
Abstract
Background
Antihypertensive agents are among the most used therapeutic classes. The approach to the pharmacological treatment of hypertension is guided by international recommendations and adherence to treatment is known to result in effective prevention of cardiovascular risk.
Aim
The aim of this study was to evaluate the pattern of use of antihypertensive agents in general practice in terms of drug choice for the initial treatment of hypertension and adherence to treatments among newly recruited patients.
Methods
We collected the data of all antihypertensive drugs prescribed by general practitioners (GPs) and reimbursed between January 1998 and December 2002 by a Local Health Authority of Emilia Romagna (Ravenna district, 350,000 inhabitants). We selected subjects aged 40 years and older, permanently living in the area during the whole period of the study, who received their first prescription of antihypertensives between January and December 1999, with no prescription of antihypertensive agents in the previous year. For each patient, we documented the starting regimen and evaluated adherence to treatment in terms of persistence during the years (patients were defined persistent if they received at least one prescription per year) and in terms of daily coverage (patients were defined covered if they received an amount of drugs consistent with a daily treatment). Finally, switches or addition of other therapeutic classes during the 3-year period were identified.
Results
A cohort of 6,043 subjects receiving their first antihypertensive treatment in 1999 was obtained. Regarding the starting regimen, monotherapies with angiotensin converting enzyme inhibitors (n=1,597; 26%) or calcium channel blockers (n=1126; 19%) were the most frequently prescribed. Of the patients, 21% started with a drug combination regimen. Regarding adherence to treatment, 18% of the cohort received only one prescription throughout the 3 years, 13% received more than one prescription but stopped the therapy during the first year, 69% were persistent during the second year and 60% also during the third year. Only 34% were covered during the first year and 24% also during the second year, whereas only 20% of the patients resulted covered throughout the 3 years. Among persistent patients, 41% maintained the same antihypertensive regimen throughout the 3 years, 25% added other drugs to the initial treatment and 34% switched to completely different regimens.
Conclusions
Our findings reflect the lack of convergence among guidelines on the drug class(es) to be considered as first choice in the initial treatment of hypertension. Although an intervention in this field may have important implications in terms of cost savings, the ongoing debate does not allow us to draw definite conclusions on whether measures should be taken by the National Health Authority. However, the lack of adherence to antihypertensive treatment is undoubtedly a matter of concern for public health and should be addressed with appropriate interventions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Antihypertensive agents are among the most used therapeutic classes: in Italy they represented 35% of overall drug prescription in 2003 [1]. The approach to the pharmacological treatment of hypertension is guided by international recommendations, and adherence to treatment is known to result in effective prevention of cardiovascular risk [2–8].
Although many drug classes are effective in the prevention of cardiovascular events [i.e. β-blockers, diuretics, calcium channel blockers, angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs)], guidelines differ with regard to which drug class is to be considered as first choice for the initial treatment of hypertension in patients with no complications. For these patients, who are mostly treated by general practitioners (GPs), US recommendations [9, 10] consider minor diuretics and β-blockers as first choice, on the basis of clinical experience with these drugs and their low cost. However, European guidelines [11] do not indicate a class of first choice. Finally, a recent British guideline [12] recommended ACE inhibitors or ARBs for young people and calcium channel blockers or minor diuretics for patients aged 55 years and older.
In clinical practice, poor compliance, intermittent treatment and discontinuation of use are frequent causes of inadequate control of blood pressure [13, 14]. Suboptimal treatment can cause progression of coronary atherosclerosis, congestive heart failure and renal disease as well as considerably higher rates of major cardiovascular events [15, 16]. Thus, improved compliance may produce favourable therapeutic effects, and studies evaluating the pattern of use of cardiovascular drugs in real clinical practice may help to identify the determinants of misuse or underuse of antihypertensive agents.
The aim of this study was to evaluate the pattern of use of antihypertensive agents in general practice in terms of drug choice for the initial treatment of hypertension and adherence to treatments among these newly recruited patients.
Methods
Data collection
Antihypertensive prescription data were retrieved from the Emilia Romagna Regional Health Authority Database [17]. This database provides the following information for each reimbursed prescription: identification number of the dispensed product, Anatomical Therapeutic Chemical (ATC) code, number of packages and number of defined daily doses (DDDs) dispensed [18], code of the patient and date of prescription. The patient code allows the retrieval of each individual’s drug history without their identification.
We collected the data of all antihypertensive drugs prescribed by GPs and reimbursed between January 1998 and December 2002 by a Local Health Authority of Emilia Romagna (Ravenna district, with both urban and rural area, counting 350,000 inhabitants). For the selection of antihypertensives, the following ATC codes were considered: C02—agents acting on α-adrenergic receptors (methyldopa, clonidine, terazosine and doxazosine are the only agents reimbursed among C02 group), C03—diuretics (including minor, high ceiling and potassium-sparing diuretics, and their different combinations), C07—β-blockers, C08—calcium channel blockers, C09—agents acting on the renin–angiotensin system (including ACE inhibitors and ARBs).
Selection of patients
In order to recruit adult patients starting antihypertensive medication, we selected subjects aged 40 years and older who received their first prescription of antihypertensives between January and December 1999 without any prescription of antihypertensive agents in the previous year. Our cohort of patients was restricted to subjects permanently living in the area throughout the study period (from 1998 to 2002).
Data analysis
For each patient, we identified the date of the first prescription of antihypertensive agents and, based on all drugs prescribed on that date, we documented their starting regimen.
The prescriptions of each patient were analysed for 3 years after recruitment, and adherence to treatment was evaluated in terms of persistence during the years and in terms of daily coverage. Patients were defined persistent if they received at least one prescription of any antihypertensive agent in 2000, 2001 and 2002. Patients were defined covered when the amount of drugs received throughout the 3-year period was consistent with a daily treatment. To this purpose, we identified the minimal daily dose recommended for the maintenance therapy for each drug and we calculated the total number of minimal doses of each antihypertensive agent received by the patient during the year. Patients reaching at least 300 minimal doses were considered as covered, allowing a tolerance of 20% over the 12-month period.
Finally, the antihypertensive regimens received by each patient of the cohort during the whole period were analysed and switches to other antihypertensive regimens or addition of other therapeutic classes were identified.
The protocol was approved by the institutional ethics committee.
Results
A cohort of 6,043 subjects receiving their first antihypertensive treatment in 1999 was obtained. This cohort represented 3.3% of the population permanently living in the Ravenna area during the period of the study. The number of females in the cohort was higher than that of males (female/male ratio =1.2) reflecting the same proportion as in the general population (Table 1).
Initial treatment
Monotherapies with ACE inhibitors (n=1597; 26%) or calcium channel blockers (n=1126; 19%) were the most frequently prescribed regimens. Of the patients, 21% started with a drug combination regimen: 19% (n=1255) with a combination of two drugs and 2% (n=130) with a combination of three or more-drugs (Fig. 1). About three quarters of the two-drug combinations included a minor diuretic. Comparing prescriptions of antihypertensives in the Ravenna district with Italian data, the extent of prescription of the various antihypertensive classes appeared similar between the two populations (Table 2).

Distribution of different regimens prescribed by general practitioners (GPs) as initial treatment. *Two-drug combinations containing a minor diuretic having a very low prevalence of prescription (<0.5%) are added to the respective monotherapies: i.e. α-blockers+minor diuretics are included in the group of α-blockers, and calcium channel blockers+minor diuretics are included in the group of calcium channel-blockers. ** Mono, Combo and Triple mean monotherapies, two-drug combinations and triple or more combinations, respectively
The choice of β-blockers for the initial treatment decreased with age, from 22% in the 40- to 49-year old age group to 8% in the 70- to 79-year old age group. The reverse was true for calcium channel blockers (from 14% to 23%). In the oldest age group (80 years and older), the use of all types of diuretics sharply increased, whereas all the other antihypertensive classes decreased (Fig. 2).

Choice of initial treatment by age
Adherence to treatment
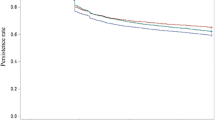
Of the patients, 18% received only one prescription throughout the 3 years; 13% received more than one prescription, but stopped antihypertensive medication during the first year; 69% were persistent during the second year and 60% also during the third year. In terms of coverage, only 34% were covered during the first year and 24% also during the second year. Only 20% of the patients were concluded to be covered throughout the 3 years (Fig. 3).

Three-year persistence and coverage of naive patients
Both persistence and coverage were found to be significantly higher in older patients (Table 3) with a Chi-square for trend =98.21 (d.f.=1; P<0.0001). Moreover, males were more adherent to the therapy than females.
Changes in antihypertensive regimen
Among persistent patients, 41% maintained the same antihypertensive regimen throughout the 3 years, 25% added other drugs to the initial treatment, and 34% switched to completely different regimens. Patients starting with ARBs maintained the initial regimen in a greater proportion (about 50%) than others, while those with diuretics, both minor and high ceiling, or complex regimens withdrew (53–67%) or changed the initial treatment to a greater extent (Fig. 4).

Three-year follow-up of patients grouped by initial regimen. *Combinations of α-blockers+minor diuretics are included in the group of α-blockers and combinations of calcium channel blockers+minor diuretics are included in the group of calcium channel blockers
Among the subjects who maintained their initial regimen during the 3 years of the study, less than 10% of those treated with diuretics (minor or high-ceiling) were covered. In contrast, the use of α-blockers or two-drug combinations without minor diuretics was associated with the highest coverage (>40%; Fig. 5).

Coverage in persistent patients receiving a constant regimen. *Combinations of α-blockers+minor diuretics are included in the group of α-blockers and combinations of calcium channel blockers+minor diuretics are included in the group of calcium channel blockers
Discussion
Our findings reflect the lack of convergence among guidelines on the drugs of choice for the initial treatment of hypertension and, more importantly, show a very low adherence to treatment over a 3-year period.
Almost half of the initial treatments observed in the present study were represented by ACE inhibitors or calcium channel blockers as single agent therapy. Such a finding reflects the overall ranking of cardiovascular drugs used in Italy, and it seems more related to the pharmaceutical market profile than to the adoption of any specific guideline in this area. As a matter of fact, this finding can be seen to be more consistent with the European guidelines, which allow doctors to choose from any drug class when starting an antihypertensive therapy, than with the US recommendations for hypertension, which indicate minor diuretics and β-blockers as the first choice for the initial treatment of uncomplicated patients. In our case, β-blockers and minor diuretics were prescribed in less than one quarter of the initial treatments, whereas 40% of the patients started antihypertensive medication with drugs that could be considered as second-line (ARBs or calcium channel blockers or α-blockers), according to the several authoritative sources [10, 19, 20]. However, if the British guidelines are considered, the drugs recommended as first choice represented almost 40% of initial treatments: in particular, 29% of 55-year-old and older patients received calcium channel blockers or minor diuretics, and 63% of the patients younger than 55 years received ACE inhibitors, ARBs or β-blockers.
The lack of information on diagnosis is a limit of our study, because the presence of compelling indications may well warrant the choice of drugs such as calcium channel blockers or ACE inhibitors as first line. We also acknowledge that the lack of diagnosis may have caused the inclusion of a few non-hypertensive patients in our cohort. However, hypertension is by far the most common indication for the use of these drugs. A questionnaire-based survey performed by us in 2002 on a representative sample of the Italian population [21] showed that hypertension largely represents the most common indication (73%) for the use of the drugs considered as antihypertensives in the present study (unpublished data). In that survey, about 20% of the patients received these drugs for other chronic conditions (i.e. angina and cardiac failure), and only less than 1% of the patients used the drugs for non-chronic indications such as oedemas. A small number of patients also received other cardiac drugs (nitrates and/or digitalis): they were prescribed more frequently than other patients calcium channel blockers or high ceiling diuretics or combinations of two drugs (different from minor diuretics). Therefore, if we assume that most patients starting antihypertensive treatment have uncomplicated hypertension, we can conclude that a large part of the initial treatment is performed with drugs that should be reserved for more troublesome situations.
In this study, we also evaluated adherence to treatment as a measure of appropriate drug use. If the information about both persistence and coverage was considered together, adherence in patients starting an antihypertensive treatment appeared very poor. Of the patients, 18% never received the second prescription, 11% discontinued the treatment within the first year, 16% followed an intermittent therapy discontinuing before the third year, 33% followed an intermittent therapy for many years and only 20% had a chronic daily treatment.
Adherence to treatment was found to be higher in patients also taking other cardiac agents (digitalis and/or nitrates), and this identifies subjects suffering from angina or heart failure: persistence increased slightly, whereas coverage throughout the 3 years was augmented by 50% (from 20% to 30%). In any case, these patients were a minority in the cohort and their patterns in terms of drug choice and adherence have only a minor, if any, influence on the overall findings.
In our study, persistence varies among drug classes. ARBs and the combinations of ARBs+minor diuretics had the highest persistence, followed by β-blockers and β-blockers+minor diuretics, and by ACE inhibitors and ACE inhibitors+minor diuretics, whereas complex regimens were associated with a very low persistence. The pattern observed by us is similar to that already described in other studies: generally, patients who were initially prescribed newer antihypertensive drugs (i.e. ARBs) were more persistent [22], in contrast to those starting with an old class or a complex regimen [23]. However, the low prevalence of ARBs in the initial treatment (4%) of hypertension must be kept in mind.
If we compare our results with those of Canadian and UK studies, we can conclude that in Italy minor diuretics are underused in the initial treatment of hypertension, whereas there is a marked and growing preference for agents active on the renin–angiotensin system [24]. In particular, in the UK, most patients received minor diuretics (more than 50%) as monotherapy or combined, and β-blockers ranked second (35%) [25]; likewise, in Canada many naive patients received minor diuretics (42%), with ACE inhibitors representing the second most prescribed regimen (32%) [26].
Adherence to antihypertensive medication is a matter of concern in health policy. Indeed, Jones et al. [25] and Caro et al. [26, 27] reported a persistence with a constant regimen of 41–49% after 6 months in the United Kingdom and of 46% after 4.5 years in Canada. However, Jones concluded that the continuation rate was low, no matter which drug was prescribed, whereas Caro speculated that the initial choice of an antihypertensive medication strongly influences adherence to treatments.
According to the published literature, there are two important factors associated with adherence to antihypertensive treatment [28]: drug tolerability and regimen complexity. Indeed, Bloom [22] and Marentette et al. [23] identified drug safety as the cause of the higher persistence in patients with newly diagnosed hypertension receiving ARBs rather than in those receiving ACE inhibitors or older classes. Complexity of the regimen has been identified as another possible cause of the poor adherence observed in actual practice [29]. More specifically, non-adherence to the treatment has been associated with the number of concurrent medications and therapeutic “turbulence” such as switches and additions. A few observational studies that directly investigated the relationship between regimen complexity and adherence to treatment showed that patients beginning therapy with multiple drug regimens were less likely to be adherent than patients initially treated with monotherapies (β-blockers, calcium channel blockers or ACE inhibitors). Also in this case, our findings are consistent with that hypothesis since we found a low persistence in patients with complex regimens (Fig. 4) and only 17% of the subjects were without changes in the regimen.
In conclusion, the lack of adherence to antihypertensive treatment is undoubtedly a matter of concern for public health and should be addressed with appropriate strategies. A better understanding of GPs’ prescribing habits and of their outcomes could assist in targeting educational interventions to improve the management of hypertension.
References
Anonymous (2004) The use of drugs in Italy—National report 2003
Amery A, Birkenhager W, Brixko P, Bulpitt C, Clement D, Deruyttere M, De Schaepdryver A, Dollery C, Fagard R, Forette F (1985) Mortality and morbidity results from the European working party on high blood pressure in the elderly trial. Lancet 1:1349–1354
Dahlof B, Lindholm LH, Hansson L, Schersten B, Ekbom T, Wester PO (1991) Morbidity and mortality in the Swedish trial in old patients with hypertension (STOP-hypertension). Lancet 338:1281–1285
Anonymous (1979) Five-year findings of the hypertension detection and follow-up program. I. Reduction in mortality of persons with high blood pressure, including mild hypertension. Hypertension detection and follow-up program cooperative group. JAMA 242:2562–2571
Anonymous (1982) The effect of treatment on mortality in “mild” hypertension: results of the hypertension detection and follow-up program. N Engl J Med 307:976–980
Anonymous (1991) Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the systolic hypertension in the elderly program (SHEP). SHEP cooperative research group. JAMA 265:3255–3264
Gueyffier F, Boutitie F, Boissel JP, Pocock S, Coope J, Cutler J, Ekbom T, Fagard R, Friedman L, Perry M, Prineas R, Schron E (1997) Effect of antihypertensive drug treatment on cardiovascular outcomes in women and men. A meta-analysis of individual patient data from randomized, controlled trials. The INDANA investigators. Ann Intern Med 126:761–767
Turnbull F (2003) Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively designed overviews of randomised trials. Lancet 362:1527–1535
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ (2003) In: 7th report of the joint national Committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 289:2560–2572
August P (2003) Initial treatment of hypertension. N Engl J Med 348:610–617
Cifkova R, Erdine S, Fagard R, Farsang C, Heagerty AM, Kiowski W, Kjeldsen S, Luscher T, Mallion JM, Mancia G, Poulter N, Rahn KH, Rodicio JL, Ruilope LM, van Zwieten P, Waeber B, Williams B, Zanchetti A (2003) Practice guidelines for primary care physicians: 2003 ESH/ESC hypertension guidelines. J Hypertens 21:1779–1786
Williams B, Poulter NR, Brown MJ, Davis M, McInnes GT, Potter JF, Sever PS, Thom SM (2004) British hypertension society guidelines for hypertension management 2004 (BHS-IV): summary. BMJ 328:634–640
Trilling JS, Froom J (2000) The urgent need to improve hypertension care. Arch Fam Med 9:794–801
Jones JK, Gorkin L, Lian JF, Staffa JA, Fletcher AP (1995) Discontinuation of and changes in treatment after start of new courses of antihypertensive drugs: a study of a United Kingdom population. BMJ 311:293–295
Casiglia E, Mazza A, Tikhonoff V, Pessina AC (2002) Population-based studies improve outcome in hypertensive patients. Am J Hypertens 15:605–608
Mancia G, Pessina AC, Trimarco B, Grassi G (2004) Blood pressure control according to new guidelines targets in low- to high-risk hypertensives managed in specialist practice. J Hypertens 22:2387–2396
Montanaro N, Vaccheri A, Magrini N, Battilana M (1992) FARMAGUIDA: a databank for the analysis of the Italian drug market and drug utilization in general practice. Eur J Clin Pharmacol 42:395–399
WHO Collaborating Centre for Drug Statistics Methodology (Norway) (2000) ATC index with DDDs
Messerli FH (2000) Implications of discontinuation of doxazosin arm of ALLHAT. Antihypertensive and lipid-lowering treatment to prevent heart attack trial. Lancet 355:863–864
Anonymous (2002) Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). JAMA 288:2981–2997
Motola D, Vaccheri A, Silvani MC, Poluzzi E, Bottoni A, De Ponti F, Montanaro N (2004) Pattern of NSAID use in the Italian general population: a questionnaire-based survey. Eur J Clin Pharmacol 60:731–738
Bloom BS (1998) Continuation of initial antihypertensive medication after 1 year of therapy. Clin Ther 20:671–681
Marentette MA, Gerth WC, Billings DK, Zarnke KB (2002) Antihypertensive persistence and drug class. Can J Cardiol 18:649–656
Degli Esposti L, Degli Esposti E, Valpiani G, Di Martino M, Saragoni S, Buda S, Baio G, Capone A, Sturani A (2002) A retrospective, population-based analysis of persistence with antihypertensive drug therapy in primary care practice in Italy. Clin Ther 24:1347–1357
Jones JK, Gorkin L, Lian JF, Staffa JA, Fletcher AP (1995) Discontinuation of and changes in treatment after start of new courses of antihypertensive drugs: a study of a United Kingdom population. BMJ 311:293–295
Caro JJ, Speckman JL, Salas M, Raggio G, Jackson JD (1999) Effect of initial drug choice on persistence with antihypertensive therapy: the importance of actual practice data. CMAJ 160:41–46
Caro JJ, Salas M, Speckman JL, Raggio G, Jackson JD (1999) Persistence with treatment for hypertension in actual practice. CMAJ 160:31–37
Payne KA, Esmonde-White S (2000) Observational studies of antihypertensive medication use and compliance: is drug choice a factor in treatment adherence? Curr Hypertens Rep 2:515–524
Monane M, Bohn RL, Gurwitz JH, Glynn RJ, Levin R, Avorn J (1997) The effects of initial drug choice and comorbidity on antihypertensive therapy compliance: results from a population-based study in the elderly. Am J Hypertens 10:697–704
Acknowledgements
We wish to thank the Local Health Authority of Ravenna, for supplying prescribing data. The study was supported by grants from the Regione Emilia Romagna and the University of Bologna. An institutional unrestricted grant was also received by Roche S.p.A.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Poluzzi, E., Strahinja, P., Vargiu, A. et al. Initial treatment of hypertension and adherence to therapy in general practice in Italy. Eur J Clin Pharmacol 61, 603–609 (2005). https://doi.org/10.1007/s00228-005-0957-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-005-0957-y