictable complication in patients with subarachnoid hemorrhage (SAH) and often leads to adverse outcomes [1]. The current treatment for CVS primarily includes the prophylactic use of vasodilators, transluminal balloon angioplasty, and triple-H therapy (hypervolemia, hypertension, and hemodilution). According to reports on clinical trials and meta-analyses, although endothelin receptor antagonists, tirilazad, nimodipine, and nicardipine, as well as transluminal balloon angioplasty, were able to prevent or reverse CVS, they could not improve clinical outcomes among the patients [2–7]. Currently, sufficient evidence to support the efficacy and safety of triple-H therapy is lacking [8].
Recent basic and clinical studies indicate that Rho-kinase is an important target in the pathogenesis of various vascular diseases [9, 10]. Increases in Rho-kinase activity lead to smooth muscle cell contraction, increased muscle fiber tension, and vascular contraction [9]. Through the inhibition of tumor necrosis factor (TNF)-induced IL-6 release [11], the Rho-kinase inhibitor fasudil performs the following actions: it inhibits the expression of tissue factors that are induced by TNF-α in vascular endothelial cells, activates the endogenous neural stem cells in the central nervous system, increases the levels of granulocyte colony-stimulating factor and astrocyte-stimulating factor, suppresses intracellular calcium release, dilates cerebral blood vessels, protects neurons, improves neurological function, inhibits ischemic cerebral injuries [12], and prevents and reverses CVS [11]. The results from one study [13–15] show that fasudil significantly improves the clinical outcome in SAH patients while preventing and reversing CVS. However, the results from other studies [16–18] do not fully support this finding. To date, no published reports have presented a systematic evaluation and meta-analysis of fasudil use in SAH treatment. Eight randomized, controlled clinical studies were included in the present study. CVS, cerebral infarction, and other indicators were assessed for efficacy analysis. A comprehensive study of the efficacy and safety of fasudil in the treatment of CVS among SAH patients was performed.
Materials and methods
Literature search strategy
The electronic databases searched in the present study included the full-text database of Chinese scientific journals, dissertations, and conference papers (for articles published from January 1994 to November 2010), the VIP journal index (January 1994 to November 2010), the Wanfang Database (January 1999 to November 2010), the Chinese Medical Association Digital Journal Database (through November 2010), PubMed (through November 2010), the Cochrane library (through November 2010), OVID (through November 2010), and EMBase (through November 2010). The Chinese search words used were “fashudier/fasudil” and “nao xueguan jingluan/cerebral vasospasm” or “zhuwangmo xiaqiang chuxue/subarachnoid hemorrhage,” and the English search words used were “fasudil” and “cerebral vasospasm” or “vasospasm” or “subarachnoid hemorrhage.” In the process of searching PubMed, the language restriction was removed. In addition, we carefully checked the studies that were included in the reference lists and satisfied the inclusion criteria of this study to identify any studies that were missed in the searches mentioned above.
Literature inclusion and exclusion criteria
The inclusion criteria were as follows:
-
1.
Controlled, prospective clinical studies on fasudil use in the prevention and treatment of non-traumatic SAH
-
2.
Studies that provided relevant calculated indicators and that could be used for data extraction for the meta-analysis
The excluded studies included the following:
-
1.
Purely descriptive studies, such as reviews and summaries
-
2.
Retrospective studies
-
3.
Repeated published studies
-
4.
Studies of questionable authenticity
Only the study methods and results in the original studies were considered in the present study, without considering sample size.
Data extraction
Based on the study objective, the following data were extracted: sample size, patient clinical classification, fasudil dosage, type and dosage of the control drug, drug administration starting time and duration, clinical assessment indicators (clinical outcomes and/or nervous system complications), assessment criteria and time, trial quality, and adverse responses.
Quality control
Two authors (G.J. Liu and Y.F. Wang) independently reviewed the literature and extracted the data following consistent standards. All of the authors participated in the discussions and decision-making processes when there was disagreement about the quality of a study. Studies that had complete data or were recently published were employed for the scalability report. The quality of all of the studies that were included in the analysis was assessed following the Jadad quality rating scale [19]. The authenticity of the studies was also evaluated. The present study did not mask the source of the studies or the affiliations of the authors.
Statistical processing
Meta-analyses were performed using Review Manager version 4.2 software provided by the Cochrane Collaboration Network. Cerebral infarction, Glasgow Outcome Scale (GOS), Glasgow Coma Scale (GCS), and other indicators were adopted as the indicators for efficacy analysis. The efficacy of fasudil and control drugs in terms of different outcome indicators was evaluated. Intent-to-treat (ITT) analysis was performed for those studies that provided data on the patients who violated the treatment protocol. The existence of publication bias in the meta-analysis was evaluated for statistically significant outcome indicators through calculating their fail-safe numbers (Nfs). Stratified analyses were conducted for each outcome indicator.
A heterogeneity test was performed for the studies before a test for overall effect. The outcome indicators in the studies with heterogeneity and the possible reason for heterogeneity were further analyzed. Sensitivity analysis was performed for all outcome indicators, including stratified analysis of outcome indicators presented in low-quality literature with data from the low-quality literature included or excluded. Outcome indicators were also analyzed using the fixed effects model and the random effects model. The odds ratio (OR) was utilized as the effect assessment indicator for categorical variables, whereas the weighted mean difference (WMD) was adopted as the effect assessment indicator for continuous variables. The patient number needed to treat (NNT) was chosen as the clinical efficacy assessment indicator for categorical variables. When calculating the OR and WMD values for each outcome indicator, the 95% confidence interval (CI) was calculated as well. P < 0.05 was considered statistical significance.
Results
Literature search results
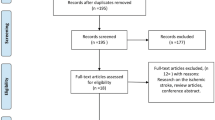
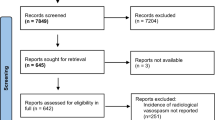
A total of 400 references were obtained in the preliminary search. Through reading of the titles, abstracts, and some full texts, the studies that were not relevant to the particular subject and those with repetitive or redundant reports were eliminated. Finally, 8 articles [13–18, 20, 21] were found to meet the criteria of this study. These 8 articles all reported controlled prospective clinical studies [13–18, 20, 21]. Among them, 6 studies reported that the patients were randomly distributed to the fasudil group and the control group [13, 15–18, 21], which was not specified in the other 2 studies [14, 20]. Nimodipine was the control for fasudil in 6 studies [13, 14, 16–18, 20, 21], with another study using a placebo as the control [15]. The final study used fasudil in addition to ozagrel in the treatment group, and ozagrel only was administered in the control group [14]. Six studies were confirmed to involve SAH caused by ruptured aneurysms [13–18], whereas the other 2 did not specify the details of the SAH mechanisms [20, 21]. A total of 843 patients were included in these 8 studies, and 71 patients (8.42%) were excluded from the analysis (69 cases because of protocol violation, and 2 were lost during the study period). The quality of all the studies that were included in the analysis was assessed according to the Jadad quality rating scale [19]. Among the 8 reports, 7 can be considered high-quality literature [13–18, 21], but the remaining study scores as low-quality literature [20]. The clinical characteristics of these 8 trials are shown in Tables 1 and 2.
Meta-analysis results (fasudil group versus control group)
Complications
Cerebral vasospasm
Four [14–16, 18] studies reported data from the patients with symptomatic vasospasm. The meta-analysis results indicated no statistically significant difference in the incidence rate of symptomatic vasospasm between the groups of patients (P = 0.19). The cause of the heterogeneity among the references (P(χ2) = 0.03) needs to be further analyzed. When the single reference with a relatively low-quality score was excluded [14], the meta-analysis showed that the incidence rate of symptomatic vasospasm of the fasudil group was only 48% of that of the control group (OR = 0.48, 95% CI: 0.32–0.72, P = 0.0005, P(χ2) = 0.64; Table 3). Sensitivity analysis suggested that the heterogeneity within the group was caused by different study methods. The NNT results indicated that, compared with the control group, 1 of every 2 patients in the fasudil group avoided symptomatic vasospasm (see Table 5).
Four articles [15, 17, 18, 20] reported data on the patients with CVS confirmed by angiography 14 days after treatment. The meta-analysis results showed that the incidence rate of CVS confirmed by angiography 14 days after treatment in the fasudil group was only 40% of that of the control group (OR = 0.40, 95% CI: 0.24–0.67, P = 0.0004, P(χ2) = 0.29). When the low-quality reference was excluded, the meta-analysis results demonstrated that the incidence rate of CVS confirmed by angiography 14 days after treatment in the fasudil group was only 45% of that of the control group (OR = 0.45, 95% CI: 0.27–0.76, P = 0.003, P(χ2) = 0.32; Table 3). The NNT results indicated that compared with the control group, 1 out of every 3 patients in the fasudil group avoided angiography-confirmed CVS (see Table 5).
Cerebral infarction
Five articles [13, 15–18] reported data from all cases with secondary cerebral infarction, whereas 2 references [14, 15] reported data from the CVS cases with cerebral infarction. The meta-analysis results showed that the OR of cerebral infarction for all cases in the fasudil group was only 50% of that of the control group (OR = 0.50, 95% CI: 0.34–0.76, P = 0.0009, P(χ2) = 0.67), whereas the OR of cerebral infarction for CVS cases in the fasudil group was only 43% of that in the control group (OR = 0.43, 95% CI: 0.26–0.70, P = 0.0008, P(χ2) = 0.13; Table 3). The NNT results indicated that, compared with the control group, 1 of every 2 patients in the fasudil group avoided cerebral infarction in all cases, whereas 1 out of every 3 patients in the fasudil group avoided cerebral infarction in CVS cases.
Clinical outcomes
Good outcomes
Five articles [13–16, 18] reported data on patients with good recovery as assessed by GOS for all cases. The meta-analysis results indicated that the good recovery rate for all cases in the fasudil group was 1.58-fold higher than that of the control group (OR = 1.58, 95% CI: 1.12–2.23, P = 0.009, P(χ2) = 0.53). The other 2 articles [14, 15] also reported data on patients with good recovery among the CVS cases. The meta-analysis results indicated that the good recovery rate for CVS cases in the fasudil group was 2.07-fold higher than that of the control group (OR = 2.07, 95% CI: 1.20–3.59, P = 0.009, P(χ2) = 0.35; Table 3). The NNT results showed that, compared with the control group, 1 of every 2 patients in the fasudil group exhibited good recovery among all cases, whereas 1 out of 4 patients displayed good recovery among the CVS cases (see Table 5).
The meta-analysis results based on the GOS scores (for all cases [13–17] and CVS cases [13, 15, 17, 18]) indicated that, compared with the control group under both conditions, the GOS scores of the fasudil group increased by an average of 0.25 points and 0.33 points respectively (all cases: WMD = 0.25, 95% CI: 0.07–0.43, P =0.006, P(χ2) = 0.69; CVS cases: WMD = 0.33, 95% CI: 0.12–0.55, P = 0.002, P(χ2) = 0.48; Table 4). These results suggest that fasudil can significantly improve the clinical outcomes of patients as assessed according to the GOS.
The final 2 articles [13, 21] reported clinical outcome data on the basis of the author’s self-formulated assessment criteria for therapeutic efficacy. The meta-analysis results showed that the number of patients with significant treatment effectiveness in the fasudil group was 2.5 times that of the control group (OR = 2.50, 95% CI: 1.32-–.72, P = 0.005, P(χ2) = 0.73), whereas the difference in the total response rate between the groups was not statistically significant (P > 0.05; Table 3). Compared with the control group, the NNT results indicated that 1 in every 4 patients of the fasudil group showed significant effectiveness (Table 5).
Adverse outcomes
Four articles [13–15, 18] reported data on death, vegetative state, or severe disability through GOS assessment among all cases. The meta-analysis results showed that, compared with the control drug, fasudil slightly decreased the incidence of these adverse outcomes (OR = 0.68, 95% CI: 0.45–1.02, P = 0.06, P(χ2) = 0.64). Two other articles [14, 15] reported data on death, vegetative state, or severe disability in CVS cases. The meta-analysis results showed that, compared with the control drug, fasudil significantly decreased the occurrence of these adverse outcomes (OR = 0.37, 95% CI: 0.18–0.76, P = 0.007, P(χ2) = 0.22; Table 3). The NNT results indicated that, compared with the control group, 1 in every 4 patients in the fasudil group avoided the occurrence of death, vegetative state, or severe disability, both among all cases and among CVS cases (Table 5).
Level of consciousness
Four articles [16–18, 20] reported data on GCS scores 2 weeks after treatment. The meta-analysis results showed that, compared with the control group, the average GCS score of the patients in the fasudil group increased by 0.95 points (WMD = 0.95, 95% CI: 0.67–1.22, P < 0.00001, P(χ2) = 0.41). The GCS scores of the fasudil group increased by an average of 0.79 points upon the exclusion of the low-quality article [20] (WMD = 0.79, 95% CI: 0.37–1.18, P = 0.0002, P(χ2) = 0.43; Table 4). These results showed that, compared with the control group, the consciousness level significantly improved in the patients of the fasudil group.
Blood flow velocity
Two articles [13, 16] reported data on TCD-determined mean blood flow velocity in the middle cerebral artery of the patients 2 weeks after treatment. The meta-analysis results demonstrated that the mean blood flow velocity in the middle cerebral artery of the patients in the fasudil group decreased by 12.14 cm/s compared with the control group (WMD = −12.14, 95% CI: −17.45 to −6.83, P < 0.00001, P(χ2) = 0.51; Table 4).
Adverse responses
Three articles [16, 18, 21] reported data on adverse responses in patients. The meta-analysis showed no significant difference in the incidence rate of adverse responses between the two groups during treatment (P > 0.05). Another article [18] reported the changes in the systolic pressure of the patients before and after treatment. The meta-analysis results showed that, compared with the fasudil group, the systolic pressure decreased by 8.40 mmHg in the nimodipine group 60 min after the treatment (fasudil group/nimodipine group: WMD = 8.40, 95% CI: 0.67–16.13, P = 0.03; Table 3).
Sensitivity analysis
-
1.
With the exclusion of a single low-quality article [20] or an article with a relatively low-quality score [14], the results of repeated meta-analysis showed that all outcome indicators (14 days after the treatment among the angiography-diagnosed CVS cases [15, 17, 18], GCS scores 2 weeks after the treatment [16–18], and symptomatic vasospasm [15, 16, 18]) remained statistically significant (P<0.05; Tables 3, 4).
-
2.
Through analysis of the 18 indicators using the fixed effects model and the random effects model, the overall effectiveness values calculated from the two models were found to be largely consistent with their 95% CI values for all indicators except symptomatic vasospasm [14–16, 18] (the results of a small number of indicators using the random effects model were relatively conservative, and the results of most of the indicators from the two models were identical; Tables 3, 4).
The sensitivity analysis carried out using both methods described above showed that the meta-analysis results of the majority of outcome indicators in this study are robust and reliable with relatively low sensitivity.
Publication bias
The fail-safe number (Nfs) of each outcome indicator is far greater than the number of trials included in the meta-analysis, which suggests that no publication bias exists in the meta-analysis described above (Table 5).
Discussion
The results of this study show the following:
-
1.
Compared with the control drug, fasudil not only greatly reduces the odds ratio of symptomatic vasospasm, but also significantly lowers the odds ratio of angiography-diagnosed CVS in SAH patients.
-
2.
Fasudil significantly reduces the odds ratio of cerebral infarction for all cases and for CVS cases in SAH patients.
-
3.
More importantly, compared with the control drug, fasudil significantly increases the odds ratios of good recovery for all cases and for CVS cases (while significantly improving the GOS scores among all cases and CVS cases), significantly reduces the odds ratio of death, vegetative state, or severe disability among the CVS cases, and exhibits a trend of slightly decreasing the odds ratio of death, vegetative state, or severe disability among all cases.
-
4.
Compared with nimodipine, fasudil significantly increases the GCS scores of patients 2 weeks after treatment.
-
5.
Fasudil significantly reduces the mean blood flow velocity in the middle cerebral artery of patients.
-
6.
Fasudil has similar adverse effects to nimodipine (the analysis of one article [18] indicated that, compared with the fasudil group, the systolic blood pressure in the nimodipine group was significantly reduced 60 min after treatment, and 1 patient withdrew from the trial because of the significantly lowered blood pressure).
The present study used the “Quality of Reporting of Meta-analyses” system formulated by Professor David Moher and others [28] at the University of Ottawa, Canada in 1999 as the standards for the development of research methods and guiding the research process. We not only searched the current major Chinese-language and English-language international electronic databases (with language restrictions removed during the PubMed search process), but also individually reviewed the studies in the reference lists of the articles that met the inclusion criteria of this study to include other studies that might have been missed in the process of the on-line literature search. We strictly assessed the quality and authenticity of the selected studies and also conducted heterogeneity and sensitivity analyses on various outcome indicators. To highlight the therapeutic effects of fasudil on CVS, we conducted stratified analysis on some outcome indicators (for all cases and CVS cases). We calculated the fail-safe number to determine whether there was a publication bias for some outcome indicators to further demonstrate the credibility of the research results. Although the sample sizes of some trials were relatively small, the vast majority of the outcome indicators exhibited good literature homogeneity. In addition, most statistically significant outcome indicators had a narrow 95% CI range, which indicates relatively high credibility of the results. The results from this study showed that the homogeneity of the studies included in this research was relatively high, the meta-analysis results of the majority of the outcome indicators were robust and reliable with low sensitivity, and no publication bias was found in any of the 9 meta-analysis results (outcome indicators of categorized variables) with statistical significance.
The highlight of this study is that, based on the meta-analysis, fasudil was found to not only prevent and reverse CVS in SAH patients, but, most importantly, also significantly improve the clinical outcomes of the patients, as evaluated with the Glasgow Outcome Scale. This effect represents an advantage over endothelin receptor antagonists such as tirilazad, or nicardipine [3–6].
We were unable to obtain detailed data, including the number of surgery patients, surgical timing, surgical approach, and surgical outcome, for each patient in the fasudil and control groups. We did not have access to the clinical-level data of each patient before treatment. In addition, differences in the geographical regions, hospital levels, and the impacts of different basic and combined medications on the clinical outcomes of the patients in each trial were not considered (these factors may affect the results and conclusions of the meta-analysis). Therefore, research bias cannot be completely ruled out in this study. In addition, we could not control for publication bias because of the different diagnostic criteria of symptomatic cerebral vasospasm used by different authors. At the same time, owing to the limited number of trials and samples available for analysis, the conclusions from the present study still need to be further verified through large randomized, controlled clinical trials.
References
Macdonald RL, Higashida RT, Keller E, Mayer SA, Molyneux A, Raabe A, Vajkoczy P, Wanke I, Frey A, Marr A, Roux S, Kassell NF (2010) Preventing vasospasm improves outcome after aneurysmal subarachnoid hemorrhage: rationale and design of CONSCIOUS-2 and CONSCIOUS-3 trials. Neurocrit Care 13:416–424
Dorhout-Mees SM, Rinkel GJ, Feigin VL, Algra A, den Bergh WM v, Vermeulen M, van GJ (2007) Calcium antagonists for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev CD000277
Jang YG, Ilodigwe D, Macdonald RL (2009) Metaanalysis of tirilazad mesylate in patients with aneurysmal subarachnoid hemorrhage. Neurocrit Care 10:141–147
Kramer A, Fletcher J (2009) Do endothelin-receptor antagonists prevent delayed neurological deficits and poor outcomes after aneurysmal subarachnoid hemorrhage?: a meta-analysis. Stroke 40:3403–3406
Wang ZJ, Liu GJ (2011) Protection effect of endothelin receptor antagonist on blood vessel in patients with subarachnoid hemorrhage. China Pharm 22:525–529
Zhang S, Wang L, Liu M, Wu B (2010) Tirilazad for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev 2:CD006778
Zwienenberg-Lee M, Hartman J, Rudisill N, Madden LK, Smith K, Eskridge J, Newell D, Verweij B, Bullock MR, Baker A, Coplin W, Mericle R, Dai J, Rocke D, Muizelaar JP (2008) Effect of prophylactic transluminal balloon angioplasty on cerebral vasospasm and outcome in patients with Fisher grade III subarachnoid hemorrhage: results of a phase II multicenter, randomized, clinical trial. Stroke 39:1759–1765
Treggiari MM, Deem S (2009) Which H is the most important in triple-H therapy for cerebral vasospasm. Curr Opin Crit Care 15:83–86
Lohn M, Plettenburg O, Ivashchenko Y, Kannt A, Hofmeister A, Kadereit D, Schaefer M, Linz W, Kohlmann M, Herbert JM, Janiak P, O’Connor SE, Ruetten H (2009) Pharmacological characterization of SAR407899, a novel rho-kinase inhibitor. Hypertension 54:676–683
Tiftik RN, Erol A, Cnar MG, Kubat H, Ark M, Ulker S, Buyukafsar K (2008) Nitric oxide does not down regulate Rho-kinase (ROCK-2) expression in rat coronary endothelial cells. J Cardiovasc Pharmacol 51:140–147
Yamaguchi S, Tanabe K, Takai S, Matsushima-Nishiwaki R, Adachi S, Iida H, Kozawa O, Dohi S (2009) Involvement of Rho-kinase in tumor necrosis factor-alpha-induced interleukin-6 release from C6 glioma cells. Neurochem Int 55:438–445
Satoh S, Hitomi A, Ikegaki I, Kawasaki K, Nakazono O, Iwasaki M, Mohri M, Asano T (2010) Amelioration of endothelial damage/dysfunction is a possible mechanism for the neuroprotective effects of Rho-kinase inhibitors against ischemic brain damage. Brain Res Bull 81:191–195
Li CH, Ye JY, Du P, Zhang QJ, Zhang GS, Sun GZ, Zhang JF, Li JH, Nie JG (2009) Effective evaluation of combined treatment in delayed cerebrovascular spasm after subarachnoid hemorrhage. J Apoplexy Nerv Dis 26:580–582
Nakashima S, Tabuchi K, Shimokawa S, Fukuyama K, Mineta T, Abe M (1998) Combination therapy of fasudil hydrochloride and ozagrel sodium for cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Neurol Med Chir (Tokyo) 38:805–810; discussion 810–811
Shibuya M, Suzuki Y, Sugita K, Saito I, Sasaki T, Takakura K, Nagata I, Kikuchi H, Takemae T, Hidaka H, Nakashima M (1992) Effect of AT877 on cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Results of a prospective placebo-controlled double-blind trial. J Neurosurg 76:571–577
Ma JJ, Yang SY, Wei W, Yue SY, Zhong Y, Yang WD, Zhang DJ, Zhu SG, Zhu T, Li M, Yang YS, Li M, Shu BH, Zheng GE (2006) A phase clinical evaluation of fasudil hydrochloride for cerebral vasospasm following subarachnoid hemorrhage. Chin J Neurosurg 22:36–40
Tong HY, Yu XG, Xu BN (2002) The effects of a new vasodilator fasudil on delayed cerebral vasospasm after subarachnoid hemorrhage. Acad J PLA Postgrad Med Sch 23:53–56
Zhao JZ, Zhou DB, Guo J, Ren ZY, Zhou LF, Wang S, Xu BN, Wang RZ (2006) Effect of fasudil hydrochloride, a protein kinase inhibitor, on cerebral vasospasm and delayed cerebral ischemic symptoms after aneurysmal subarachnoid hemorrhage. Neurol Med Chir (Tokyo) 46:421–428
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary. Control Clin Trials 17:1–12
Gao GC (2008) Effects of fasudil hydrochloride on cerebral vasospasm following subarachnoid hemorrhage. Chin J Misdiag 8:3844–3845
Ning L, Bo LH, Hong H (2008) Effect of fasodil on cerebral vasospasm in patients with subarachnoid hemorrhage. Chin J Pract Med 35:40–41
Hunt WE, Hess RM (1968) Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg 28:14–20
Hunt WE, Kosnik EJ (1974) Timing and perioperative care in intracranial aneurysm surgery. Clin Neurosurg 21:79–89
Jennett B, Bond MR (1975) Assessment of outcome after severe brain damage. Lancet 305:480–484
Teasdale G, Jennett B (1974) Assessment of coma and impaired consciousness. A practical scale. Lancet 304:81–84
Cao HJ, Liu JP (2010) [Number needed to treat (NNT), an index for clinical therapeutic efficacy assessment–its significance and application]. Chin J Integr Tradit West Med 30:752–756
Rosenthal R (1979) The “file drawer problem” and tolerance for null results. Psychol Bull 86:638–641
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF (1999) Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet 354:1896–1900
Acknowledgements
We are grateful to all the staff of American Journal Experts for language assistance and paper revision.
Conflict of interest
There was no conflict of interest among the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liu, G.J., Wang, Z.J., Wang, Y.F. et al. Systematic assessment and meta-analysis of the efficacy and safety of fasudil in the treatment of cerebral vasospasm in patients with subarachnoid hemorrhage. Eur J Clin Pharmacol 68, 131–139 (2012). https://doi.org/10.1007/s00228-011-1100-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-011-1100-x