
Abstract
Background
Sepsis is common in neonates and is a major cause of morbidity and mortality. Sixty percent of preterm neonates receive at least one antibiotic, and 43% of the antibiotics administered to these neonates are aminoglycosides. The clearance (Cl), serum half-life (t1/2), and volume of distribution (Vd) of aminoglycosides change during the neonatal life, and the pharmacokinetics of aminoglycosides need to be studied in neonates in order to optimise therapy with these drugs.
Objective
The aim of this work is to review the published data on the pharmacokinetics of aminoglycosides in order to provide a critical analysis of the literature that can be a useful tool in the hands of physicians.
Methods
The bibliographic search was performed electronically using PubMed, as the search engine, through July 11th, 2008. Firstly, a Medline search was performed with the keywords “pharmacokinetics of aminoglycosides in neonates” with the limit of “human”. Other Medline searches were performed with the keywords “pharmacokinetics of … in neonates” followed by the name of the aminoglycosides: amikacin, gentamicin, netilmicin and tobramycin. In addition, the book Neofax: A Manual of Drugs Used in Neonatal Care by Young and Mangum (Thomson Healthcare, 2007) was consulted.
Results
The aminoglycosides are mainly eliminated by the kidney, and their elimination rates are reduced at birth. As a consequence Cl is reduced and t1/2 is prolonged in the neonate as compared to more mature infants. The high body-water content of the neonate results in a large Vd of aminoglycosides as these drugs are fairly water soluble. Postnatal development is an important factor in the maturation of the neonate, and as postnatal age proceeds, Cl of aminoglycosides increases.
Conclusion
The maturation of the kidney governs the pharmacokinetics of aminoglycosides in the infant. Cl and t1/2 are influenced by development, and this must be taken into consideration when planning a dosage regimen with aminoglycosides in the neonate. Aminoglycosides are fairly water soluble, and the larger water content of neonates yields a larger Vd in these patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Aminoglycosides are used for the treatment of neonates with suspected or proven Gram-negative bacterial infection, which is potentially life-threatening in neonates. Aminoglycosides are administered in association with a penicillin such as ampicillin or amoxicillin [1]. Penicillins increase bacterial permeability to aminoglycosides [2]. An evaluation of the use of antibiotics revealed that 60% of neonates receive at least one antibiotic during the first week of life, of which aminoglycosides represent 43% [3].
The high morbidity and mortality of bacterial infections in neonates require that the antibiotic therapy should be started as soon as the infection is suspected [4]. The remarkable interindividual variability in the pharmacokinetics of aminoglycosides requires that their optimum dosing be defined.
The aminoglycosides have a low therapeutic index [5] and thus knowledge about their pharmacokinetics is essential. The main pharmacokinetic parameters are clearance (Cl), serum half-life (t1/2), volume of distribution (Vd), and the area under the concentration time curve (AUC). The pharmacokinetics of aminoglycosides are different in neonates than in adults [6], and it is thus necessary to study the pharmacokinetics of these drugs in neonates. In neonates there is a marked interindividual variability in aminoglycoside pharmacokinetic parameters (see the “Discussion” section), and it is necessary to identify the main causes of variability.
Over the past few decades, it has become common to apply pharmacokinetic principles when designing drug regimens. This applies also to neonatology where biological functions rapidly change during development. The main pharmacokinetic parameters, t1/2, Cl and Vd, have been collected and organised into this article for gentamicin, netilmicin, tobramycin and amikacin. Therapy with aminoglycosides also requires knowing their peak and trough concentrations, and these two parameters have been collected.
The aminoglycosides have similar uses, and under particular circumstances, have similar minimum inhibitory concentrations (MIC). Escherichia coli is often found in neonatal infections and MIC90 are 0.25 μg/ml (netilmicin), 0.5 μg/ml (gentamicin and tobramycin) and 1 μg/ml (amikacin) [5].
This work aimed to review the kinetic parameters of gentamicin, netilmicin, tobramycin and amikacin in the neonate in order to provide a tool that may be useful in the hands of physicians.
Bibliographic search
The bibliographic search was performed electronically using PubMed as the search engine, through July 11th, 2008. Firstly, a Medline search was performed with the keywords “pharmacokinetics of aminoglycosides in neonates” with the limit of “human”. Other Medline searches were performed with the keywords “Pharmacokinetics of … in neonates” followed by the names of the aminoglycosides: amikacin, gentamicin, netilmicin and tobramycin. In addition, the book Neofax: A Manual of Drugs Used in Neonatal Care by Young and Mangum [7] was consulted. The bibliographic search gave rise to 60 original articles, 2 review articles and 3 book chapters. The publication years of this matter ranged from 1962 to 2007.
Results
The demographic data of the neonates and the pharmacokinetic parameters are collected in four tables. The information about gentamicin is summarised in Table 1. Table 2 shows the data relative to netilmicin. Table 3 summarises the information relative to tobramycin, and Table 4 shows the pharmacokinetic parameters of amikacin.
Cl is expressed in different units by different authors. This makes the comparison between studies difficult. To overcome this difficulty we have converted Cl into milliliters per minute per kilogram which is the unit adopted by Thummel et al. [6], and it makes the comparison with the adult values easy. Standard deviation (SD) cannot be converted and therefore Cl is shown without SD.
Gentamicin
A great part of the information on aminoglycoside pharmacokinetics deals with gentamicin. Aminoglycosides are toxic for the eighth cranial nerve [5, 8] and for the kidney [5, 9]. This requires that the concentration of aminoglycosides be within the appropriate interval. Gentamicin trough concentration >2 μg/ml is associated with toxicity [5, 10], and peak concentration <5 μg/ml is associated with lesser efficacy [5, 11] as gentamicin, as well as the other aminoglycosides, exhibits a concentration-dependent bactericidal effect [5]. Formerly, gentamicin was administered at a dose of 2.5 mg/kg every 12 h [12]. Later, it appeared that once-daily gentamicin dosing of 4-5 mg/kg yields higher peak and lower trough gentamicin concentration than twice-daily dosing [13–16] (for review see Rao et al. [17] and Miron [18]). Recently, administering 5 mg/kg gentamicin and extending the dosing interval to 36-48 h has been recommended [19–22]. Extending the dosing interval to 48 h while increasing the gentamicin dose to 5 mg/kg causes an increase in peak concentration and a decrease in trough concentration as compared with a dose of 2.5 mg/kg every 12 h [20, 22, 23].
The extended-interval method of aminoglycosides has been used in 75% of U.S. hospitals since 2002 [24, 25]. Young and Mangum [7] suggest a gentamicin dose of 5 mg/kg every 48 h during the first week of life, when the gestational age is ≤29 weeks, a dose of 4.5 mg/kg every 36 h, during the first week of life, when the gestational age is 30 to 34 weeks and a daily dose of 4 mg/kg when the gestational age is ≥35 weeks. Using these dosing rates, gentamicin peak and trough concentrations should be <12 and <2 μg/ml respectively. Lanao et al. [21] administered 10 mg/kg gentamicin every 36-48 h, and this dosage appeared to be appropriate to obtain the peak concentration of 15-20 μg/ml and the trough concentration <0.5 μg/ml.
Some authors suggested using a loading dose of 4-5 mg/kg to shorten the time between the first dose of gentamicin and the time when gentamicin therapeutic serum concentration is reached [26–29]. The introduction of once-daily dosing and the extended interval between dose regimens, which require 4-5 mg/kg of gentamicin, makes the use of the loading dose unnecessary.
Table 1 summarises the kinetic parameters of gentamicin and shows that t1/2 ranged from 4.9 to 14.6 h, Cl ranged from 0.53 to 1.72 ml min−1 kg−1 and Vd ranged from 0.45 to 0.75 l/kg.
This variability observed for gentamicin, as well as the other aminoglycosides, requires that therapy with these drugs be individualised, especially for critical patients such as premature infants.
Netilmicin
Once-daily dosing of netilmicin was reported by Gosden et al. [30] and Brooks et al. [31]. These authors administered 4-4.5 mg/kg netilmicin and obtained peak and trough concentrations within the expected values. Ettingler et al. [32] administered 6 mg/kg netilmicin, and the trough concentrations were >2 μg/ml in one-third of the cohort. Consistent results were obtained by Klingenberg et al. [33], who administered 6 mg/kg netilmicin every 24 or 36 h. In this study, the trough concentration exceeded 2 μg/ml in 43% of the patients, and these authors suggest a dosing interval of 48 h for gestational age <29 weeks, 36 h for gestational age of 29-36 weeks and 24 h for full-term infants. Interestingly, in full-term infants and in infants with postnatal age >7 days, the percentages of neonates with a trough concentration >2 μg/ml were 15 and 6% respectively suggesting that gestational age and postnatal development influence the trough concentration of netilmicin. Young and Mangum [7] suggest a dosage of netilmicin similar to that of gentamicin given above. With this dosage, the peak concentration of netilmicin should be 5–12 μg/ml and the trough concentration should be <2 μg/ml.
When netilmicin was administered twice-daily at the dose of 2.5 mg/kg every 12 h, the average trough concentration was 2.8 μg/ml [34], and similar results were obtained by Granati et al. [35]. This suggests that the once-daily dose of 4 mg/kg [31] or 4.5 mg/kg [30] is safer than the twice-daily dose.
Siegel et al. [36] administered 3 or 4 mg/kg netilmicin once daily to premature and full-term neonates and obtained average trough concentrations ranging from 2.3 to 3.5 μg/ml. It must be noted that the trough concentrations were measured 6 h after dosing.
The loading dose of netilmicin was introduced by Berger et al. [37] and Rengelshausen et al. [38]. For dosing details see Table 2. The literature on aminoglycosides reveals that the loading-dose regimen is overcome by once daily and extended-interval dosing regimes.
Table 2 shows that t1/2 ranged from 3.4 to 18.2 h, Cl ranged from 0.45 to 1.37 ml min−1 kg−1 and Vd ranged from 0.34 to 0.88 l/kg.
Tobramycin
Little is known about tobramycin pharmacokinetics in the neonate. In an early study, de Hoog et al. [39] modified both the tobramycin dose and the interval between doses according to the neonate age. The tobramycin dosing schedule was 3.5 mg/kg every 24 h (≤28 weeks), then 2.5 mg/kg every 18 h (28-36 weeks) and 2.5 mg/kg every 18 h (≥36 weeks). Using this schedule, the percentage of trough concentrations >2 μg/ml ranged from 19 to 49%. In a successive study, de Hoog et al. [40] administered 4 mg/kg tobramycin to all patients and the interval between doses was 48 h (<32 weeks), 36 h (32-36 weeks) and 24 h (≥37 weeks). Using these dosages, the majority of infants had tobramycin peak concentrations from 5 to 10 μg/ml and trough concentrations from 0.5 to 1 μg/ml. The elimination rate constant (Ke) was 0.064 ± 0.034 and 0.098 ± 0.046 h-1 at gestational ages <32 and ≥37 weeks respectively; and Vd was 0.70 ± 0.17 and 0.54 ± 11 l/kg at the gestational ages of <32 and ≥37 weeks respectively [40]. The difference in Cl reflects the reduced clearance of tobramycin in preterm neonates [41–43]. The difference in Vd is primarily attributable to a higher percentage of body water in premature infants resulting in a higher Vd as tobramycin is fairly water soluble [41–43].
Young and Mangum [7] suggest a dose of tobramycin similar to that of gentamicin given above. Ke and Vd of tobramycin were measured in 470 neonates by nonlinear mixed effects model (NONMEM) and by nonparametric expectation maximization (NPEM2) [44]. Population estimates and variation coefficients (CV%) for optimal models were Ke 0.071 h-1 (27%) and Vd 0.59 l/kg (9%) (NONMEM) and Ke 0.079 h-1 (42%), Vd 0.65 (48%) (NPEM2). NONMEM showed less bias (P < 0.05) than NPEM2. These data are in agreement with those by Nahata et al. [42, 45] (see Table 3).
Table 3 summarises the kinetic parameters of tobramycin and shows that t1/2 ranged from 4.4 to 9.9 h, Cl ranged from 0.69 to 1.19 ml min−1 kg−1 and Vd ranged from 0.49 to 0.94 l/kg.
Amikacin
The literature on the pharmacokinetics of amikacin in the neonate is sparse and scanty. A study on the extended interval between doses is lacking. Langhendries et al. [46] suggest administrating amikacin to neonates once daily. These authors compared peak and trough concentrations of amikacin after once-daily and twice-daily dosing. The peak concentration was 23.1 ± 3.3 μg/ml (once daily, 15 mg/kg) and 13.6 ± 3.2 μg/ml (twice-daily, 7.5 mg/kg every 12 h) (P < 0.001). Conversely, the trough concentration was not different with two dosages. Young and Mangum [7] suggest an amikacin dose of 18 mg/kg every 48 h during the first week of life when the gestational age was ≤29 weeks; a dose of 18 mg/kg every 36 h during the first week of life when the gestational age was 30–34 weeks; and a daily dose of 15 mg/kg when the gestational age was ≥35 weeks.
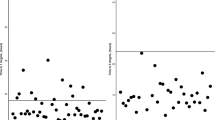
Tréluyer et al. [47] studied the population pharmacokinetics of amikacin in neonates, infants and children, and the kinetics parameters are an average of all cases. There was a remarkable interindividual variability. Cl ranged from 0.16 to 4.16 ml min−1 kg−1, and t1/2 ranged from 0.59 to 21.8 h. The plot of Cl versus postnatal age shows that Cl increased up to 20 months of age and then reached a plateau up to at least 80 months. Vd showed an opposite trend; the highest values were found in neonates and then Vd decayed up to 80 months of age. A remarkable interindividual variability in Cl was also observed in extremely premature neonates [48].
Assael et al. [49] studied the effect of intrauterine maturation on the pharmacokinetics of amikacin in 29 neonates whose gestational age and body weight ranged between 28 and 42 weeks and 0.9 and 4.5 kg respectively. The patients received a daily dose of 7.2 mg/kg amikacin. The trough concentration inversely correlated with the gestational age (R = -0.56) and neonates with gestational age <34 weeks showed significantly higher accumulation of amikacin. The pharmacokinetic parameters of amikacin are shown in Table 4.
Table 4 shows that t1/2 ranged from 3.0 to 16.4 h, Cl ranged from 0.36 to 1.71 ml min−1 kg−1 and Vd ranged from 0.34 to 0.72 l/kg.
Discussion
There is a remarkable variation in the pharmacokinetic parameters of gentamicin [21, 50], netilmicin [30–32, 38], tobramycin [39, 40] and amikacin [51, 52]. Such a variation is due to renal maturation [50] as aminoglycosides are fairly water soluble and are eliminated with the urine. There is a correlation (R = 99) between gentamicin Cl and creatinine Cl [53], and gentamicin t1/2 correlates (R = 0.78) with plasma creatinine concentration [54]. The variability in t1/2 and Cl of gentamicin could be due to variability in the glomerular filtration rate [54]. Another source of variability is the gestational age [52]. Other factors generating variability are malnutrition, disease, developmental stage or genetics. These factors can coexist, and it is difficult to divide them between different factors. Monitoring aminoglycoside serum concentration is necessary, especially in critical patients such as the premature infant.
The dose of aminoglycosides and the interval between doses have been changed in neonates during recent years. Increasing the gentamicin dose to 4-5 mg/kg and administering it once daily has been suggested [14–16]. This dose yields peak and trough concentrations which are 5–12 and <2 μg/ml respectively. Additionally, increasing the gentamicin dose to 5 mg/kg and extending the interval between doses to 24-48 h depending on the gestational age has been suggested [19-22]. The extended interval between doses yields peak values of gentamicin between 5 and 12 μg/ml and trough concentrations <2 μg/ml respectively, which are the expected values. Another advantage of the extended interval is to reduce the number of administrations with consequent reduction in the cost of monitoring. Pharmacokinetic parameters such as Vd and Cl are not modified in the extended time interval. The extended interval is also reported for netilmicin [33] and tobramycin [40].
The pharmacokinetic rationale for increasing the gentamicin dose and extending the interval between doses is related to the pharmacokinetics of gentamicin. This drug has a long t1/2 and a large Vd, especially in premature infants [21]. The same applies to the other aminoglycosides. The peak concentration is determined by the dose and Vd. When the gentamicin Vd is large, as in premature infants, a dose of 5 mg/kg is correct [7]. At sepsis, Vd of gentamicin increases. The trough concentration is determined by the interval between doses and by t1/2. The trough concentration is modified by disease and malnutrition. The once-daily regimen and the extended interval between dose regimens yield trough concentrations <2 μg/ml.
The MIC90 of Escherichia coli and Klebsiella pneumoniae, which are often found in cases of newborn infection, is 0.5 μg/ml for gentamicin [5]; and assuming a peak-to-MIC90 ratio above 10, a peak gentamicin serum concentration of 5-12 μg/ml is appropriate to eradicate the infection.
Netilmicin Cl measured in infants with gestational age >36 weeks is double that measured in neonates with gestational age <34 weeks [30], indicating that the dose of netilmicin must be modified according to the developmental stage. The MIC90 of Escherichia coli and Klebsiella pneumoniae is 0.25 μg/ml for netilmicin [5]; and assuming a peak-to-MIC90 ratio above 10, a peak netilmicin serum concentration of 2.5 μg/ml is desirable. However it is opportune to have a netilmicin serum concentration of 5-12 μg/ml. The trough concentration obtained with 6 μg/ml every 36 h [33] is lower than that obtained after 2.5 mg/kg twice daily [34] and with 2 mg/kg thrice daily [55]. This suggests that the extended-interval dosing regimen is safer than fractioning the dose of netilmicin during the day. Using the therapeutic schedule given by Young and Mangum [7], peak concentration should range from 5 to 12 μg/ml.
Tobramycin MIC90 values for Escherichia coli and for Klebsiella pneumoniae are 0.5 and 1 μg/ml respectively [5]; and assuming a peak-to-MIC90 ratio above 10, a peak tobramycin serum concentration higher than 10 μg/ml should be desirable [40]. What has been stated for gentamicin holds true for tobramycin as well: t1/2 is greater in the premature than full-term neonate and the opposite is true for Cl [39].
The peak concentration of amikacin is 26 μg/ml in the adult [6] and is five-fold higher than that of gentamicin [5]. The therapeutic schedule of amikacin differs in different studies. According to the schedule by Young and Mangum [7], peak concentration should be >40 μg/ml and trough concentration should be <6 μg/ml. Amikacin MIC90 value for Escherichia coli and Klebsiella pneumoniae is 1 μg/ml [5], and assuming a peak-to-MIC90 ratio above 10, a peak tobramycin serum concentration higher than 10 μg/ml should be appropriate.
The scenario of the aminoglycoside pharmacokinetics in the neonate is complex. Aminoglycosides are mainly eliminated by the kidney and the glomerular filtration rate is lower in the premature than full-term neonate [53], and creatinine Cl correlates with gentamicin Cl [54]. The kinetic parameters of individual aminoglycosides differ among neonates, and the gestational age is an important factor determining variability [51]. Monitoring aminoglycoside serum concentration is important in neonates [56] and in particular in critical patients such as premature infants.
References
Hickey SM, McCracken G Jr (1997) Postnatal bacterial infections. In: Fanaroff AA, Martin RJ (eds) Neonatal-perinatal medicine: diseases of the fetus and infant, 6th ed. Mosby, St Louis, pp 717–731
Plotz PH, Davis BD (1962) Synergy between streptomycin and penicillin: a proposed mechanism. Science 135:1067–1068
Bonati M (1988) Early neonatal drug utilisation in preterm newborns in neonatal intensive care units: Italian Collaborative Group on Preterm Delivery. Dev Pharm Ther 11:1–7
Edwards MS (1997) Antibacterial therapy in pregnancy and neonates. Clin Perinatol 24:59–70
Chambers HF (2006) The aminoglycosides. In: Brunton LL, Lazo JS, Parker KL (eds.) Goodman & Gilman’s the pharmacologic basis of therapeutics, 11th ed. McGraw Hill, New York, pp 1155–1171
Thummel KE, Shen DD, Isoherranen N, Smit HE (2006) Design and optimization of dosage regimens: pharmacokinetic data. In: Brunton LL, Lazo JS, Parker KL (eds.) Goodman & Gilman’s the pharmacologic basis of therapeutics, 11th ed. McGraw Hill, New York, pp 1787–1888
Young TE, Mangum B (2007) The antibiotics. Neofax: a manual of drugs used in neonatal care, 20th ed. Thomson Healthcare, Montvale, NJ, USA, pp 2-77
Matz GJ (1993) Aminoglycoside cochlear ototoxicity. Otoryngol Clin North Am 5:705–712
Andronikou S, Giapros VI, Cholevas VI, Popadopoulou ZL (1996) Effect of aminoglycosides therapy on renal function in fullterm infants. Pediatr Nephrol 10:766–768
Swan SK (1997) Aminoglycoside nephrotoxicity. Semin Nephrol 17:27–33
Kovarik JM, Hoepelman IM, Verhoef J (1989) Once-daily aminoglycoside administration: new strategies for old drug. Eur J Clin Microb Infect Dis 8:764–769
Hindmarsh KW, Nation RL, Williams GL, John E, French JN (1983) Pharmacokinetics of gentamicin in very low birth weight preterm infants. Eur J Clin Pharmacol 24:649–953
Krishnan L, George SA (1977) Gentamicin therapy in preterms: a comparison of two dosage regimens. Indian Pediatr 34:1075–1080
de Alba Romero C, Gomez Castillo E, Manzanares Secades C, Rodriguez Lopez J, Arreaza Lopez J, Saenz Valiente P (1998) Once-daily gentamicin dosing in neonates. Pediatr Infect Dis J 17:1169–1171
Agarwal G, Rastogi A, Pyati S, Wilks A, Pildes RS (2002) Comparison of once-daily versus twice-daily gentamicin dosing regimens in infant ≥2500 g. J Perinatol 22:268–274
Thureen PJ, Reiter PD, Gresores A, Stolpman NM, Kawato K, Hall DM (1999) Once- versus twice-daily gentamicin dosing in neonates ≥34 weeks’s gestation: cost-effectiveness analyses. Pediatrics 103:594–598
Rao EM, Ahmed M, Hagan R (2006) One dose per day compared to multiple doses per day of gentamicin for treatment of suspected or proven sepsis in neonates. Cochrane Database Syst Rev 25:CD005091
Miron D (2001) Once daily dosing of gentamicin in infants and children. Pediatr Infect Dis J 20:1169–1173
Rastogi A, Agarwal G, Pyati S, Pilles R (2002) Comparison of two gentamicin dosing schedules in very low birth weight infants. Pediatr Infect Dis J 21:234–240
Avent ML, Kinney JS, Istre GR, Whitfield JM (2002) Gentamicin and tobramycin in neonates: comparison of a new extended dosing interval regimen with a traditional multiple daily dosing regimen. Am J Perinatol 19:413–419
Lanao JM, Calvo MV, Mesa JA, Martin-Suarez A, Carbajosa MT, Miguelez F, Dominguex-Gill A (2004) Pharmacokinetic basis for the use of extended interval dosage regimens of gentamicin in neonates. J Antimicrob Chemother 54:193–198
Mercado MCK, Brodsky NL, McGuire MK, Hurt H (2004) Extended interval dosing of gentamicin in preterm infants. Am J Perinatol 21:73–77
Darmastads GL, Hossain MM, Jana AK, Saha SK, Choi Y, Sridhar S, Thomas N, Miller-bell M, Edwards D, Aranda J, Willis J, Coffey P (2007) Determination of extended-interval gentamicin dosing for neonatal patients in developing countries. Pediatr Infect Dis J 26:501–507
Chuck SK, Raber SR, Rodvold KA, Areff D (2000) National survey of extended-interval aminoglycoside dosing. Clin Infect Dis 30:433–439
Maglio D, Nightingale CH, Nicolau DP (2002) Extended interval aminoglycoside dosing: from concept to clinic. Int J Antimicrob Agents 19:341–348
Semckuk WM, Shevchuk YM, Sankaran K, Wallace SM (1995) Prospective, randomized, controlled evaluation of a gentamicin loading dose in neonates. Biol Neonate 67:13–20
Wattenberg KL, Kelly HW, Angelus P, Backstrom C (1989) The need for a loading dose of gentamicin in neonates. Ther Drug Monit 11:16–20
Iseman BT, Kotagal UR, Mashni SM, Luckhaupt EJ, Johnson CJ (1996) Optimal gentamicin therapy in preterm neonates includes loading doses and early monitoring. Ther Drug Monit 18:549–555
Gal P, Ransom L, Weaver RL (1990) Gentamicin in neonates: the need for loading doses. Am J Perinatol 7:254–257
Gosden PE, Bedford KA, Dixon JJ, Speidel BD, Leaf AA Macgowan (2001) Pharmacokinetics of once-a-day netilmicin [4.5 mg/kg] in neonates. J Chemother 13:270–276
Brooks JR, Marlow N, Reeves BC, Millar MR (2004) Use of once-daily netilmicin to treat infants with suspected sepsis in a neonatal intensive care unit. Biol Neonate 86:170–175
Ettlinger JJ, Bedford KA, Lovering AM, Reeves DS, Speidel BD, MacGowan AP (1996) Pharmacokinetics of once-a-day netilmicin [6 mg/kg] in neonates. J Antimicrob Chemother 38:499–505
Klingenberg C, Smabrekke L, lier T, Flaegstad T (2004) Validation of a simplified netilmicin dosage regimen in infants. Scand J Infect Dis 36:474–479
Kuhn RJ, Nahata MC, Powell DA, Bickers RG (1986) Pharmacokinetics of netilmicin in premature infants. Eur J Clin Pharmacol 29:635–637
Granati A, Assael BM, Chung M, Montini C, Parini R, Pallazzon P, Gagliardi L, Radwanski E, Rubaltelli FF (1985) Clinical pharmacology of netilmicin in preterm and term newborn infants. J Pediatr 106:664–669
Siegel JD, McCracken GH, Thomas ML, Threlkeld N (1979) Pharmacokinetic properties of netilmicin in newborn infants. Antimicrob Agents Chemother 15:246–253
Berger B, Kretzer V, Gludovatz P, Rohrmeister K, Prusa AR, Kohlhauser C (2003) Evaluation of a netilmicin-loading dose in very low birth-weight infants. Biol Neonate 83:25–29
Rengelshausen J, Beeden A, Tsamouranis K, Mokus G, Walter-sack I, Haefeli WE, Linderkamp O (2006) Pharmacokinetics of a netilmicin loading dose on the first postnatal day in preterm neonates with very low gestational age. Eur J Clin Pharmacol 62:773–777
de Hoog M, Schoemaker RC, Mouton JW, van den Anker JN (1997) Tobramycin population pharmacokinetics in neonates. Clin Pharmacol Ther 62:392–399
de Hoog M, Mouton JW, Schormaker RC, Verduin CM, van den Anker JN (2002) Extended-interval dosing of tobramycin in neonates: implications for therapeutic drug monitoring. Clin Pharmacol Ther 71:349–58
Keyes PS, Johnson CK, Rawlins TD (1989) Predictors of trough serum gentamicin concentrations in neonates. Am J Dis Child 143:1419–1423
Nahata MC, Durrel DE, Miller MA (1986) Tobramycin pharmacokinetics in premature identical twins during newborn period. Dev Pharmacol Ther 9:178–182
Skopnik H, Wallraf R, Nies A, Troster K, Heimann G (1992) Pharmacokinetics and antibacterial activity of daily gentamicin. Arch Dis Child 67:57–71
de Hoog M, Schoemaker RC, van den Anker JN, Vinks AA (2002b) NONMEM and NPEM2 population modeling: a comparison using tobramycin data in neonates. Ther Drug Monit 24:359–365
Nahata MC, Powel DA, Durrel DE, Miller MA (1986) Tobramycin pharmacokinetics in very low birth weight infants. Br J Clin Pharmacol 21:325–327
Langhendries JP, Battisti O, Bertrand JM, Francois A, Darmiont J, Ibrahim S, Tulkens PM, Bernard A, Buchet JP, Scalais E (1993) Once-a-day administration of amikacin in neonates: assessment of nephrotoxicity and ototoxicity. Dev Pharmacol Ther 30:220–230
Tréluyer JM, Merlé Y, Tonnelier S, Rey E, Pons G (2002) Nonparametric population pharmacokinetic analysis of amikacin in neonates, infants and children. Antimicrob Agents Chemother 46:1381–1387
Allegaert K, Anderson BJ, Cossey V, Holford NHG (2005) Limited predictability of amikacin clearance in extreme premature neonates at birth. Br J Clin Pharmacol 61:39–48
Assael BM, Parini R, Rusconi F, Cavanna G (1982) Influence of intrauterine maturation on the pharmacokinetics of amikacin in the neonatal period. Pediat Res 16:810–815
Izquierdo M, Lanao JM, Cervero L, Jimenez NV, Dominguez-Gil A (1992) Population pharmacokinetics of gentamicin in premature infants. Ther Drug Monitor 14:177–183
Bleyzac N, Varnier V, Labaune JM, Corvasier S, Maire P, Jelliffe RW, Putet G, Aulagner G (2001) Population pharmacokinetics of amikacin at birth and interindividual variability in renal maturation. Eur J Clin Pharmacol 57:499–504
Padovani EM, Pistolesi C, Fanos V, Messori A, Martini N (1993) Pharmacokinetics of amikacin in neonates. Dev Pharmacol Ther 20:167–173
Kildoo C, Modanlou HD, Komatsu G, Harralson A (1984) Development pattern of gentamicin kinetics in very low birth weight sick infants. Dev Pharmacol Ther 7:345–356
Brion LP, Fleishchman AR, Schwartz GJ (1991) Gentamicin interval in newborn infants as determined by renal function and postconceptional age. Pediatr Nephrol 5:675–678
Viganò A, Principi N, Brivio L, Tommasi P, Stasi P, Dalla Villa A (1992) Comparison of 5 milligrams of netilmicin per kilogram of body weight versus 2 milligrams per kilogram thrice daily for treatment of Gram-negative pyelonephritis in children. Antimicrob Agents Chemother 36:1499–1503
Testa M, Fanos V, Martinelli V, Strognati M, Mussap P, Del Zompo M (2007) Therapeutic drug monitoring of gentamicin in neonatal intensive care unit: experience in 68 newborns. Chemother 19(Suppl 2):39–41
Di Cenzo R, Forrest A, Slish JC, Cole C, Guillet R (2003) A gentamicin pharmacokinetic population model and once-daily dosing algoritm for neonates. Pharmacotherapy 32:585–591
Murphy JE, Austin ML, Frye RF (1998) Evaluation of gentamicin pharmacokinetics and dosing protocols in 195 neonates. Am J Health-Syst Pharm 55:2280–2288
Vervelde ML, Rademarker CMA, Krediet TG, Fleer A, Asten PV, van Dijk A (1999) Population pharmacokinetics of gentamicin in preterm neonates: evaluation of a once-daily dosage regimen. Ther Drug Monitor 21:541–519
Tréluyer JM, Merlé Y, Semlali A, Pons G (2000) Population pharmacokinetic analysis of netilmicin in neonates and infants with use of a nonparametric method. Clin Pharmacol Ther 67:600–609
Yoshioka H, Takimoto M, Fujita K, Maruyama S (1979) Pharmacokinetics of tobramycin in the newborn. Infection 7:180–182
Sardemann H, Colding H, Hendel J, Kampmann JP, Hvidberg EF, Vejisgaard R (1976) Kinetics and dose calculations of amikacin in the newborn. Clin Pharmacol Ther 20:59–66
Kenyon CF, Knoppert DC, Lee SK, Wandenberghe HM, Chance GW (1990) Amikacin pharmacokinetics and suggested dosage modifications for preterm infant. Antimicrob Agents Chemother 34:265–268
Wang J, Liang W-Q, Wu J-J, Pan C-M (2000) Population pharmacokinetics analysis of amikacin and validation on neonates using Monte Carlo method. Acta Pharmacol Sin 21:954–960
Allegaert K, Cossey V, Langhendries JP, Nauleers G, Vanhole C, Devlieger H, Van Overmeire A (2004) Effects of co-administration of ibuprofen-lysine on the pharmacokinetics of amikacin in preterm infants during the first days of life. Biol Neonate 86:207–211
Acknowledgements
This work has been supported by the Ministry of the University and Scientific and Technological Research (Rome, Italy).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pacifici, G.M. Clinical pharmacokinetics of aminoglycosides in the neonate: a review. Eur J Clin Pharmacol 65, 419–427 (2009). https://doi.org/10.1007/s00228-008-0599-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-008-0599-y